
Abstract
Background:
Access to patients' medical histories can be of vital importance to ensure proper treatment in an emergency. Germany is planning to introduce a medical emergency dataset (MED), accessible through an electronic health card, and comprising important patient information, such as diagnoses, medications, and allergies.
Introduction:
This article evaluates the effect of MEDs on the comprehensiveness of a physician's documentation and handover process to the emergency department of a hospital.
Materials and Methods:
In 2 randomized, crossover simulation studies, 72 emergency physicians participated in 2 emergency scenarios, either with or without access to an MED. Subsequently, they had to document the key information (pre-existing conditions, medications, and allergies) and hand it over to a fictional hospital. The influence of the MED on the documentation of key information was analyzed using the two-sided Prescott's exact test. Sensitivity analyses adjusting for scenario were conducted.
Results:
The results show that in scenarios with an MED, documentation of key information in the handover process was more complete. In the first trial, 2 of 3 key items (pre-existing conditions/information and allergies) presented a statistically noticeable difference in scenarios with the MED. The second trial confirmed these results for all key items.
Discussion:
The findings indicate that the use of MEDs in emergency care could be beneficial since documentation and handover in scenarios with an MED were superior to current real-world practices.
Conclusions:
Access to more complete patient information through an MED could help to improve the patient's treatment.
Introduction
Access to patients' medical histories can be vital in case of a medical emergency. 1 Furthermore, the exchange of health information between health care professionals is important to ensure quality of care in the ongoing treatment process. 2,3 Over the past decades, several initiatives to promote a digital dataset with emergency-relevant patient information have been launched. 4 –8 Often referred to as a “Patient Summary,” “Emergency (Care) Summary,” or “Summary Care Record,” these datasets are primarily used in hospitals and doctor's offices as patient information is mostly shared between health care providers in clinical settings. Unlike the aforementioned initiatives, the plan in Germany is to store a medical emergency dataset (MED) in a decentralized manner on patients' electronic health cards (EHCs). One of the main focuses of MEDs is in the field of preclinical emergency care.
In the German Preclinical Emergency Medicine Model, emergency medical services (EMSs) are physician staffed. Response teams (at the highest activation level) are led by emergency physicians who are certified in emergency medicine and manage emergencies on-site before handing over the care to doctors of the emergency department (ED) upon arrival at the hospital. In the near future, emergency physicians will be able to get access to the MED on patients' EHCs through an electronic card reader in combination with their Health Professional Card.
9
The text-based dataset can be created by the patient's treating physician and consists of the following components
10
: Diagnoses Medications Allergies Medical implants Special needs/information (e.g., pregnancy and communication barrier) Contact information (e.g., family and physician).
It is worth noting that the MED comprises summarized medical information and does not contain any recommendations or instructions for treatment in case of an emergency.
Thus far, neither the effect of the MED on treatment decisions in an emergency situation outside a hospital nor its influence on the subsequent documentation and handover to the ED has been evaluated. One goal of the research project, Timely Information in Medical Emergencies, was to assess the anticipated impact that the MED will have on emergency care. Funding for the project was provided by the European Union and the Federal Ministry of Health, Equalities, Care and Ageing of North Rhine-Westphalia, Germany.
Within the framework of the project, two simulation studies evaluated the performance of emergency physicians presented with different emergency scenarios. The scenarios were performed in a setting where either (1) the MED was not available or (2) the MED was available on the scene. The focus of the current article lies on the effect of MEDs on the comprehensiveness of emergency physicians' documentation and handover processes in simulated emergency scenarios.
Materials and Methods
Trial Design
Two randomized, crossover simulation studies (AB/BA crossover), each lasting 2 consecutive days, were conducted in September 2016 and October 2017. Both trials were performed at the training center of the University Hospital Muenster, Germany. Approval from the ethics committee of the local medical council and the University of Muenster was obtained before conducting the studies (ethics vote 2016-369-f-S). All participants (hereinafter also referred to as emergency physicians) signed an informed consent form for data gathering and analysis.
