
Abstract
Objectives:
The main objectives of the study were to evaluate the level of patients' acceptance of teleconsultation (TC) and to define the ideal patient profile for this type of service. The secondary objectives were to estimate the impact in time and financial resources for the patient in relation to face-to-face medicine.
Materials and Methods:
This is a prospective, nonprobabilistic, and random sampling study using an uncontrolled selection process consisting of a 19-question survey for health care users in the general population, in which the patients' acceptance of TC was analyzed through the question: “If your doctor suggested that you have a video conference consultation, how attractive would the proposal be for you?”
Results:
Of the 400 patients, 73.8% were in favor of a TC service. The variables that were associated with the acceptance of TC were health care users who had previously purchased on the internet (odds ratio [OR] = 2.6 confidence interval [CI] 95% 1.31; 5.05) and whether they were willing to assume the economic cost for a TC (OR = 7.8 CI 95% 3.26; 18.6). In terms of face-to-face consultations per year, 50% of the patients spent 5 h (standard deviation [SD] 10.7) going to see the doctor, and on average they requested 8.9 h (SD 16.1) of time off work permission and assumed an economic cost of €29.8 (SD 82.9) on journey time.
Conclusion:
A high number of health care users accept the use of TC, and this percentage increases in patients who had previously purchased online and were willing to assume an economic cost for this service.
Introduction
Teleconsultation (TC) consists of conducting a medical consultation through a telecommunications system. Despite the absence of physical contact, TC via real-time videoconferencing is the optimal way for verbal and nonverbal communication between the patient and the doctor by using information technology and telecommunications.
It is believed that telemedicine (TM) and specifically TC can revolutionize health care, because location is no longer a barrier in different medical specialties. Clinical trials are currently being carried out for the protocolization of medical care for multiple acute and chronic diseases through TC, as is the case for Diabetes Mellitus, 1 –4 Emergencies, 5 –7 Palliative care, 8,9 Psychiatry, 10 Cardiology, 11 –13 Dermatology, 14,15 Pediatrics, 16 as well as nursing care. 17
For TM to improve the care of our patients, thus saving resources for institutions, professionals, and patients, we need to differentiate between three pillars: a patient with an adequate profile to be attended to through TM, a health professional with a profile suitable for exercise TM, and a clinical case at an optimal time of illness to benefit from the service. This study assesses patient acceptance for the use of TC in health care. A few studies that have evaluated patient opinion on TC services were found when reviewing the literature.
Materials and Methods
Study Design
We carried out a prospective, nonprobabilistic, and random sampling study by using an uncontrolled selection process consisting of a 19-question survey (Appendix Table A1) for health care users (HU) in the general population, in which the patients' acceptance of TC was analyzed through the question: “If your doctor suggested that you have a video conference consultation, how attractive would the proposal be for you?” This variable had five response options: “very attractive,” “quite attractive,” “somewhat attractive,” “not very attractive,” or “not at all attractive.” In the analysis of the results, the variable was dichotomized as “reluctant to TC”—including the “not very attractive” or “not at all attractive” responses—and as “favorable to TC”—including the “somewhat attractive,” “quite attractive,” or “very attractive” responses.
The secondary objectives were to define the ideal patient profile to consult for TC, to estimate the potential saving of resources in time and money in the use of TC in relation to face-to-face medicine, HUs' willingness to pay for TC, and the potential health improvements according to the HUs. The survey (Appendix Table A1) was conducted with 19 interrogative variables that analyzed information on sociodemographic aspects, use of the internet, health care visits in person, consumption of economic resources, time related to health, degree of acceptance, and confidence in TC. The survey was edited in the Google forms survey platform.
Scope of Study
Two methods were used to collect the data from the HUs. The first was in person through a surveyor in the waiting room of the outpatient medical–surgical consultations and emergency service in a tertiary-level hospital of the Autonomous Region of Madrid, Spain. The second was by sending the form online (email, WhatsApp).
Study Population
The inclusion criteria were people willing to fill out the form. Patients with impaired baseline or cognitive characteristics were excluded, in addition to those who did not want to fill out the form.
Statistical Analysis
The database was automatically generated through the Google forms survey platform by transferring the data to the Excel spreadsheet (Microsoft, Redmond, WA). In the descriptive study of the sample, the categorical variables are described by using their absolute and relative frequencies, and the numerical variables by using the mean and standard deviation (SD). To evaluate the degree of patient acceptance of TC, the variable was dichotomized as “reluctant” and “favorable to TC” (“If your doctor suggested that you have a video conference consultation, how attractive would the proposal be for you?”).
