
Abstract
Background:
Telepsychiatry is a well-studied modality that has been shown to perform as well as, if not better than, in-person mental health services. However, acceptability of this modality to practitioners, especially as it relates to the type of consult, has not been well studied. To address barriers to implementing a new telepsychiatry consultation–liaison (CL) service at a rural campus of a large tertiary care health network, authors designed a survey to assess consultee attitudes before and after the service launch. A secondary objective was to examine the consult data.
Materials and Methods:
The new telepsychiatry CL service at the rural hospital was delivered by providers at the main campus of the health network. Authors surveyed all consultees before the launch and every 3 months for 12 months thereafter. Consult data was also tracked in that same period.
Results:
Over a 12-month period, 442 initial and follow-up consults were completed. Consultees were most concerned with assessing delirium, agitation, and neurocognitive disorder over live video. Consultees generally held their belief that telepsychiatry consults are not as enjoyable as in-person consults, but they recognized its value, specifically regarding improved access for patients.
Discussion:
The service was successfully launched and was well received as evidenced by the continued use of the service.
Conclusions:
The project revealed valuable insight which has been used to improve the service and to replicate it at another campus within the health network.
Introduction
Telepsychiatry is a well-studied modality that has been shown to perform as well as, if not better than, in-person mental health services. 1,2 Studies have demonstrated feasibility of a telepsychiatry consultation–liaison (CL) service from urban academic medical centers to remote hospitals. 3 –6 However, concerns over impaired therapeutic rapport and acceptability of this modality to practitioners have been raised. 7 –9
In a 2017 survey at Lehigh Valley Health Network (LVHN) in Eastern Pennsylvania, physicians expressed concerns about telemedicine, specifically regarding the loss of personal contact. 10 In that survey, 68% of physicians across specialties believed that patients prefer to see their doctors in person, and 85% of psychiatrists thought that patients receive better quality of care in person. Interestingly, there is a growing body of evidence that supports telepsychiatry's ability to deliver both high quality of care and high patient satisfaction. 1 As LVHN prepared to launch a new telepsychiatry CL service at one of its rural campuses, the survey findings highlighted the need for a quality improvement process to measure and optimize provider satisfaction.
The flagship hospital of LVHN is the Cedar Crest campus, which is a 1,167-bed, tertiary care facility in an urban setting with a robust, full-time CL service. In 2016, LVHN acquired the Schuylkill campus, which is a 320-bed hospital located in Pottsville, Pennsylvania, a city with a population of ∼15,000 and 45 miles away from the Cedar Crest campus. Historically, the Schuylkill campus only had a part-time CL service due to limited availability of local psychiatrists. To improve access to CL psychiatrists for patients at the Schuylkill campus, LVHN launched a new telepsychiatry CL service at the rural hospital to be delivered by providers at the Cedar Crest campus.
To address barriers to implementing the new telepsychiatry CL service, the authors assessed consulting psychiatric providers' attitudes shortly before the service launch and for 12 months thereafter. Consult data from the same period was also examined.
Materials and Methods
This was a single-center quality improvement project conducted through provider surveys and administrative record review. The goal of this project was to evaluate telepsychiatry as an acceptable modality to psychiatric consultants. With that goal in mind, the inclusion criteria for provider surveys were physicians, physician assistants (PAs), and certified registered nurse practitioners (NPs) who perform either in-person or video psychiatric consultations within LVHN. Excluded from the surveys were resident physicians, fellows, medical students, and telemedicine nurses and technicians. For the consult data presented in this project, we included every initial and follow-up consultation involving a video encounter between a provider and a patient. If a consultation was requested but the patient declined to see a psychiatric provider or was discharged from the hospital before an encounter could occur, it was excluded from analysis.
LVHN is made up of seven hospital campuses, all within Eastern Pennsylvania. The inpatient psychiatric CL service at the Cedar Crest campus was staffed by seven psychiatrists, two PAs, and two NPs at the beginning of this project. The service provides full-time, in-person CL coverage at three hospitals: the Cedar Crest campus and the 17th Street campus both in Allentown, Pennsylvania, and the Muhlenberg campus in Bethlehem, Pennsylvania. In-person coverage is 8:00 a.m. to 5:00 p.m., 7 days/week, and phone coverage is 24/7. With the ultimate goal of providing the same coverage schedule at every campus of LVHN in a cost-effective manner, a new telepsychiatry CL service was launched at the Schuylkill campus in January of 2019.