An expert committee comprising two medical directors of the German Rescue Service and two emergency physicians created three scenarios with a focus on internal medicine. The scenarios were common situations that emergency physicians might be confronted with while on duty. The emergency situations had built-in pitfalls (unwanted preclinical actions), so additional health information was useful to find the optimal treatment. Table 1 gives an overview of the scenarios, obtainable information, and unwanted medical procedures. For the two trials, the general approach differed:
Scenarios in the Two Trials Displayed with Obtainable Medical Information and Unwanted Preclinical Actions
AV, atrioventricular; BG, blood glucose; BP, blood pressure; Ca, carcinoma; CPR, cardiopulmonary resuscitation; ECG, electrocardiogram; HCT, hydrochlorothiazide; HR, heart rate; INR, international normalized ratio; PCI, percutaneous coronary intervention; SpO2, pulsoximetric oxygen saturation; SR, sinus rhythm.
a. The first trial compared matching scenarios of either (1) a setting in which the participants could only use information provided by the environment or (2) a setting in which participants additionally received the MED on the scene. Participants were not informed about the MED before the trial.
b. The second trial compared matching scenarios of (1) a setting where no additional information was available to participants in the environment against (2) a setting in which participants received the MED on the scene. Participants were informed about the concept of the MED before the study.
In the first trial, potentially useful information was planted in the environment for participants to find because it seemed highly likely that the information available to the participants in scenarios with an MED would be superior to scenarios without any additional information. In the second trial, a priori MED information was provided and we chose control scenarios without any additional patient health information in the environment. This was another important and realistic situation to account for, as was the setting with information provided by the environment in the first study.
In accordance with the crossover design, all emergency physicians would perform one simulation run (hereinafter also referred to as a run) with MED and one without MED. The order in which each of the scenarios occurred (with MED/without MED or without MED/with MED) was randomly selected. To avoid a possible learning effect among the emergency physicians, each was randomly assigned to only two of the three created scenarios. The randomization procedure is described in more detail in the Supplementary Data.
Simulation Settings
In each scenario, simulated patients (SPs) and the roles of family members or acquaintances were performed by professional actors. The supporting team in a scenario consisted of two real paramedics to assist the emergency physician with standard patient care (e.g., blood pressure monitoring) and one person giving stage instructions (e.g., when the patients' condition progressed). The scenarios were scripted so that the actors as well as the supporting team would only give standardized answers and could not help with the decision-making of the participants. At predefined times, the actors would perform specific actions or the vital parameters of the SP would change regardless of the emergency physicians' prior actions, so immediate action was required.
For subsequent data analysis, the simulation runs were recorded on video. After each run, the emergency physician would hand over the gathered information about the patient to a fictitious hospital in a secluded video booth where they would also complete a handover protocol. 11 In this scenario, it was essential that any key pre-existing conditions and information such as the patient's allergies and medications were documented. After completion of the simulation runs, the emergency physicians were asked to complete a pseudonymized questionnaire concerning their profession and demographics, scenarios, and specific questions about the MED. A more detailed description of the general procedures and documentation process during the trials is given in the Supplementary Data.
Because electronic MEDs on the EHC and reading devices had not yet been implemented, a DIN A4-sized paper MED was created for each SP in the scenarios. Figure 1 shows an example of an MED that was provided. In settings with an MED, the accompanying actor would mention that the patient has an MED and hand it to the emergency physician after a certain amount of time had elapsed and none was requested. As stated above, some of the patient's medical history could be obtained from the environment in the first trial. Stacks of newspapers, magazines, prescriptions, doctors' letters, and drug packaging were placed in the rooms in an attempt to emulate the kind of environments emergency physicians encounter when responding to emergencies at patients' homes.