The results are shown for patients and companions as a favorable percentage for TC and a 95% confidence interval (CI). For the secondary objective of defining the ideal patient for the use of TC, it was believed that a patient is suitable for TC when the proposal to have a video conference consultation was considered as “somewhat attractive,” “quite attractive,” or “very attractive.” Hypothesis tests were performed to assess the statistical association between the stratification variables (reluctant vs. favorable to TC) and the explanatory variables.
The chi-square test or Fisher's exact test was used for categorical variables, if the expected frequency in any of the boxes was <5. In the case of numerical variables, when normality was assumed, a contrast was performed by using a Student's t test for independent samples. When normality could not be assumed, the contrast was performed by using the Wilcoxon nonparametric rank test. A logistic regression model with variables was proposed that reported a p-value <0.001 in the univariate analysis. To adjust the final model, the backward elimination strategy was used, starting from the maximum model. The results of the final model strategy were shown by means of odds ratios (ORs) and their corresponding 95% CIs. The calibration of the model was evaluated by using the Hosmer-Lemeshow test, and the discriminant power was assessed by means of the area under the receiver operating characteristic (ROC) curve.
The results of the patient suitability model are represented by a probability nomogram. For the rest of the secondary objectives—the estimation of the economic and time savings for the patients, the predisposition to assume the economic cost of the HUs for TC, and the definition of potential improvements in health care—the variables of interest have been described. The categorical variables are described by their absolute and relative frequencies, and the numerical variables are described by mean, SD, median, and the 25th and 75th percentiles. The analyses were performed by using the statistical software Stata/IC 14.1 for Windows.
Ethical Considerations
The study was approved by the Clinical Research Ethics Committee of the hospital where the study was carried out. The personal data of the patients were processed in accordance with the general data protection regulations in force in Spain. Participants provided verbal informed consent.
Results
Of the 467 questionnaires (Appendix Table A1) completed by the HUs, 400 were patients (Table 1) and 67 were companions. Overall, 73.8% (295) of the patients (Table 2) and 71.6% (48) of the companions found a TC service to be favorable ( Tables 3 and 4 ). The variables' age, internet user, having purchased on the internet, use of video conference applications, and the willingness to assume economic cost for a video conference consultation were associated in favor of a TC service with a degree of statistical significance (Table 5). In the multivariate analysis of the data, the two variables “having purchased on the internet” and “being willing to assume an economic cost for a TC” were associated with statistical significance to patient suitability for TC (Table 6).
Description of Patient Population
Media (SD).
SD, standard deviation.
Frequency of Patient Attraction to Teleconsultation
Frequencies of Patients Reticent and Favorable to Teleconsultation
CI, confidence interval; TC, teleconsultation.
Frequencies of Patient Companions Reticent and Favorable to Teleconsultation
Description of Patient Population Reticent Versus Favorable to Teleconsultation
Univariate analysis.
Patient Suitable for Teleconsultation
Univariate and multivariate analysis.
OR, odds ratio.
In terms of OR, the probability of being a suitable patient for TC was 2.6 times greater if the HU had previously purchased on the internet and 7.8 times greater if they were willing to assume the economic cost for a TC. Through these two variables, the probability of being a suitable patient for TC is represented in the nomogram (Fig. 1) with an area under the ROC curve of 0.72. The following is an example of calculating the suitable patient probability for TC in the Nomogram.
