
Abstract
Objective:
Telehealth is increasingly used in urology, but few studies have evaluated how it can be integrated with urology face-to-face (FTF) encounters and primary care (PC). We describe the 5-year experience of a Veterans Affairs urology service that has incorporated telehealth into their patient care program.
Methods:
We performed a retrospective review of encounters from 2013 to 2018 in telehealth urology clinics. To examine the way telehealth and FTF visits were utilized together, the key components of care were defined for the evaluation of three common referrals: elevated prostate-specific antigen (PSA), microscopic hematuria, and obstructive lower urinary tract symptoms (LUTS). A random convenience sample of 20 patients from each condition was abstracted to describe the setting of care for each component over a 2-year period.
Results:
We reviewed 811 unique patients who had a total of 2,008 telehealth visits. The mean utilization of telehealth (2.48) and FTF (2.42) encounters per patient were similar. The most common reasons for referral to telehealth clinics were sexual dysfunction (26.8%), LUTS (20.6%), hematuria (15.0%), prostate cancer (13.3%), and an elevated PSA (12.1%). Thirty-six percent of patients were managed by telehealth alone; 64% were by a combination of telehealth and FTF encounters. Telehealth was often used in conjunction with PC and FTF visits to perform components such as the physical exam and procedures.
Conclusions:
Telehealth was utilized for a wide array of diseases and often used in conjunction with PC and urologic FTF visits to deliver complete care for the three disease states we evaluated.
Introduction
Telemedicine is increasingly being utilized in diverse clinical settings in hopes of improving access to care and improving the patient experience. Multiple modalities are currently available, including clinical videoconferencing, mobile applications, wearable devices, text messaging, and voice telephone. However, there is little information about how these telehealth technologies are integrated into care, especially in a surgical specialty such as urology.
We previously reported on the convenience and acceptability to patients of the urology telehealth program offered by the Veterans Affairs (VA) Greater Los Angeles Healthcare System (VAGLAHS). 1 Although telemedicine has been shown to be a successful tool in urology, which is well received by patients and physicians alike, few studies have described how telehealth visits can be combined with primary care (PC) and face-to-face (FTF) visits to deliver care in a real-world setting.
We describe our 5-year experience at the VAGLAHS with the utilization of telehealth technology to deliver urologic care, specifically in a general urology clinic and an erectile dysfunction education clinic. To analyze how PC, telehealth, and FTF encounters were combined, we examined the patient course through three common urologic referrals: elevated prostate-specific antigen (PSA), microscopic hematuria (MH), and obstructive lower urinary tract symptoms (LUTS).
Materials and Methods
Urology Telemedicine Program Structure
Telehealth encounters were performed between the tertiary West Los Angeles Veterans Affairs (WLA VA) Medical Center, and remote patient sites at two PC-oriented Community-Based Outpatient Clinics (CBOCs). The WLA VA is a tertiary medical center that offers comprehensive urology services. The CBOCs, which offer only PC augmented by limited nonsurgical specialty care, are in Santa Maria and Bakersfield, located 151 and 108 miles from the WLA VA, respectively. 1 During these encounters, a nurse and a clinical telehealth technician are available to assist the patient at the CBOC, while an attending surgeon or nurse practitioner from the WLA VA interacts with and evaluates the patient. Ultrasound bladder scanners are available at each CBOC, and the International Prostate Symptoms Scale (IPSS) survey can be administered and recorded by the nursing staff within the patient's electronic health record. All patients were seen and examined by their primary care provider (PCP) before the referral, and only these visits or PCP visits that specifically targeted follow-up needs for the urologic condition being evaluated were included in the analysis. Both new consults and active follow-ups can be seen in telehealth.
Patient Demographics and Diseases Evaluated
An Institutional Review Board waiver was obtained before performing this study. We used administrative data to evaluate new and follow-up encounters performed between September 2013 and January 2018. Patient demographics, including age at the initial telemedicine encounter, gender, race, and ethnicity were recorded. Visits to all urology telehealth clinics (three general urology clinics and one erectile dysfunction clinic) were assessed. Following the patient's initial telehealth encounter, the number of subsequent telehealth and FTF encounters were recorded. We used the primary International Classification of Diseases-9-Clinical Modification (ICD-9-CM) or International Classification of Diseases-10-Clinical Modification (ICD-10-CM) diagnosis code for the initial telehealth encounter to determine the primary urologic diagnosis. When the primary code was not a urologic condition or there was otherwise confusion, a chart review was performed to confirm the primary urologic diagnosis.