Consultation requests from the Schuylkill campus were sent to the CL administrative staff at the Cedar Crest campus, who would then schedule patient encounters within 24 h of the request, Monday through Friday. For the encounter, a telemedicine nurse at the Schuylkill campus would bring a computer-on-wheels with televideo capability through hospital Wi-Fi into the patient room. The CL psychiatrist would begin the encounter in a private, designated workspace at the Cedar Crest or the Muhlenberg campus using a Logitech C920 webcam, a headset with microphone, and Cisco WebEx videoconference software. The electronic health record (EHR) system at the Schuylkill campus was a software developed by Computer Programs and Systems, Inc. until it was switched to Epic in October of 2019.
Before service launch, the authors developed an anonymous survey with 17 Likert-scale questions and 2 free response questions (Appendix A1). Questions 1 through 6 were taken from a previously validated survey, which was used in 2017 to assess LVHN physicians' attitude toward the use of telepsychiatry. 10 Questions 7 through 19 were new and piloted to the department chair of psychiatry. To anonymously identify the provider completing the survey, every survey asked for mother's first initial, middle initial, and two-digit birth month (e.g., Joan Mary Smith born on 08/01/1933 would be: JM08).
The surveys were completed on paper by the providers at the weekly CL team meeting. The preimplementation survey was completed one week before the service launch in January 2019. After the launch, postimplementation surveys were completed every 3 months for 12 months. The postimplementation survey was identical to the preimplementation survey, except for questions 1, 2, 18, and 19, which were appropriately modified to the present tense.
Before the service launch, it was unclear if PAs and NPs would be completing telepsychiatry consults alongside physicians. Therefore, all providers in the CL team, including the PAs and NPs, completed the preimplementation survey. Although it was later decided by the department that telepsychiatry consults would only be completed by physicians during the first year of the service, the authors surveyed all eleven providers throughout the 12 months to find out how the perspective of the entire CL team on telepsychiatry would change based on both first-hand experience and conversations between colleagues.
Survey responses were analyzed by calculating the Likert mean, which is a weighted average of all providers' responses by assigning a numerical value to each answer choice. For questions 1 through 8, the Likert mean was calculated by assigning 1 to strongly disagree, 2 to disagree, 3 to do not know, 4 to agree, and 5 to strongly agree. For questions 9 through 17, the Likert mean was calculated by assigning 1 to very concerned, 2 to concerned, 3 to do not know, and 4 to not concerned.
The CL administrative staff routinely tracks every consult request with the reason for consultation cited by the requesting physician at the Schuylkill campus on a daily basis. The authors reviewed this information and populated a spreadsheet. Chart review and analysis of patient demographics were intentionally omitted, because the authors' aim was to complete a quality improvement project with an investigative focus on provider satisfaction. This project was approved by LVHN's Institutional Reviewed Board and was not deemed human research.