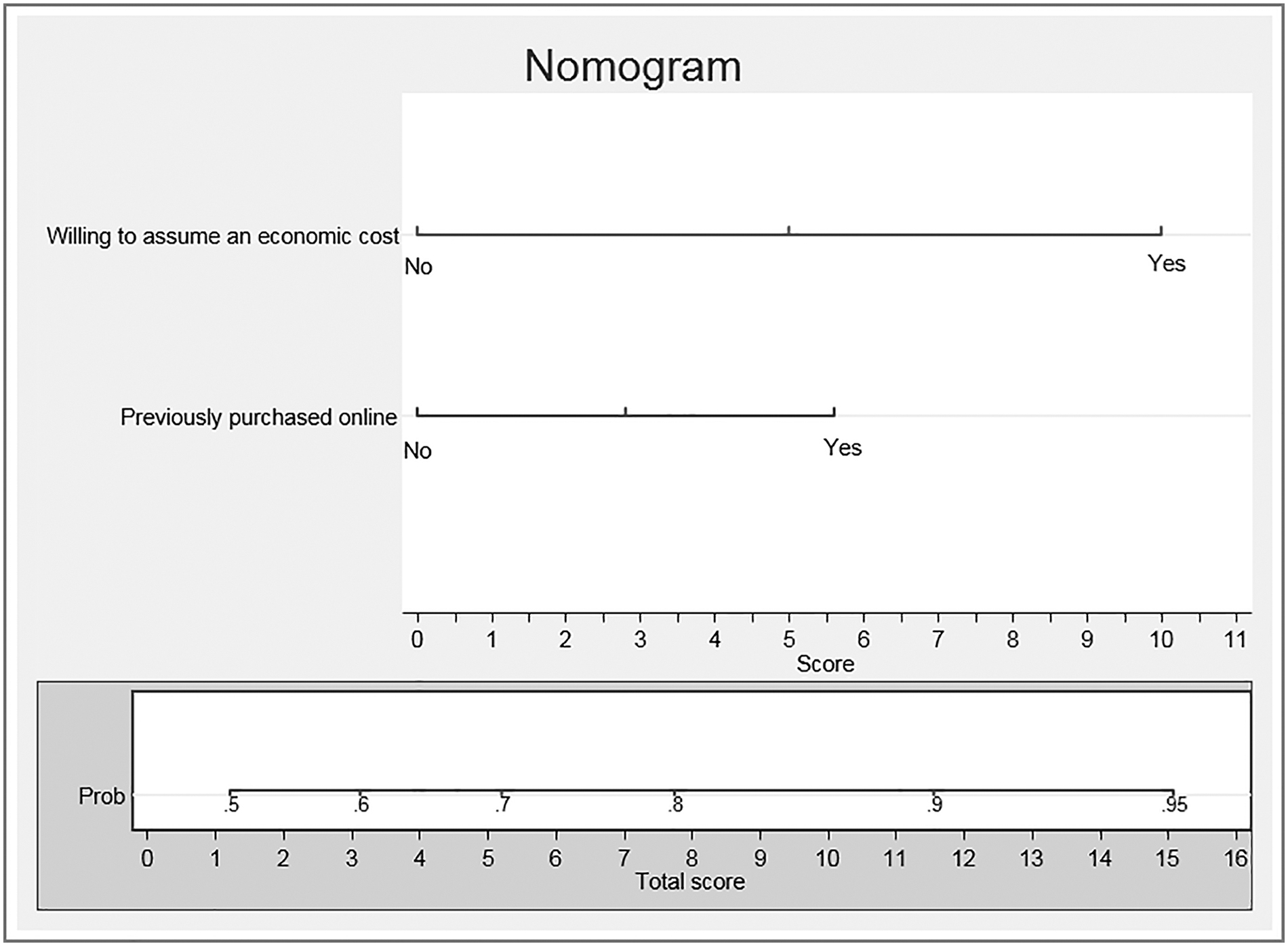
Nomogram. Patient suitability for TC. TC, teleconsultation.
Scenario 1: If a patient is willing to assume an economic cost for a TC, they get a score of 10 points, and if they had previously purchased on the internet, they get a score of 5.5 points. In this scenario, with a total score of 15.5 points, the probability that this patient is suitable for a TC service is >95% (Fig. 2).