Descriptive Analyses of Common Referrals
To illustrate how telehealth modalities were integrated into the care of patients, we first defined the key elements of care for the evaluation of the three common referrals: elevated PSA, MH, and obstructive LUTS (Supplementary Table S1). Using ICD-9-CM and ICD-10-CM diagnosis codes (790.93 and R97.2 [elevated PSA]; 599.7, 599.72, R31.1, R31.2, R31.21, R31.29, and R31.9 [MH]; 600, 600.01, 600.9, N39.41, N40.1, and N40.3 [obstructive LUTS]), we identified a convenience sample of 20 randomly selected patients within each condition. Two authors (A.N. and N.S.) evaluated care within each group over a 2-year period following the initial referral to urology. Assessed components of care included laboratory tests, imaging, physical examination (P.E.), procedures, and setting of care.
Results
Demographics and Urologic Diseases Evaluated
There were 811 unique patients and 2008 telehealth visits (Table 1). The average age was 65.6 years and 98.3% (797/811) were male. Most patients were White (57.5%, n = 466), followed by African American (19.2%, n = 156) and Hispanic ethnicity (10.6%, n = 86). Thirty-six percent (292/811) of patients were managed by telehealth alone; 64% (519/811) were by a combination of telehealth and FTF encounters. Among this population of patients with at least one telehealth visit, there was a mean 2.48 telehealth encounters and 2.42 urology FTF encounters. The mean follow-up time was 29.45 months. The most common urologic conditions evaluated during the initial telehealth encounter (including both general urology and sexual dysfunction clinics) were sexual dysfunction 26.8% (217/811), LUTS 20.6% (167/811), hematuria 15.0% (122/811), prostate cancer 13.3% (108/811), and an elevated PSA 12.1% (98/811) (Table 2).
Demographic Characteristics of Patients Seen in the Urology Telehealth Clinics from 2013 to 2018
LUTS, lower urinary tract symptoms; PSA, prostate-specific antigen.
Definitions and Frequencies of Urologic Conditions Evaluated 2013–2018 in Urology Telehealth Clinics (Including General Urology and Erectile Dysfunction Clinics)
Descriptive Analysis of the Role of Telehealth in the Evaluation of Three Common Conditions
Elevated PSA
The mean age was 68.2 years and the mean PSA level was 7.13 ng/mL (Fig. 1 and Table 1). Patients had a mean of 2.75 telehealth encounters and 1.55 FTF encounters (Fig. 2). Telehealth was used to obtain 100% of the disease history, 0% of the PE, 38.2% of laboratories, and for 0% of procedures (Supplementary Table S2). The key component of the PE, the digital rectal exam (DRE), was performed by the PCP within the prior 6 months in 45% (9/20) of cases (Supplementary Table S3). Seventy percent (14/20) of patients had a DRE following the urology consult, of which two were done by the PCP at the urologist's request, nine were done at the time the patient presented for prostate biopsy, and three were done at a FTF visit when biopsy was not performed.

Flow chart demonstrating evaluation of 20 patients referred for an elevated PSA. DRE, digital rectal exam; PCP, primary care provider; PSA, prostate-specific antigen.

Mean number of visits conducted through telehealth versus face to face during the evaluation of 3 common urologic referrals for 20 patients: elevated PSA, microscopic hematuria, and LUTS. LUTS, lower urinary tract symptoms.
Twelve patients underwent prostate biopsy and ultimately 10 patients were diagnosed with prostate cancer. Of the eight patients who were not biopsied, four had stable PSAs when rechecked, two declined biopsy, and two were lost to follow-up.
Microscopic hematuria
The average age of the patients was 62.2 years, and all but one was male (Fig. 3 and Table 1). Patients had a mean of 1.5 telemedicine visits and 1.35 FTF encounters. Telehealth was used to obtain 100% of the disease history, 16.3% of laboratories, 50% of imaging, and 0% of procedures (Supplementary Table S2). Among all those seen for MH, the average number of red blood cells per high-powered field on urinalysis was 5. Seventy-five percent (15/20) of patients elected a full hematuria workup. Of the five who did not, two did not want to travel and three refused cystoscopy. No patients were diagnosed with bladder cancer.