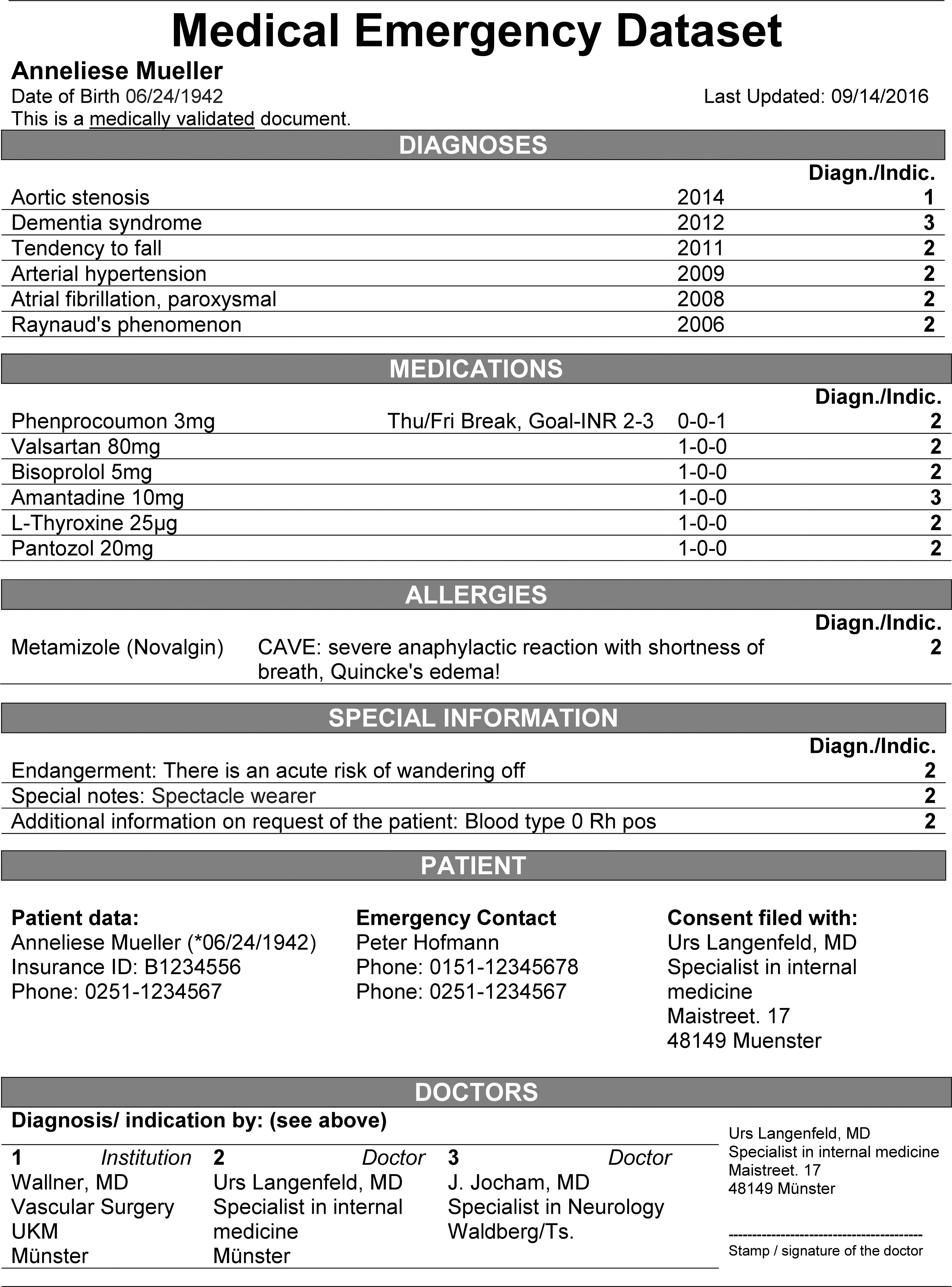
Example of a Medical Emergency Dataset as provided in scenario A—translated from the original German document used in the first trial. INR, international normalized ratio; Rh pos, rhesus positive; UKM, University Hospital Muenster.
There was no additional information to gather from the environment in the second trial. In all settings, SPs could not give explicit information about their condition, even when asked. In the second trial, only if an emergency physician asked a family member or acquaintance about a specific piece of information (i.e., allergies, medications, and pre-existing conditions/information), and only if their assumption was correct, would the actor confirm their suspicion.
Participant Recruitment
A website was created where emergency physicians would get a brief description of the study and could apply for participation. Six weeks before each trial, a link to the recruitment site was shared on the official website and social media of the Emergency Physician Work Group of North Rhine-Westphalia (AGNNW). Included in the trials were individuals with at least 1 year of experience working as an emergency physician and who had no detailed prior information about the study design.