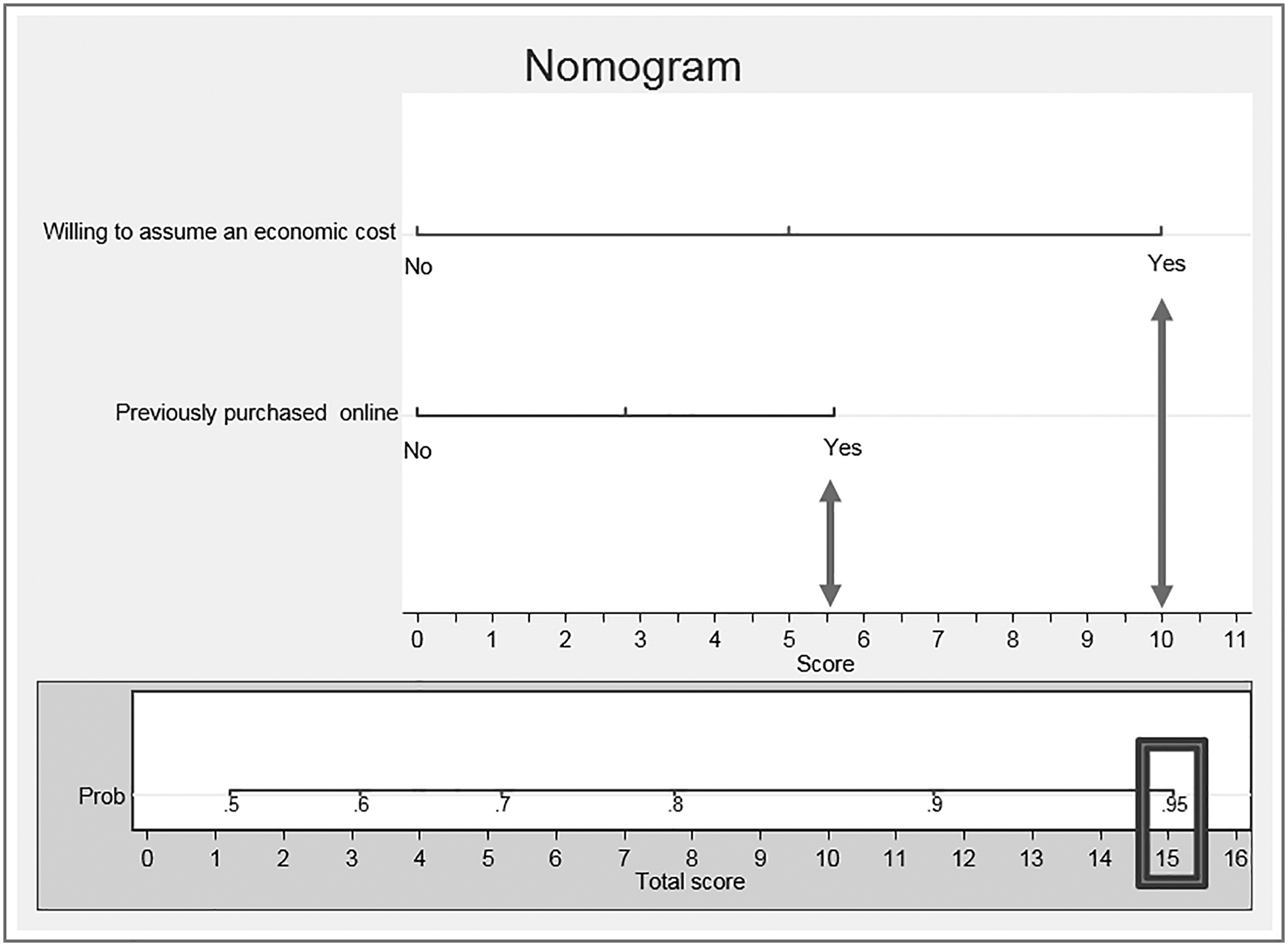
Scenario 1. People who would pay for a video conference and purchased online. According to this model, the probability of being a suitable patient for TC is >95%.
An analysis was performed of the 346 patients who had had a face-to-face medical consultation in the past year, to estimate the saving of resources related to health (Table 7). In terms of face-to-face consultations per year, 50% of the patients spent 5 h in going to see the doctor, and on average they requested 8.9 h of time off work permission and assumed an economic cost of €29.8 on journey time. Among the patients and companions favorable to the use of TC, 37.3% (110) and 10.4% (5), respectively, would be willing to assume a cost of more than €5 to have a TC ( Tables 8 and 9 ). Of the 400 patients, 59.2%, 21%, and 16% believed that time in the waiting room, bedside manner, and consultation time, respectively, should be improved (Table 10).
Description of Savings of Resources in Time and Money of Patients Who Had Attended a Face-to-Face Medical Consultation in the Past Year
Willingness of Patients to Assume the Economic Cost of a Teleconsultation
Willingness of Companions to Assume the Economic Cost of a Teleconsultation
Potential Improvements in Health Care According to Users
Discussion
This study shows how HUs accept TC and are favorable to its use—a suitable patient for TC can be described as one who is willing to assume an economic cost for TC and has previously purchased online. After reviewing the literature, no studies were found supporting the observation that describes the appropriate patient for TC according to the variables that have been analyzed. In their review article, Thijssing et al. describe how TC can lead to a saving in economic resources, travel time, and hours of absenteeism. It also includes the opinion of the patients who would like to see an improvement in the time in the waiting room and bedside manners from current health care professionals 16,18 —results reproduced in this study.