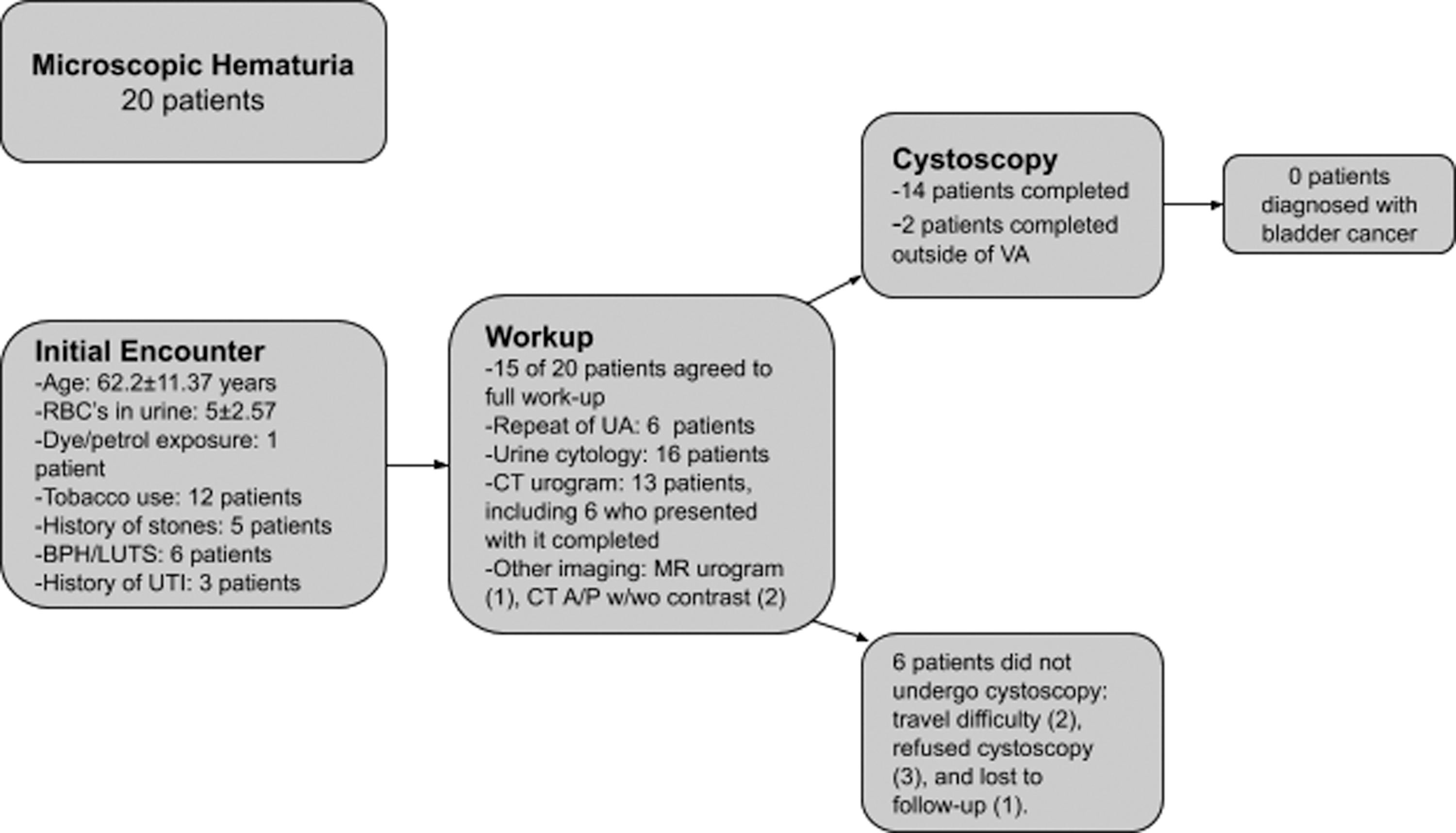
Flow chart demonstrating evaluation of 20 patients referred for microscopic hematuria. BPH, benign prostatic hyperplasia; RBC, red blood cell; UA, urinalysis; UTI, urinary tract infection; VA, Veteran Affairs.
Obstructive LUTS
The average age was 67.8 years, and patients had an average of 2.4 telemedicine encounters and 1.15 FTF visits (Table 1). Telehealth was used to obtain 100% of the disease history, 0% of the PE, 22.8% of laboratories, and 42.4% of procedures (Supplementary Table S2).
Thirteen unique patients underwent a genitourinary exam: eight in the prior 6 months by their PCP and seven during a FTF urology visit (Supplementary Table S3). The IPSS was administered by CBOC staff to eight patients during telemedicine encounters. The bladder scanner was used to estimate postvoid bladder volume in 17 unique patients, 14 by CBOC staff during telehealth encounters, and 7 during FTF visits. During subsequent urology FTF encounters, four had a uroflow, one underwent urodynamics, three had a cystoscopy, and one had a transurethral resection of the prostate. A majority, 78.6% (11/14) of medication changes (discontinuations or dose adjustments) and 92.3% (12/13) of medications initiated for LUTS were made during telehealth visits.
