
Abstract
Background:
Telepharmacy services are expected to have an important role in increasing access of patients to pharmaceutical care and reducing potential dispensing errors in community pharmacies.
Objective:
To assess the predictors for effective telepharmacy services on increasing access of patients to care and reducing dispensing errors in community pharmacies.
Method:
This is a prospective study carried out for 4 months in 52 community pharmacies across the United Arab Emirates (UAE) using disguised direct observation. Multivariable logistic regression was used as a tool to predict factors associated with effective telepharmacy services in improving dispensing safety and increasing access of patients to pharmaceutical care. Data were entered and analyzed using the Statistical Package for Social Science (SPSS) software version 26.
Results:
Pharmacist recommendations related to COVID-19 at pharmacies with telepharmacy (n = 63,714) versus those without remote services (n = 15,539) were significantly more likely to be (1) contact the nearest testing center (adjusted odds ratio [AOR] = 7.93), (2) maintain home quarantine (AOR = 5.64), and (3) take paracetamol for fever (AOR = 3.53), all were significant results (p < 0.05). Rates of medication dispensing errors (MDEs) and its subcategories, prescription-related errors, and pharmacist counseling errors across pharmacies with telepharmacy versus those without remote services were (15.81% vs. 19.43%, p < 0.05), (5.38% vs. 10.08%, p < 0.05), and (10.42% vs. 9.35%, p > 0.05), respectively. However, pharmacies with telepharmacy were more likely to include wrong patient errors (AOR = 5.38, p < 0.05).
Conclusions:
Telepharmacy can be used as a tool to reduce the burden on the health care system and improve drug dispensing safety in community pharmacies.
Introduction
The effects of coronavirus disease 2019 (COVID-19) on public health and health care systems have been devastating. 1 A tremendous humanistic and monetary loss was suffered worldwide. 2 Furthermore, COVID-19 has caused the health care systems of both developed and developing countries to be at the edge of collapsing. 3 Therefore, several nations combated the COVID-19 by implementation of restrictive measures including health quarantine, early diagnoses, and infection control measures. 4,5
In this regard, telemedicine, which is the provision of remote health care services using information technology tools such as smartphones, telephones, and mobile wireless devices, has achieved much more attention during the pandemic since it reduced the risk of COVID-19 transmission by minimizing in person contact among individuals. 6 –8 This includes telepharmacy, which refers to providing remote pharmacist services, with a spatial distance between the pharmacist and the patients as the consumers of health services. 6,9 The effectiveness of telepharmacy was demonstrated as a mean to prompt asthma control, 10 and a tool to reduce adverse drug events in hospitals. 11 However, no significant difference in dispensing error rates across pharmacies with and without remote services was reported. 12
With COVID-19 invading the world, many countries have legally expanded the role of community pharmacists to involve communicating with patients and costumers remotely using telepharmacy tools including virtual consultation, social media, and home delivery of medicines. 5,13 –15 The United Arab Emirates (UAE) is one of the first countries in the Middle East to implement these services, particularly during the outbreak of COVID-19. 16 The implementation of telepharmacy assists in expanding the role of pharmacists in the emergency response to include improving the awareness of the public toward COVID-19 symptoms and refer them to the appropriate health care facility for testing and provide necessary information to reduce the spread of this virus in community. 9,17 Moreover, consulting the public on medication use, adverse events, and adherence are potential benefits of remote pharmacist interventions. 18,19
However, the optimum conditions to operate such services are still unknown. More specifically, the potential factors to maximize the benefits of these services and reduce its drawbacks have not been examined. Therefore, this study predicts the factors associated with effective telepharmacy services and anticipates the weaknesses that may cause harm to patients or wasted resources.
Aims
This study aimed to evaluate the predictors for effective telepharmacy services by exploring factors associated with pharmacist interventions and dispensing errors in community pharmacies.
Method
DESIGN
This is a prospective observational study conducted for 4 months (March 2020–July 2020) in community pharmacies in the UAE during the COVID-19 outbreak. The research team conducted a disguised direct observation to collect data related to pharmacist interventions and dispensing errors across pharmacies with and without telepharmacy services. The study was approved by The Research Ethics Committee at the University of Sharjah.
SAMPLE SIZE CALCULATION
G*Power software 20 was used for sample size calculation (power = 0.8, α ≤ 0.05, effect size = 0.8). We decided to include 52 community pharmacies (26 for each group). Proportionate random sampling was used as sampling technique to enroll pharmacies from different geographic regions in the UAE: 16 pharmacies were included from Abu Dhabi, 21 pharmacies from the northern region, and 15 pharmacies from the central region. We invited >100 pharmacies to participate: 43 rejected to participate and 8 dropped out (Fig. 1).