Telehealth (TH) is a tool that shows multiple forms of communication between professionals and HUs, with TC being the most common means. 19 This study describes how HUs are in favor of a TC service and how they mostly accept TC as a complementary tool for communication with their trusted doctor. According to the literature, chronic patients and their caregivers who require frequent medical follow-up, such as patients with Amyotrophic Lateral Sclerosis, accept and view TC favorably. 20 In chronic diseases, TC is comparable and not inferior to face-to-face consultations. Another example in favor of the use of TC in chronic diseases is the result of the TELEDIABE survey, in which all diabetic patients are interested in continuing in the project. 7,21 –24 McCall et al. describe an acceptance >70% among patients who suffer from depressive-anxiety syndrome and are treated through TC. 25 Ballestero et al. describe how an outpatient TM consultation is a satisfactory, agile, and useful resource to improve accessibility to the health service, in addition to quickly solving administrative procedures such as prescriptions. TC fulfills acute and chronic disease needs, and it also frees up more time, which can be dedicated to face-to-face consultation for people who visit the health care location. 26,27 Acceptance of TC also predominated in this study. These data are in agreement with a review article that shows how 95% of studies report that caregivers are satisfied and comfortable with TH, making patient care more efficient, effective, safe, and less stressful. 28,29
It is complex to evaluate the cost savings as a result of TH in the current public and private health care systems due to the heterogeneity of the patients' health problems and their various health care needs. 30 The different authors who have boldly decided to take this path have the opinion that, although there are no reliable economic studies because they take a long time to carry out, those patients who obtain the benefits of TH would be prepared to pay for the service. 31 In future cost-effectiveness analyses, the TH visits described as not inferior to face-to-face consultations will be analyzed, and each specific clinical case must be taken into account, such as emergency medicine where the only opportunity for health care is through TH. 32
This study's description of cost savings, time off work permission, and patient travel agrees with what is written in the literature given that TH decreases the number of referrals or hospital visits (40–74%), 7,33 in addition to improving the coordination during the disease process when used as triage. According to the data available, the average annual savings in travel amounts to €29.7 and is consistent with the TELEDIABE survey, which estimates an average savings of €80 per medical visit. This saving is described as most significant in populations with geographic dispersion and limited resources such as Oxaca, which allocated 52% of health expenses for transportation in 2014. 31,34 Some studies describe how TC leads to a cost saving of at least 10–18% on face-to-face medicine. This saving could be for patients, health institutions, and/or health insurance. 35 –37
TC is described as a health tool that is likely to be cost-effective. 38,39 This study describes an average annual saving of 10.7 h of journey time and 8.9 h of work leave. This is also supported by TELEDIABE data, which estimates 115 ± 86 min as the saving time for medical TC compared with face-to-face medical visits. 21 Regarding the willingness of the HUs to assume economic cost, according to the data available, 37% of patients and 10% of companions are willing to pay more than €5 to use a TC service. It is described in the literature how the elderly and those HUs who have to travel to see the doctor may be predisposed to assume economic costs. Lin et al. describe how the average cost per patient and visit was $12.59 in their integrated health service, 40,41 and Fuertes-Guiró et al. calculate how the cost of each teledermatology consultation is €29.25 with a cost/min of €3.8. 40
One of the aspects of the respondents' health care to improve was the time spent in the waiting room, which is consistent with the literature since waiting time has a negative effect on patient satisfaction with the health service. This waiting time even affects the way in which patients perceive the health care professional and their confidence in their capacity to solve problems. According to Xie et al., on average, 90% of the time that patients are in the hospital, they are waiting. 2
Assuming that the patients interviewed are not different from the general population, this study presents limitations for the generalization of the results, such as the fact that the number of nonrespondents who declined to carry out the survey is unknown and the fact that the HUs responded to the survey can lead to the assumption that they had a certain predisposition to collaboration. A questionnaire that was short and quick-to-answer was chosen to prevent HU fatigue, although as the interviewer was young, selection biases may have unconsciously incurred. The survey is not a validated questionnaire and is the result of the authors' scientific curiosity to know about certain specific aspects of TH; therefore, the data from this pilot study may contain biases specific to the method used. The results are applicable to a common population and hospital environment, but they are not generalizable.