Results
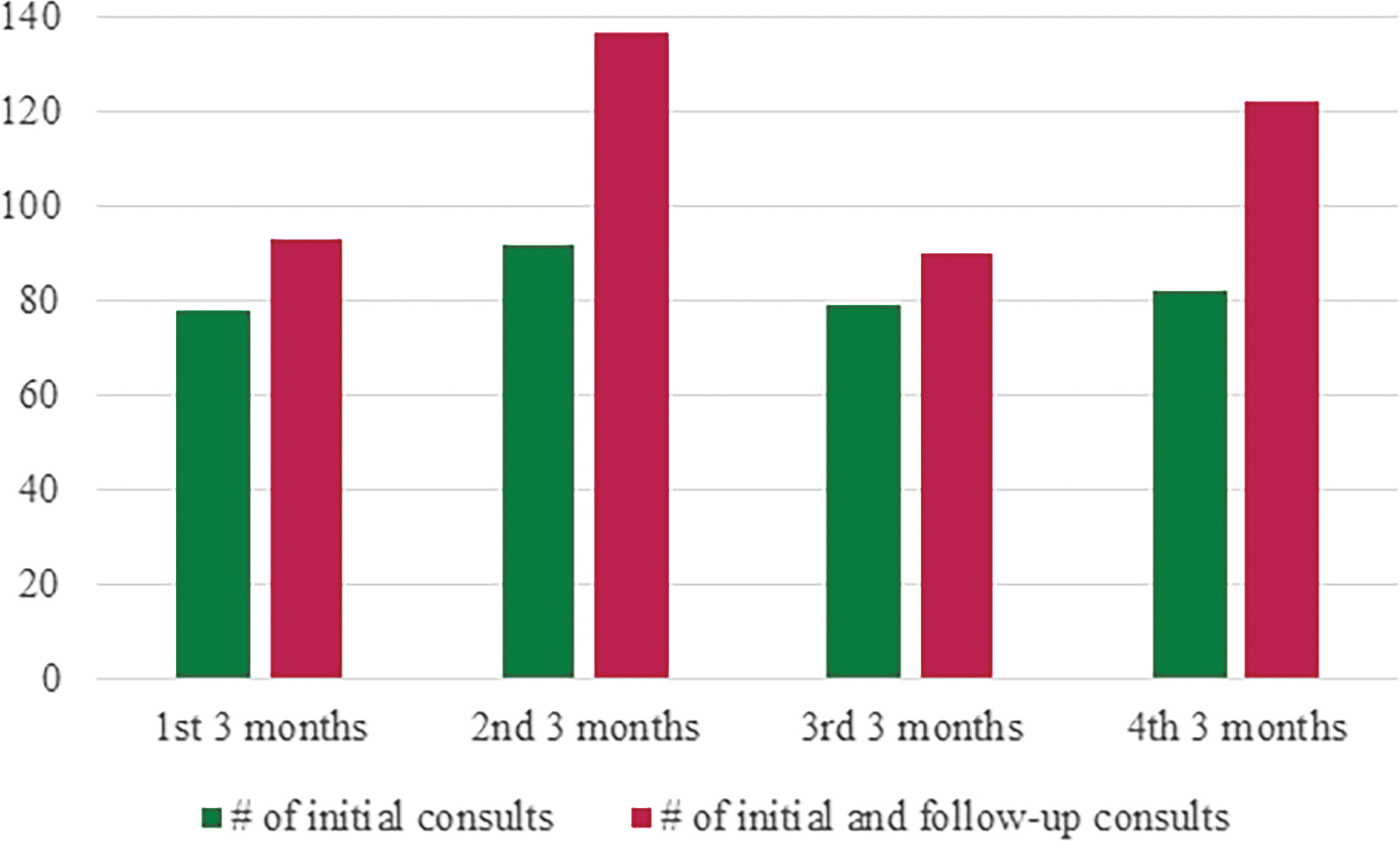
Over the first 12 months of the service, five physicians completed 331 initial and 111 follow-up consults over live video (Table 1). The average number of follow-up consults performed after an initial consultation was 0.34, with a range from 0 to 5. Figure 1 displays the number of consults for each 3-month quarter of the study period. Table 2 summarizes the reason for consult as cited by the requesting physician at the Schuylkill campus. Of the 331 initial consult requests, 17 had undocumented or unclear reason for consult, and 34 had multiple reasons cited for consult.
Number of initial and follow-up telepsychiatry consults seen during 3-month periods at Lehigh Valley Hospital—Schuylkill.
Number of Consults at Lehigh Valley Hospital—Schuylkill
Reason for Consult As Cited by the Requesting Physician at Lehigh Valley Hospital—Schuylkill
Likert mean of survey results reflecting the consultees' general attitude toward the telepsychiatry service is shown in Figure 2. Consultees' level of concern for managing a specific diagnosis through telepsychiatry are summarized in Figure 3. Survey response rates were 100% at preimplementation and 6 months and 82% at 3, 9, and 12 months.

Likert mean reflecting change in attitude toward the telepsychiatry consultation service. The figure reflects responses to survey questions 1–8 from Appendix A1. Likert mean was calculated by assigning strongly disagree = 1, disagree = 2, do not know = 3, agree = 4, and strongly agree = 5.