The flow of the study.
CHARACTERISTICS OF PHARMACIES
The pharmacies included in this study were randomized into test (with telepharmacy) and control (without telepharmacy) groups. Both groups were not operating electronic patient record, automated dispensing machines, or electronic prescribing system (Fig. 2). Pharmacies with telepharmacy services utilize the available tools, such as videoconferencing and home delivery of medications to deliver their services to patients such as filling prescriptions, medication reviews, patient counseling, and home delivery of medications. 21
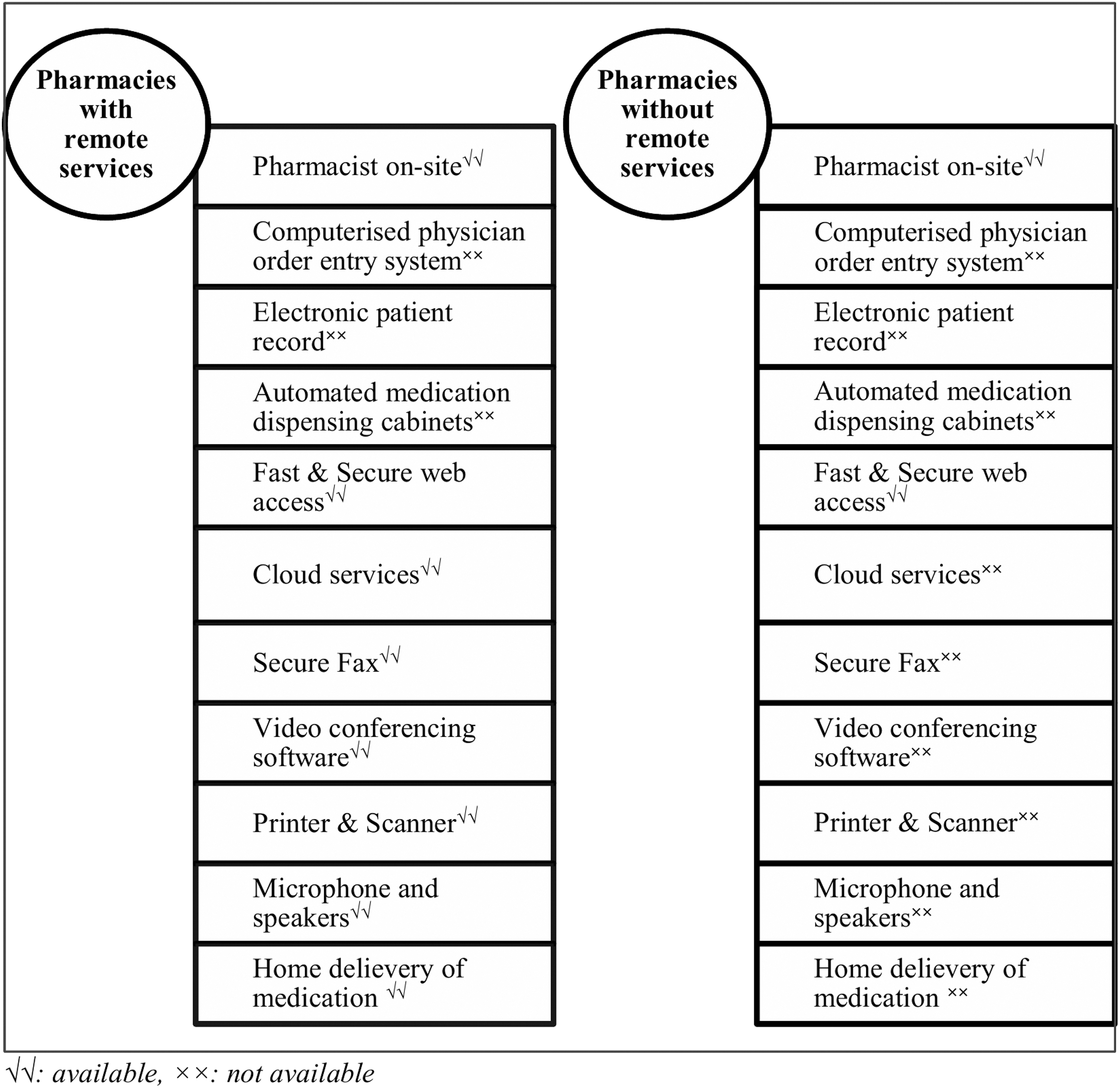
Characteristics of the included community pharmacies.
