
Abstract
Background:
Telemedicine use has expanded substantially in recent years. Studies evaluating the impact of telemedicine modalities on downstream office visits have demonstrated mixed results.
Introduction:
We evaluated insurance claims of a large commercial payer, Blue Cross Blue Shield of Michigan (BCBSM), to assess the frequency of follow-up visits following encounters initiated via telemedicine versus in-person.
Materials and Methods:
We used the BCBSM claim-level data set (2011–2017) to assess encounters in the following places of service: hospital outpatient, doctor's office, patient's home, or psychiatric daycare facility. We identified the primary diagnostic category for 30-day episodes of care using clinical classifications software (CCS) and multilevel clinical classifications software (ML-CCS). Our intervention group consisted of episodes initiated via telemedicine; our control group consisted of episodes initiated in-person. Our primary outcome was the percentage of 30-day episodes with a related visit (encounters occurring within the same period and CCS categories) across CCS categories. Our secondary outcome was the mean related visit rate.
Results:
The final data set included 4,982,456 patients and 68,148,070 claims, of which 53,853 were telemedicine related. Many episodes did not have related visits (the mean related visit rate was 16%). Telemedicine visits had a higher frequency of related visits across all CCS categories.
Discussion:
Episodes of care initiated via telemedicine more frequently generate related visits within a 30-day period. This increased health care utilization could represent excessive care or could reflect expanded access to care.
Conclusion:
Further research should explore the cause of this increased utilization and potential unintended consequences.
Introduction
Telemedicine use has expanded substantially over the past decade. Mehrotra et al. found that telemedicine visits increased 25% and 52% every year for the past decade in Medicare and among commercially insured patients, respectively. 1,2 Additionally, as of 2017, more than three-quarters of hospitals have implemented telehealth systems in some capacity. 3 A number of factors drive telehealth adoption, including growing evidence that demonstrates how telehealth can be used effectively for a variety of medical conditions, 4,5 and reduced barriers to implementation, specifically regarding reimbursement for care provided via telemedicine. 6
However, the notion that telemedicine visits are direct substitutes for in-person visits is not well supported by evidence. Existing studies that compare telemedicine with in-person care focus on quality or value metrics over the duration of one or multiple visits, whereas few studies have evaluated the downstream impact of a telemedicine visit on overall utilization of health care during an episode of care. An episode of care is defined as a window of time (e.g., 7, 14, and 30 days) during which an acute medical condition typically resolves. For instance, if a patient develops an upper respiratory infection, her episode of care may last approximately 1 week and may include one or more interactions with the health care system (e.g., office visit, laboratories, urgent care visit). There is a critical need to understand the “substitutability” of telemedicine visits to estimate the full impact of telemedicine on health care spending.
On one hand, if telemedicine is found to be an effective substitute for in-person care, its widespread adoption may either keep health care spending the same or reduce health care spending if the telemedicine visits are proven less costly than those performed in-person. However, if telemedicine is not a viable substitute for in-person care, and telemedicine visits do not eliminate the need for in-person visits, then health care spending may increase with telemedicine use. The latter scenario can occur if telemedicine evaluation cannot adequately resolve medical issues with the same efficiency of in-person visits, as well as if clinicians conduct telemedicine visits more frequently than in-person visits. Past research has demonstrated that the number of related visits is one of the most influential factors affecting the total cost of treating a condition. 7
Prior investigations into the impact of telemedicine modalities on downstream office visits and utilization of health care resources (e.g., antibiotics) have found mixed results. 8,9 These studies are limited by the fact that they evaluate asynchronous messaging (i.e., e-visit) rather than live, two-way audiovisual telemedicine. We build on the work in this area by examining insurance claims for a large commercial payer in Michigan to determine how often patients follow up for related care within 30 days. We assess whether follow-up rates differ between episodes of care initiated via telemedicine versus in-person care. By virtue of this approach, we will gain a deeper understanding of whether telemedicine services are a direct substitute for or expansion of in-person care.
Materials and Methods
Data SET
We used Blue Cross Blue Shield of Michigan (BCBSM) claim-level data sets from 2011 to 2017. We included evaluation and management procedure codes with the following places of service: hospital outpatient, doctor's office, patient's home, or psychiatric daycare facility. We identified telemedicine encounters according to the policies used by BCBSM. 10,11 We removed duplicated claims, claims with invalid national provider identifiers, and patients whose first and last claims were within 30 days.
Defining Related Visits
For each 30-day episode of care, we identified the primary diagnostic category using both the clinical classifications software (CCS) and the multilevel clinical classifications software (ML-CCS). 12,13 We excluded episodes that did not belong to any CCS category nor to the claims in CCS categories 48, 56, 58, 238, and 2,601–2,621 (due to overlap in international classification of diseases [ICD]-9 and [ICD]-10 E codes in these categories). We defined related visits as health care encounters (e.g., office visit, emergency room visit, urgent care visit) with a primary diagnosis code in the same CCS category as the initial, or triggering, visit. For each episode, we identified whether the triggering visit was conducted via telemedicine or in-person, as well as the number of related visits. Related visits include both telemedicine visits and in-person visits.
