
Abstract
Background:
Huntington's disease (HD) is a complex neurodegenerative disorder that causes impairment in cognitive, motor, and psychological function and requires subspecialty neurological and interdisciplinary care. Access to subspecialty care for HD is restricted by disability from the disease, lack of trained providers, and barriers to care for disadvantaged and rural populations.
Program Description:
Since 1999, the University of Virginia HD clinic has used telemedicine to provide clinical services, consultation, and staff training. Initially, encounters were scheduled with the neurologist on a case-by-case basis at outlying rural clinics and community hospitals. Since 2015, telemedicine visits have been conducted by the entire interdisciplinary HD team and access has been extended to homes and long-term care facilities. This infrastructure was used to conduct a virtual clinic 2 days after initiation of coronavirus disease (COVID) mitigation. The clinic has continued to provide subspecialty and interdisciplinary care through telemedicine while clinic access has been restricted. A total of 69 individuals have been seen in 127 telemedicine visits, 56 of which were conducted by the interdisciplinary team.
Conclusions:
Telemedicine can provide high-quality subspecialty neurological and interdisciplinary care for HD that offers continuity across a wide range of care settings, and can overcome both anticipated and unanticipated barriers to access.
Introduction
Huntington's disease (HD) is a complex neurodegenerative disorder that causes progressive impairment in cognitive, motor, and psychological function over an average disease course of 20 years. Optimal management requires subspecialty neurological and interdisciplinary care. Subspecialty neurological and interdisciplinary care can improve outcomes, maintain function, and reduce morbidity and caregiver burden in HD and related disorders, but is generally available only at major medical centers and specialty clinics. 1 –5 Travel to a distant facility presents logistical and financial challenges, particularly as HD symptoms progress.
Telemedicine can increase access to specialized neurological care and is well established for management of acute stroke, but experience in other neurological disorders is limited. 6 Interest in telemedicine for HD and other movement disorders has grown. 1 –3,7–10 Of HD clinics responding to an international survey, 23.6% reported using telemedicine, and remote motor assessments in HD have been shown to be reliable when compared with office assessments. 1,9 In general, telemedicine has not been widely used for interdisciplinary care in movement disorders, although a Canadian program includes social work services. 2,10
The University of Virginia (UVA) HD program has provided interdisciplinary care for patients with HD since 1996, with neurological follow-up offered through telemedicine since 1999. In 2015, telemedicine services were expanded to include interdisciplinary care. In this report, we describe >20 years of experience providing subspecialty neurological and interdisciplinary care for HD through telemedicine.
Program Description
Initially, telemedicine services for HD were provided on a case-by-case basis for neurological follow-up, using synchronous video and audio connections over a broadband network connecting remote sites to the UVA Office of Telemedicine, now the Karen S. Rheuban Center for Telehealth. Patients were seen at a network of partner sites, primarily in rural areas. For the past 5 years, telemedicine visits have been scheduled in monthly interdisciplinary clinics and as stand-alone visits. Patients are seen simultaneously by a medical provider (physician or nurse practitioner) and rehabilitation specialists from physical therapy, occupational therapy, and speech language pathology with additional providers available, including a psychiatrist, genetic counselor, social worker, and chaplain. Telemedicine encounters originate from the neurology clinic or telemedicine office. Tablets are loaned to patients if needed, and use of secure Health Insurance Portability and Accountability Act compliant on-line portals has extended access to homes and long-term care facilities. Additional locations around the state include county or health department clinics, community hospitals, correctional facilities, and psychiatric hospitals (Fig. 1 and Table 1). The information technology staff members from the UVA Karen S. Rheuban Center for Telehealth provide technical support.
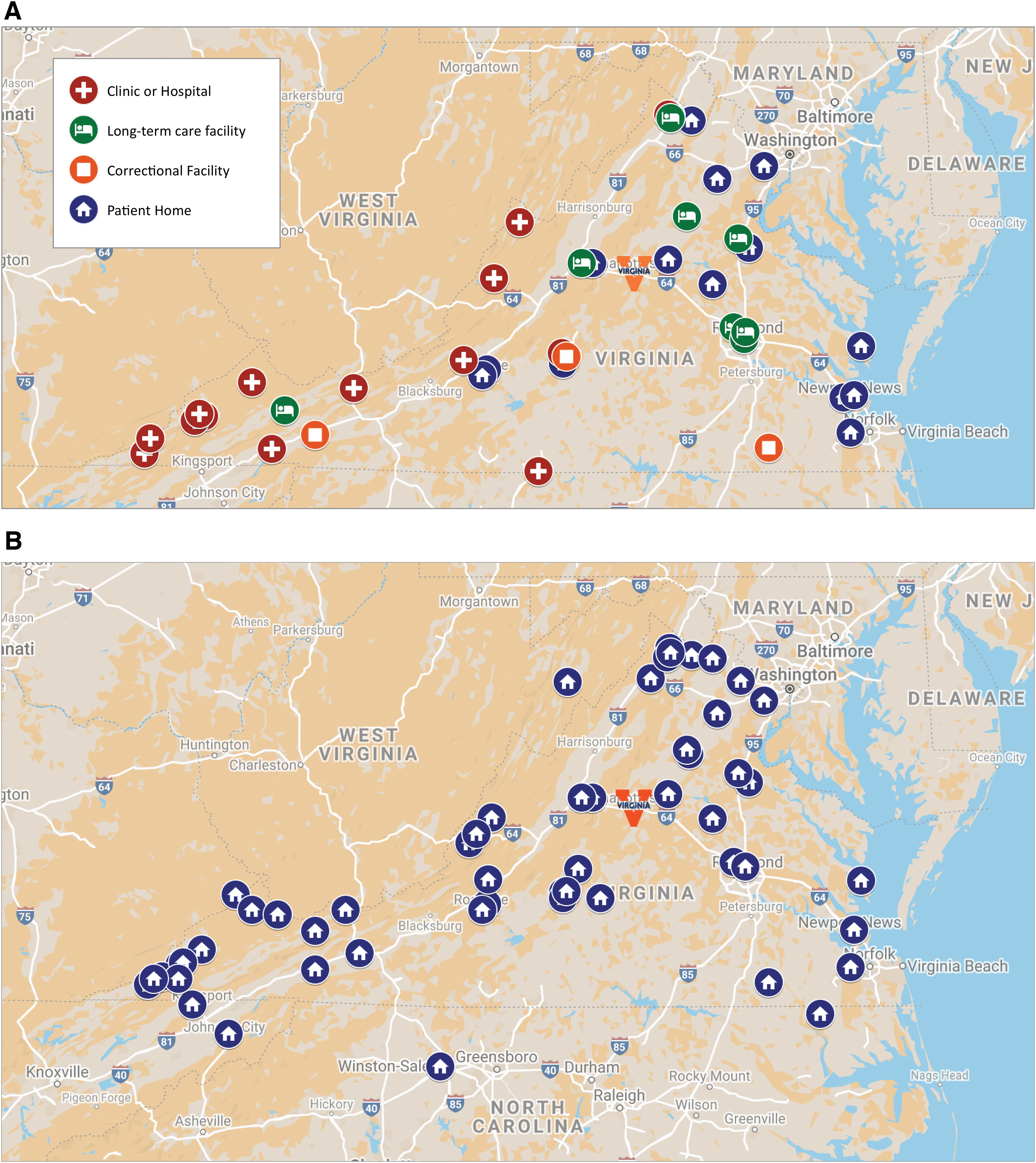
Geographic distribution of telemedicine sites and patient locations 1999–2020
Telemedicine Encounters 1999–2020