Thirty-six emergency physicians were recruited for each trial, each participating in one of the two trials. Data integrity and security concerns regarding videotaping the simulated scenarios and evaluations were addressed during a prebriefing and described in a brochure, which had been sent to the participants.
Data Sources
The video material from cameras in the simulation room and the secluded booth was synchronized according to the actual timeline of the scenario and saved as a movie file. A pair of experts, comprising a physician from the study team (L.W.) and an external emergency physician, evaluated the videotaped scenarios according to predefined checklists. In addition to the unwanted preclinical action (e.g., giving nitroglycerine to a patient with coronary syndrome who took sildenafil), the documented key pre-existing conditions and information, medications, and allergies of the patients were scoring items in the scenarios for each participant.
In this study, it was essential, that the key items were either documented (1) in the handover protocol, 11 (2) by referencing corresponding documents (e.g., doctor's letter), or (3) by mentioning them in the video protocol in the handover booth. The number of key items documented was scored to assess the comprehensiveness of the handover process between the settings. In the Supplementary Data, the management and processing of the study documentation are discussed.
Statistical Methods
Both studies were planned as AB/BA crossover trials to analyze the impact of the MED on the actions of emergency physicians. The primary outcome (not reported in this article) was avoidance of unwanted medical procedures that were defined for each scenario. Power analyses were conducted to ensure that (with 36 participants) a power of about 80% would be achieved to detect a difference of 25–50% versus 5–10% of undesirable procedures in scenarios without versus with MED, respectively. For the power analysis, a computer simulation study was conducted, with individual probabilities for unwanted medical procedures for each scenario within the aforementioned ranges.
To account for the crossover nature, p-values for the influence of the MED on documentation of key items in the simulation runs were computed using the two-sided Prescott's exact test. 12 For simplicity's sake, results are presented separately for simulation runs with and without MED. Possible period effects were analyzed with a two-sided Mainland–Gart test. 13 Further sensitivity analyses adjusting for the scenario were conducted using generalized estimating equations. p-Values ≤0.05 presented in this article are considered statistically noticeable, but all inferential analyses presented are nevertheless considered exploratory since only the analysis of the primary endpoint was considered confirmatory.
All statistical analyses were performed using SAS® software, version 9.4, for Windows (SAS Institute, Cary, NC).
Results
Study Population
Participants showed no relevant differences in both randomized groups in the two trials. In the first trial (n = 36), participants were aged 40.2 ± 8.1 (mean ± standard deviation) years, 58% female, and with median 5.5 years (interquartile range [IQR] 3.5–9.5 years, range 1–27 years) of experience in EMSs. In the second trial (n = 36), participants were aged 39.5 ± 7.1 years, 28% female, and with 5 years (IQR 2–10 years, range 1–26 years) of experience in EMSs.
Comprehensiveness of Anamnesis
Table 2 shows the results for the documentation of key items in the first trial, comprising data from all three scenarios. For all results displayed in the table, no relevant influences by the scenarios or statistically noticeable differences between periods were found. Overall comprehensiveness of anamnesis for the past medical history (combined with key pre-existing conditions/information, key allergies, and key medications) in the first trial was more complete in scenarios with MED (19/36 vs. 4/36; p = 0.0002). When adjusted for scenario, the analysis shows evidence for the existence of a period effect (p = 0.0421). Documentation in the second run is often more complete in comparison with the first run (15/36 vs. 8/36 runs).
Results for the Documentation of Key Items at the End of the Three Scenarios (A+B+C), Displayed for All Simulation Runs in Both Trials (1st Trial n = 36 participants and 2nd Trial n = 36 participants)
Calculated with the two-sided Prescott's exact test.
Documentation could mean: (1) a handwritten handover protocol, (2) reference to corresponding documents (e.g., doctor's letter), (3) mentioning them in the video protocol, or (4) any combination of the aforementioned points.
In the second trial, only if an emergency physician would ask an actor about the correct key item, the actor would provide the information.
MED, medical emergency dataset.
The results concerning the effects of MEDs on the documentation of key information were confirmed in the second trial. This was to be anticipated as no additional information could be obtained from the environment this time. To further illustrate the impact of MEDs, a descriptive analysis of the documentation in both trials can be found in Table 2.