Identifying an Intervention Group and Control Group
Our intervention group included all episodes of care initiated via a telemedicine visit. To identify our control group, we used the propensity score theorem to control for the covariates affecting the likelihood of a telemedicine visit within each CCS category. 14 Namely, we focused on age, sex, and number of comorbidities. We first estimated the propensity scores based on the covariates—age, sex, and number of comorbidities—and used a logit model for telemedicine and in-office claims. We then matched the two groups (telemedicine and in-person) based on the propensity scores for our analysis.
Primary Outcome and Statistical Analysis
Our primary outcome was the “related visit rate,” which is defined as the percentage of 30-day episodes with a related visit for each CCS category (and ML-CCS category). We compared this primary outcome for 30-day episodes of care initiated via telemedicine visit (intervention group) with the 30-day episodes of care initiated through in-person visits (control group). We also calculated the mean number of related visits for each category. For this mean related visit rate, we excluded observations with no related visits.
Institutional Review Board Statement
This study was deemed not-regulated by our university's institutional review board.
Results
The final data set included 4,982,456 patients (52.7% male and 47.3% female) and 68,148,070 observations (i.e., claims). Of these claims, 53,853 were telemedicine claims, which is <1% of total claims. Telemedicine was used most for mental health illnesses (e.g., mood disorder, anxiety disorder, attention-deficit disorder), upper respiratory tract infections, urinary tract infections, and diabetes (Table 1). When grouping conditions via ML-CCS categories, as demonstrated in Table 2, mental illnesses account for the highest number of telemedicine visits, followed by endocrine, nutritional, and metabolic diseases, immunity disorders, and diseases of the respiratory system.
Top Clinical Classification Software Categories with Telemedicine Visits
CCS, clinical classifications software.
Multilevel Clinical Classifications Software Categories and Associated Telemedicine Visits
ML-CCS, multilevel clinical classifications software.
It was common for episodes to not follow with related visits within 30 days. For all CCS categories, we found that the mean related visit rate was 16% (median 12%, range 2–71%), and the mean number of related visits was 0.25 (median 0, range 0–10). Figure 1 shows the percentage of episodes within a CCS category (and an ML-CCS category) with at least one related visit. We observed that the mental illness ML-CCS category had the highest frequency of claims with related visit(s), whereas infectious and parasitic diseases account for the lowest.

Percentage of episodes in each CCS that has at least one related visit within 30 days: bars show the percentage by CCS categories and lines show the percentage by ML-CCS categories. CCS, clinical classification software; ML-CCS, multilevel clinical classifications software.
We observed that telemedicine visits (intervention group) correspond to a higher frequency of related visits compared with in-office visits (control group) (Fig. 2). This effect seemed to exist across all the CCS categories.
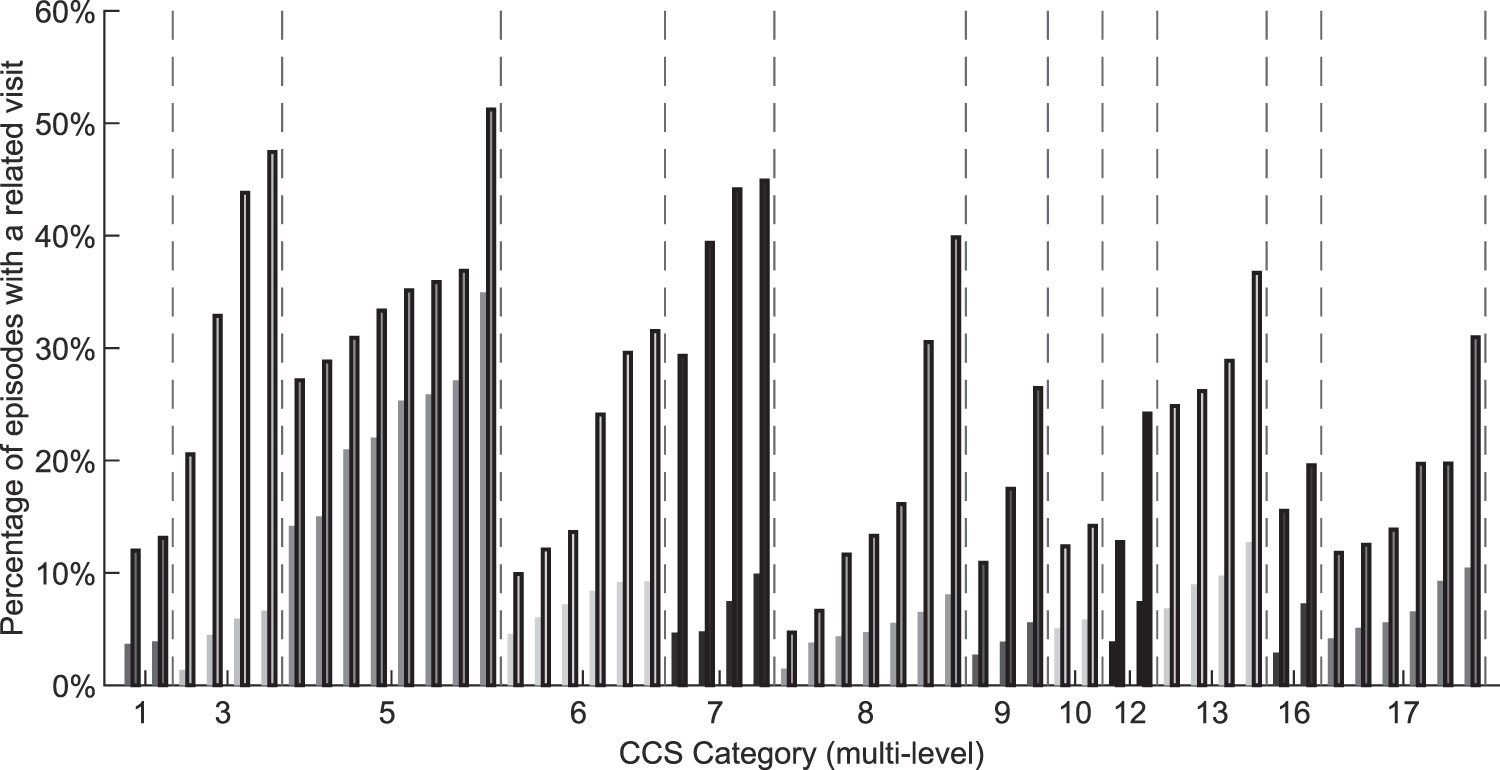
Percentage of episodes that have at least one related visit: comparing telemedicine episodes and propensity score matched in-office episodes (categories with <100 telemedicine episodes are omitted). Bars with outline represent telemedicine visits, bars without outline represent non-telemedicine visits.