This table displays the number of individual patients seen and number of telemedicine encounters conducted through videoconferencing since 1999. These are further broken down by sites, participating providers, and services provided.
Eleven additional telemedicine visits were conducted as structured telephone encounters for patients without videoconferencing access.
HD, Huntington's disease; LTC, long-term care facilities.
To date, 69 patients have participated in 127 visits, 41 for 1 visit and 28 for 2–7 visits. Of these, 51% were seen at home or in a long-term care facility with the remainder seen at 19 separate community settings (Table 1). Most patient visits have been for continuity of care, with a few seen for diagnostic evaluation or initial management. In addition to direct patient care, additional services offered through telemedicine have included interprofessional case consultation with local providers, on-site consultation with in-home providers, in-service training sessions for facility staff, and family and genetic counseling. Recommendations from our telemedicine encounters are similar to those resulting from on-site encounters, including medication management, home health referrals, equipment prescriptions, and referrals for genetic testing, imaging, cognitive testing, counseling, driving evaluations, and research studies.
The use of telemedicine has saved 39,470 miles and 654 h of travel time for patients and families with an average per visit of 310 miles and 5.15 h. Availability of telemedicine services prevented 32 patients from being lost to follow-up, 6 of whom were followed across multiple sites. As already noted, telemedicine has also allowed us to offer first-time HD subspecialty care to patients without other access.
Discussion
In this report, we describe delivery of interdisciplinary care for HD through telemedicine. Over 20 years, our telemedicine services have evolved from episodic subspecialty neurological care at remote institutional sites to a routinely available service providing integrated interdisciplinary care, often at home or in long-term care facilities. Our experience adds to the growing literature on provision of subspecialty neurological care to patients with movement disorders by telemedicine and demonstrates that telemedicine can provide access to specialized interdisciplinary care in multiple settings. 2,3,7 –10
Advantages of telemedicine include improved access to interdisciplinary and subspecialty care and reduced economic and logistical burdens for patients and families. There are additional qualitative benefits to care provided by telemedicine. The stress of travel to a distant clinic can affect patient function and alter performance during the evaluation. In HD, this can result in behavioral issues that affect the assessment and also limit access. Assessment in home or long-term care settings offers direct observation of the patient's environment and enhances communication and coordination with patients, families, and other providers. However, as for many areas in teleneurology, formal assessment of outcomes is needed. 2,6,10
There are some limitations to care through telemedicine. Lack of access to telecommunication technology may limit availability. Poor audio or video quality can impair communication and observation. Parts of the neurological examination cannot be conducted remotely, such as strength, sensation, and reflexes. Development of telemedicine services has also been limited by reimbursement and infrastructure issues, although the rapid expansion of telehealth capacity in response to coronavirus disease (COVID) has reduced these administrative barriers, at least temporarily.
Our experience indicates that telemedicine can effectively provide subspecialty neurological and interdisciplinary care for complex neurodegenerative diseases such as HD, offering continuity across care settings in the face of both anticipated and unanticipated barriers to access.
Footnotes
Acknowledgments
The authors acknowledge the invaluable contributions of the University of Virginia Huntington's Disease Program team to the interdisciplinary telemedicine services and thank the University of Virginia Karen S. Rheuban Center for Telehealth for logistical and technical support.
Disclosure Statement
No competing financial interests exist.
Funding Information
The University of Virginia Huntington's Disease Program receives grant support from the Huntington's Disease Society of America. Financial disclosures for the previous 12 months: M.B.H. and MD receive clinical research support from the CDHI Foundation and Neurocrine, and support for clinical programs from the Huntington's Disease Society of America and the American Parkinson Disease Association.