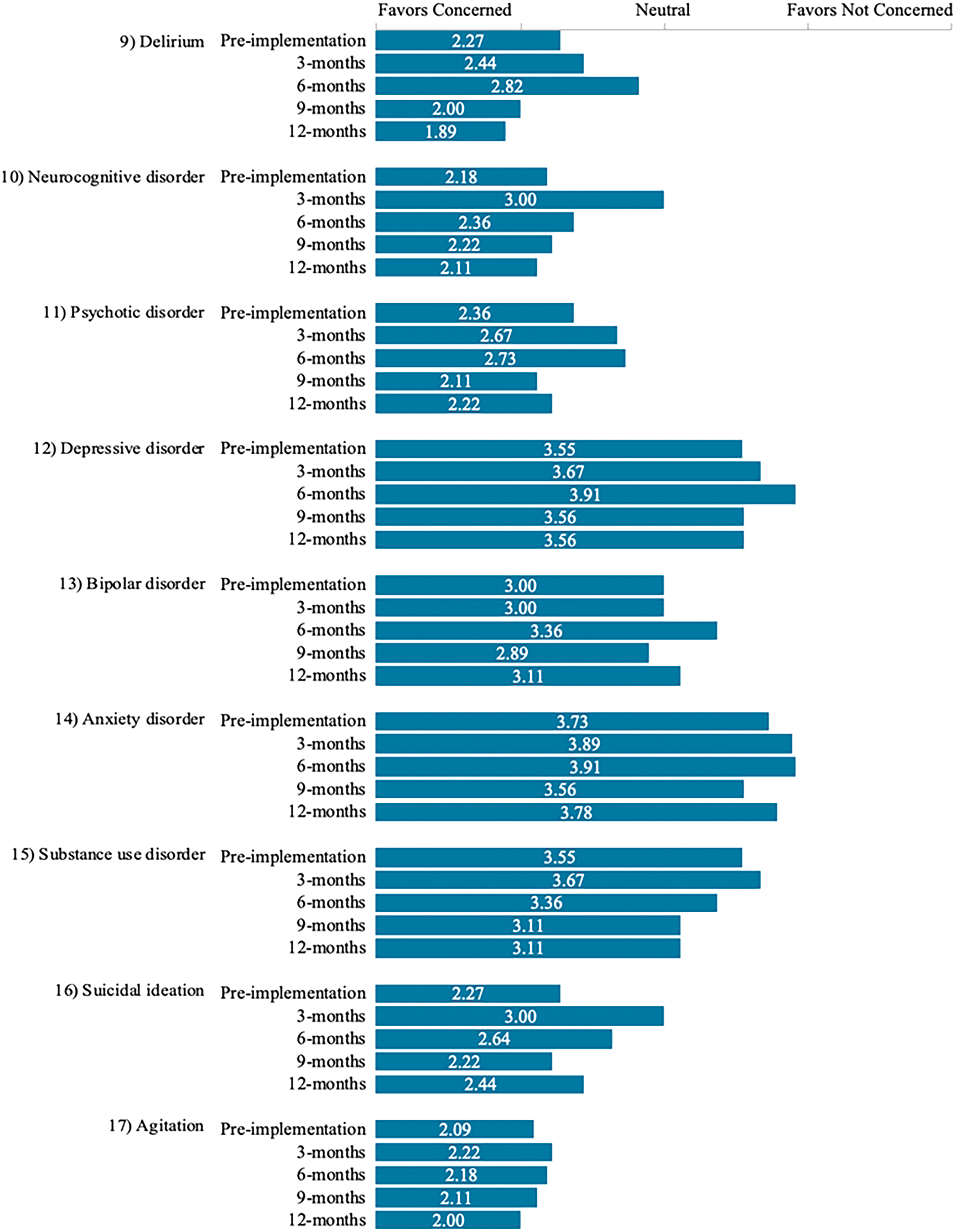
Likert mean reflecting change in consultees' level of concern for performing telepsychiatry consult for a specific diagnosis. The figure reflects responses to survey questions 9–17 from Appendix A1. Likert mean was calculated by assigning very concerned = 1, concerned = 2, do not know = 3, and not concerned = 4.