For further analysis, we looked at the mean number of related visits and compared episodes initiated via telemedicine versus in-person visits. For this analysis, we considered the mean difference of related visits for telemedicine- and in-office-initiated episodes (excluding episodes with no related visits). Figure 3 illustrates our results. We focused only on the ML-CCS categories with significant treatment effects (i.e., the mean difference for the number of related visits between telemedicine- and in-office-initiated visits was statistically significant). We observed that the mean number of related visits was higher for telemedicine-initiated visits across all CCS categories except for mental illnesses CCS categories, for which telemedicine-initiated visits corresponded to a lower mean number of visits.

Difference in the mean number of related visits (telemedicine–nontelemedicine): comparing telemedicine episodes and propensity score matched nontelemedicine episodes (t-test p-value ≥0.05 omitted, null hypothesis: indifferent in mean).
Discussion
In our study, we found that it was more common for patients to schedule related visits within 30 days if their episode of care was initiated via a telemedicine visit rather than an in-person visit. We also found that in episodes where patients had a related visit, the mean number of visits was higher in most CCS categories for episodes of care initiated via a telemedicine visit. Together, these findings suggest that telemedicine may not be a direct substitute for in-person care and may actually trigger additional related care.
Our finding that telemedicine visits may lead to increased downstream visits is consistent with prior studies, which found that e-visits (secure messaging between providers and patients through a portal) prompted an additional ∼6% of office visits. 8 e-Visits also led to increased use of prescription antibiotics for certain conditions, although with decreased use of related tests and imaging. 9
Our study has several limitations. First and foremost, we cannot conclude whether the additional visits observed for our telemedicine cohort represent excessive care or expanded access to care. Second, many CCS categories contained few telemedicine visits in total, and therefore, more years of data are necessary to observe significant effects within CCS categories. Third, our analysis was conducted using a single payer in a single state, which may impact the generalizability of our results. However, BCBSM is a large commercial payer in the state, and the state of Michigan is diverse, so we would expect these results to be fairly generalizable.
Our limitations notwithstanding, our findings have significant implications for policymakers. Our finding that telemedicine visits may lead to additional downstream visits may impact cost savings calculations. We recommend tracking this unintended consequence, as these indirect costs can influence decision-making around parity laws for telemedicine reimbursement. For patients, however, telemedicine may seem like a convenient option to meet their health care needs, but it may ultimately be more burdensome if these types of visits lead to additional, and potentially avoidable, encounters. For providers, increased downstream visits within an episode of care may reduce their ability to see new patients, as prior studies have shown.
Our findings suggest that, while telemedicine has the potential to improve health care delivery by substituting in-person care, its use may lead to unintended consequences such as increased health care utilization. Moving forward, research in this area should determine whether additional telemedicine health care encounters initiated via telemedicine visits reflect inadequate care or improved access to care. It would also be worthwhile to conduct a more granular assessment of the mental illness CCS category to better understand why telemedicine-triggered episodes of care had fewer mean-related visits. In the end, the successful expansion and widespread adoption of telemedicine may transform health care delivery, but unintended consequences should be closely monitored.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Ellimoottil is supported by K08 HS027632-01 from the Agency for Healthcare Research and Quality.