For this reason, the internal validity of this study cannot be assured. Another limitation could correspond to the fact that the interviewees were waiting in the waiting room and knew that a doctor would attend to them in person in the next hour. In addition, the fact that they were respondents with technological experience who were accustomed to the use of technology could be significant. Regarding costs, the uncertainty of whether people have double public and private health care does not allow the profile of the patient willing to assume the cost for a TC to be known more precisely, since it can be hypothesized that the public HUs are more reticent to disbursement.
A final limitation in this study is that health outcomes are not described and there is more focus on the aspects of accepting TC and saving resources associated with face-to-face medicine. This questionnaire can be a guide for future economic studies and even for the selection of potential patients.
Conclusions
A large number of the HUs accept and are favorable to the use of TC, whereas there are also HUs willing to assume economic cost for TC services. Being willing to assume an economic cost for a TC and having previously purchased on the internet are variables associated with the probability that patients are suitable for TC. TC takes the health service to the place where HUs are located and it is useful in two situations: when there is no other possible alternative, such as in space, during catastrophes, and in areas with wide geographic dispersion; it is also a complementary tool for health services such as in chronic diseases that require hyper-frequentation of the health services and of the triage of acute diseases.
TC saves economic resources and time generated by the journey to the face-to-face medical visit, while also reducing the time off work that patients must request to go to see the doctor. TH is currently in growth and the main future challenges are policies, infrastructure, human resource training, patient education, protocolization of diseases by scientific societies with the evaluation of results of cost-utility, cost-efficiency, cost-effectiveness, transaction costs, the expectation of utility, 35,36 the secondary effects, and mortality derived from its use. It is important to highlight that this is currently the ideal moment for the complete development and implementation of TH, since according to the WHO Mobile Health, 85% of the world population has a Wi-Fi network.
Footnotes
Acknowledgments
Thanks are due to Oscar Bailly Bailliere, Gianluca Stamerra, PhD, and Tomas Curbelo for their contribution in the process of preparing the form and collecting the data; Carmen Rosa del Mar Rodríguez, PhD for her contribution to the bibliographic search; and David Pugh Spanish English Translation: david.pugh@theenglishprojectcentre.com.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Appendix
Appendix Table A1. Level of Patient Acceptance of Teleconsultation
1. Gender
Male
Female
2. Are you a patient or a companion?
Patient
Companion
3. Date of birth
Day
Month
Year
4. What type of internet user do you consider yourself to be?
I do not use the internet
0
to
5
Expert
5. Have you ever bought anything on the internet?
Yes
No
6. Do you use video conferencing applications such as Skype, Hangout, or Facetime?
I do not know what it is
I know what it is, but I do not know how to use it
I have used it on occasions
I use it several times per year
I use it frequently
7. During the past month, how many times have you visited your family doctor?
Free numbering
8. How many times have you visited your family doctor during the past 12 months?
Free numbering
9. How satisfied are you with the service offered by your regular doctor?
Not very
1
to
5
Very
10. What would improve about the service offered by your regular doctor? Choose two
I would increase the time in the consultation
I would improve the bedside manner
I would reduce the time in the waiting room
The consultation should be closer to my home.
Parking availability.
11. What medical specialty do you need a consultation for today?
Free text
12. How long does it usually take you to go to the doctor's from the time you leave until you return home? (in hours)
Free numbering
13. How many minutes does the consultation usually last? (in minutes)
Free numbering
14. How much money does it cost you to go to the doctor's and return home? Consider taxi, petrol, parking, public transportation, etc. (in Euros)
Free numbering
15. How many working hours do you have to ask to take off to see the doctor? (in hours)
Free numbering
16. What price would you be willing to pay if your doctor came to visit you at your home or office? (in Euros)
Nothing
20–30
30–50
50–70
70–100
17. If your doctor offered you a video conference consultation, how attractive would this proposal be to you?
Not at all attractive
1
to
5
Very attractive
18. What price would you be willing to pay to have a video conference consultation?
Nothing
5–10
10–20
20–30
30–40
19. Having had the consultation with your doctor, do you think that you could have had the consultation by video conference directly from your home?
Yes
No