Discussion
In this model of integrating telehealth into three general urology clinics and one erectile dysfunction clinic, we found that the most common urologic conditions evaluated were sexual dysfunction (26.8%), LUTS (20.6%), hematuria (15.0%), prostate cancer (13.3%), and an elevated PSA (12.1%). Sixty-four percent (519/811) of patients who were seen in telemedicine were also seen FTF and the overall average of telemedicine versus FTF visits was nearly identical. These data compare similarly to a study of 376 unique incarcerated patients evaluated through telemedicine, in which 56% of them were eventually seen FTF. 2 Our analysis demonstrated that many patients were eventually seen FTF to perform components such as the urological PE, and to perform procedures (Supplementary Table S2). This highlights the role telehealth can play in the evaluation, as well as the long-term, nonprocedural aspects of follow-up of patients. It is worth noting that over a third of patients were seen entirely by telehealth suggesting an important role for telehealth in the triage of patients needing specialty care, and in the treatment of urology care that is not procedurally based.
This work also highlights the strategy of selectively working with PCPs to conduct the PE in the setting of telehealth to optimize patient convenience. For example, nine patients evaluated for an elevated PSA and eight patients evaluated for LUTS already had a urological PE completed by their PCP. Additionally, two patients evaluated for an elevated PSA were sent back to their PCP to perform the PE. This nontraditional approach to the PE was limited to situations in which both the urologist and PCP were comfortable with this approach. As clinically indicated, patients could be seen FTF in the urology clinic. In cases where specialist confirmation of the PE is not required, and the delivery model allows for partnership, this strategy could further facilitate delivery of specialty care to underserved areas.
In this series, telehealth visits helped providers triage the need for a physical exam, and to medically manage LUTS, as the majority of medication initiation or changes occurred in the telemedicine setting.
Telemedicine has been used in the postoperative setting for both patients who have undergone radical prostatectomy, as well as for pediatric urology patients. 3,4 These studies have demonstrated that telemedicine used in these settings is safe, associated with high-patient satisfaction, and has the potential to lower costs and save time. The Atlanta VA Medical Center uses telephone calls to gather clinical information for hematuria workups through a standardized algorithm, and then determines afterward whether a FTF examination is warranted. They determined that patients preferred the convenience of the visit, were highly compliant, and that it was performed expeditiously. 5 Although this is similar to the use of televideo visits that we used, relative advantages and disadvantages of the telephone versus video visits have not been examined for MH. WhatsApp, a mobile phone messaging application, has also been used to effectively assess the grade of hematuria for which patients presented. 6 Telerounding, through the use of rounding robots, mobile phones, or tablets, to provide remote urologic consultations has also been met with great patient satisfaction and allowed providers to connect with patients hundreds of miles away. 7 –9
A longstanding challenge to the widespread implementation of telemedicine has been the financial model of care delivery. As a truly comprehensive health care system, the VA model has long facilitated telehealth innovation. Payment for telehealth in the fee-for-service model continues to make progress. Thirty-six states currently have telemedicine parity laws that require private payers to cover telemedicine services at rates equal to those paid if the service was performed FTF. 10,11 Medicaid covers telemedicine services in most states, however, Medicare has more regulations, restricting care to patients who live in remote locations, and requiring patients to be seen at a facility while engaging in the visit.
Other remaining obstacles to the continued implementation of telemedicine include states adopting clinical practice rules with higher specifications for telehealth than FTF services such as prerequisites for a FTF assessment, or an established relationship or PE. 11 Some states also have laws that do not permit out-of-state care especially if the physician is not licensed to practice in that state, and other states require that a health care provider such as a registered nurse or physician be on the premises during a telemedicine visit.
The study has several limitations, including the potentially limited external validity of our investigation given that most health care settings do not operate under a financial model similar to the VA, have different information technology resources and coordination of care compared with the VA, and do not have predominantly male patient populations. However, recent health care policy changes are encouraging more widespread implementation of telehealth, and there is little reason to think that the gender of the patient would impact the use of telehealth in ways not attributable to the diseases being assessed. The frequency of sexual dysfunction in this study may have been skewed by inclusion from an erectile dysfunction-focused clinic, however patients with erectile dysfunction would have been seen in the general urology clinics if the more targeted clinic was not available. Another limitation is the possibility of errors in ICD coding, which may be more common in a health care system that does not submit a majority of its encounters to outside payers. This was a retrospective study and the analysis of specific urologic conditions was illustrated with sample sizes too small to make broad conclusions about efficacy and safety.
Conclusions
Telehealth was utilized for a wide array of diseases and was most often used in conjunction with PC and urologic FTF visits to provide care for three urologic disease states. Telehealth may be best seen as a flexible component of care delivery that can be used alone or in conjunction with the standard FTF visit, and that it can present new opportunities for collaboration with PC providers.
Footnotes
Authors' Contributions
A.N. conceived and designed the analysis, collected the data, performed the analysis, and wrote the article. N.S. supervised the project and contributed to the design of the analysis. L.K and R.B. contributed to the writing of the article. J.B.S. supervised the entirety of the project, including conceiving and designing the analysis, performing the analysis, and writing of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.