DISPENSING ERRORS
The definitions of dispensing errors and categories were adopted from a previous study that examined dispensing errors in community pharmacies in the Middle East. 22 A dispensing error was defined as “…any unintended deviation from an interpretable written prescription or medication order. Both content and labeling errors are included. Any unintended deviation from professional or regulatory references, or guidelines affecting dispensing procedures, is also considered a dispensing error” (Table 1).
Dispensing Error Classification
CASE DEFINITION FOR COVID-19
To document access of COVID-19 probable and confirmed patients to pharmaceutical services, the study adopted criteria for COVID-19 case classification based on the Centers for Disease Control and Prevention 23 and European Centre for Disease Prevention and Control. 24
DATA COLLECTION
The research team filled a data collection form, which was developed to include detailed information about prescriptions, pharmacist interventions, and dispensing errors. The data collection was carried out each day from 9:00 am to 5:00 pm. The main researcher reviewed and confirmed the collected data at the end of each research day. The research data collectors (16 licensed pharmacists) were recruited and trained on dispensing safety of medications, COVID-19–related recommendations, and data collection techniques.
DATA ANALYSIS
The data were entered and analyzed with Microsoft Excel (Redmond, Washington) and the Statistical Package for Social Science (SPSS) version 26. To assess the determinants of effective COVID-19–related recommendations and potential dispensing error types with community pharmacy status but with or without remote services (dependent variable of interest), multivariable logistic regression analyses were used. Descriptive results are presented as proportions (%) with confidence intervals (95% CIs), whereas logistic regression results are presented as adjusted odds ratios (AORs) with 95% CI. Statistical significance was considered at p-value <0.05 (with a confidence limit at 95%).
Results
Community pharmacies in the test group (with telepharmacy) provided care to 6,371 probable and 1,074 confirmed cases of COVID-19 compared with 1,213 and 33, respectively, in the control group. Pharmacies with telepharmacy services provided 63,714 COVID-19–related recommendations compared with 15,539 in the control group. Most of these recommendations were use face mask, frequent washing, take vitamin C, and take paracetamol for fever.
The incidence of dispensing errors in pharmacies with telepharmacy, 15.8%, was significantly lower than that reported in the control group, 19.43%. Error rates based on prescriptions and based on pharmacist's prescribing across pharmacies with and without telepharmacy were 5.38% versus 10.08% and 10.42% versus 9.35%, respectively.
There were significant differences between pharmacies with telepharmacy (n = 63,714) services versus pharmacies without remote services (n = 15,539) for the COVID-19–related recommendations (Table 2). Take paracetamol for fever (AOR = 3.53; 95% CI, 2.89–5.44; p < 0.05), maintain home quarantine (AOR = 5.64; 95% CI, 4.77–7.97; p < 0.05), eat healthy food (AOR = 5.49; 95% CI, 3.56–8.92; p < 0.05), contact the nearest testing center (AOR = 7.93; 95% CI, 5.47–11.27; p < 0.05), and contact the nearest medical center (AOR = 3.34; 95% CI, 2.70–3.99; p < 0.05) recommendations each versus keep social distancing were significantly more likely to be associated with test group pharmacies versus control group pharmacies (without telepharmacy). However, use of face mask, gloves, and frequent washing (AOR = 0.71; 95% CI, 0.44–0.90; p < 0.05) versus keep social distancing was significantly less likely to be associated with test group pharmacies versus control group pharmacies. Take vitamin C, stop smoking, keep self-isolation, avoid nonessential traveling, and call emergency recommendations each versus keep social distancing were not significantly different across pharmacies with and without remote services (p > 0.05).
Association of COVID-19–Related Recommendation Categories (n = 79,253) With Pharmacy Status (With vs. Without Remote Services)
Bold p Values are considered significant.
Multivariable logistic regression, where probability of each recommendation category was modeled for pharmacy status (with remote services [n = 63,714] vs. without remote services [15,539]).
p Value is not significant.
The logistic regression (Table 3) indicated that wrong patient (AOR = 5.38; 95% CI, 3.91–6.42; p < 0.05) versus wrong quantity was more likely to be associated with test group pharmacies versus control group pharmacies. However, wrong drug (AOR = 0.62; 95% CI, 0.38–0.81; p < 0.05) versus wrong quantity was less likely to be associated with test group pharmacies versus control group pharmacies.