In response to question 18, the CL providers raised concerns about establishing patient rapport; establishing an efficient daily workflow; forming reliable, high-quality video connection over the hospital Wi-Fi network; establishing a culture of acceptance of telepsychiatry consults by the consulting primary teams at the Schuylkill campus; and being able to observe subtle physical exam signs over video.
In response to question 19, the CL providers suggested to adjust consult coverage schedule at the Cedar Crest and Muhlenberg campuses to account for time demands of completing telepsychiatry consults; start follow-up interview sessions at the same time each day; allow PAs and NPs to join the telepsychiatry service; unify the EHR systems across campuses; offer prompt, in-session technical support; improve the quality and reliability of video connection; and train the Schuylkill campus nursing staff to detect important, specific physical signs, such as extrapyramidal symptoms and signs of substance withdrawal.
Discussion
Survey responses to questions 1 and 8 demonstrate that the CL providers recognize the value of telepsychiatry, specifically regarding improved access for patients, but they enjoy completing in-person consultations more than teleconsults. Other studies have published similar findings of psychiatrists reporting less satisfaction with telepsychiatry than seeing patients face-to-face in outpatient and school settings. 11,12 It is worth noting that these responses were from before COVID-19, and it would be interesting to see how the pandemic may have shifted these attitudes given that a large percentage of the work across the department has also become virtual.
Responses to question 7 show that providers initially believed technical support for telepsychiatry to be inadequate, but that attitude noticeably improved between the 9- and 12-month survey periods. Anecdotal interviews at around this time revealed that providers noticed a significant improvement in video quality after some telemedicine nurses began using an Ethernet cable, rather than Wi-Fi, to connect the telemedicine computer-on-wheels to the internet. This period was also when the Schuylkill campus migrated its EHR system to Epic, which was the EHR in use at the Cedar Crest and Muhlenberg campuses and was therefore the system that CL providers were familiar with.
A frequently raised suggestion for improvement by CL psychiatrists was to allow PAs and NPs to perform telepsychiatry consults to increase the workforce and flexibility of schedule. They remarked that for various reasons, telepsychiatry consults took longer to complete than in-person consults, so allowing them to join the work would add more flexibility to physicians' daily workflow. As of 2020, this change has been implemented with the PAs and NPs now performing more telepsychiatry consults at the Schuylkill campus than physicians.
By the end of the year, consultees were most concerned with managing delirium, agitation, and neurocognitive disorder. A common theme among these disorders is that they could often result in behavioral disturbances on the unit. On the other hand, consultees were least concerned with managing anxiety disorder, depressive disorder, and substance use disorder over video. Specifically for mood disorders, many previous studies have demonstrated noninferiority in treatment outcome when comparing telepsychiatry to in-person treatments. 2,13 This might explain why the management of anxiety and depression were least concerning to telepsychiatry consultants at LVHN.
The limitation of the study was the small number of providers who were generating survey results. Furthermore, some surveys were being completed by providers who did not have first-hand experience in the telepsychiatry CL service but were instead engaged in frequent conversations with providers who were performing them.
Lessons learned from this project have been used to prepare for the launch of another telepsychiatry CL service, this time at the Hazelton campus, to continue addressing the geographic inequities in access to CL psychiatry. This project has opened the door for future studies utilizing the vast amount of data that will come out of the rapid change to virtual delivery of psychiatric care during the COVID-19 pandemic.
Conclusions
The new telepsychiatry CL service at LVHN was successfully launched and was well received as evidenced by the continued use of the service. The main goal of this quality improvement project was to identify and address the barriers to high consultee satisfaction. Frequently cited barriers were inadequate video quality, disjointed EHR systems across campuses, and inability for physicians to share the workload with their PA or NP colleagues. In light of these findings, the EHR system has been unified across campuses, and the department has allowed PAs and NPs to join the telepsychiatry CL workforce. The department has used these strategies to replicate the service at other campuses within the Network.
Footnotes
Acknowledgments
The authors wish to thank the clinicians, staff, and administrators at Lehigh Valley Health Network.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.