Association of Dispensing Error Types (n = 12,471) With Pharmacy Status (With vs. Without Remote Services)
Multivariable logistic regression, where probability of each MDEs type was modeled for pharmacy status (with remote services [n = 7,908] vs. without remote services [4,563]).
p Value not significant.
MDEs, medication dispensing errors.
Discussion
To our knowledge, this study is the first study in the world to investigate the predictors for effective remote pharmacist interventions on COVID-19 patients and dispensing safety of medicines using a disguised direct observation as a tool for data collection.
The literature has shown that the digital infrastructures in Spain 25 and Italy 26 were unable to combat the consequences of the national lockdowns. Their implementation of telepharmacy services was limited due to the poor coordination with primary care and community pharmacists.
Historically, telepharmacy services were adopted to increase access to care in rural areas in the United States, 27 –29 Australia, 30,31 and to some patient groups in Spain and Denmark. 32,33 The goals of these experiences were to guarantee adequate health care services to patients, time saving, and improve patient satisfaction. In Egypt, a telepharmacy model was established to enhance the pharmacists' role in pediatric oncology and improve medication safety by educating patients about pulmonary diseases, specifically asthma and chronic obstructive pulmonary disease. 10,34 –36
The effectiveness of telepharmacy services were evaluated by examining the rate of dispensing errors, 37,38 by documenting number and nature of pharmacist interventions, 29 or by demonstrating the saving of time and staff for more quality-enhancing initiatives. 39,40
The findings of this study suggest a potential role for pharmacists in the emergency response to COVID-19. This is in line with the findings of Adunlin et al., 9 about potential role of community pharmacists in the response to the COVID-19 outbreak.
In addition, the findings of this study indicated that take paracetamol for fever, maintain home quarantine, eat healthy food, and contact the nearest medical center recommendations each versus keep social distancing were significantly more likely to be associated with test group pharmacies versus control group pharmacies (without telepharmacy). The plausible explanation is that telepharmacy provides more comfortable environment to the pharmacists to counsel patients without risk to get the virus.
In terms of evaluating error types, we found wrong patient errors were more likely to be associated with pharmacies operating remote services. This could be attributed to lack of electronic patient records and poor coordination between the pharmacist on-site and the delivery team. Wrong drug (AOR = 0.62; 95% CI, 0.38–0.81; p < 0.05) versus wrong quantity was less likely to be associated with test group pharmacies versus control group pharmacies.
This study highlights the capacity of remote pharmacist interventions to increase access of COVID-19 probable and confirmed patients to the care they need, and thus reduce the burden of the pandemic on health care system, and improve medication dispensing safety by reducing MDE rates. The UAE health authorities were the first in the region to regulate telemedicine and telepharmacy services on a national scale. These efforts might be the reason for the general controlled situation in the country. Medication safety-based research is rare in the Arabic region; most of the previous studies were conducted in hospital settings to document prescribing safety in the emergency departments 41 or the role of clinical pharmacists in reducing prescription-related errors. 42
This study had many limitations: (1) each community pharmacy operates nearly different system for medication dispensing, thus bias could be induced due to the variation, (2) due to lack of time and avoiding close personal contact with the staff and the patients, the main outcomes of this study may be underestimated, (3) the rate of acceptance for pharmacist interventions was beyond the scope of the study due to practical reasons, (4) we were unable to determine the impact of missing information on the accuracy of our findings, and (5) outcomes such as factors associated with error severity, causes, cost analysis, and channels of medicine delivery were unexamined in this study. Reasons for not addressing this issue were practical (insufficient data collectors), participant based (pharmacists refused to participate), and COVID-19–based reasons (avoiding close contact with the patients).
To sum up, this study provides high-quality evidence of the most important factors associated with telepharmacy implementation in community pharmacies in the UAE. These findings can service as national reference to maximize benefits of these services and implement corrective actions for the drawbacks.
Conclusions
Significant differences exist between pharmacies with and without remote services based on types of recommendations, interventions, and errors documented. Wrong patient errors are more likely to be documented in remote telepharmacies. As such, pharmacists in these settings must be cognizant of this fact and use extreme diligence when working in a telepharmacy setting.
Footnotes
Authors' Contributions
All authors have contributed to all parts of the research, including conceptualization, literature review, study design, research pharmacist recruitment, data analysis, and article preparation and review.
Acknowledgments
We thank the University of Sharjah for facilitating our research. We also thank the community pharmacists for their efforts and cooperation.
Ethics Approval
The study was approved by The Research Ethics Committee at the University of Sharjah.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.