Questionnaire
Figures 2 and 3 show the results of a questionnaire regarding the emergency physicians' opinions on different aspects of the MED. Overall, the participants gave positive feedback about the MED.

Emergency physicians' opinions on the comprehensibility of the information provided in the MED (1st trial n = 35 and 2nd trial n = 34).
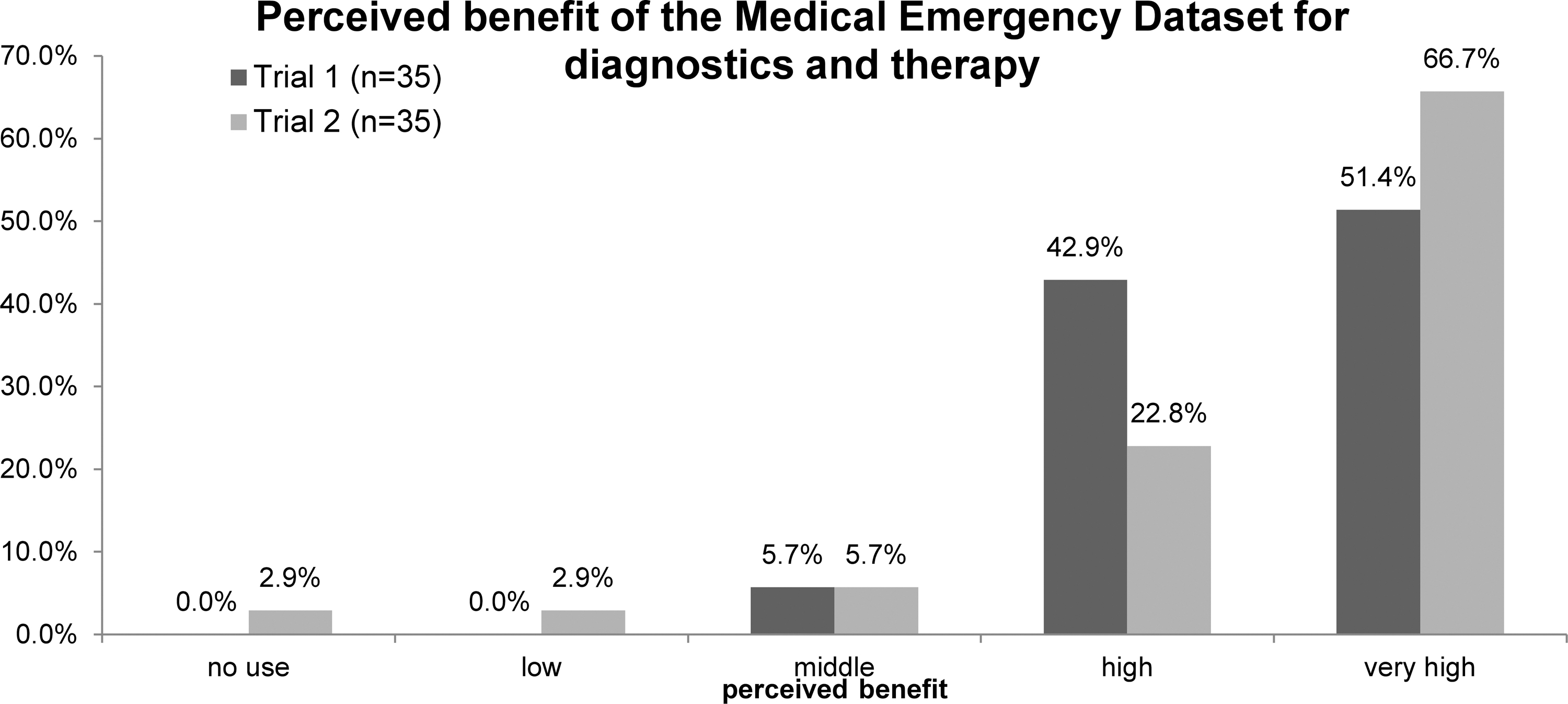
Emergency physicians' perceived benefits of the MEDs for diagnostics and therapy (1st trial n = 35 and 2nd trial n = 35).
Discussion
In both trials described in this article, the comprehensiveness of an emergency physician's handover to the hospital was compared in simulated emergency scenarios with and without an MED present on the scene. Results show the documentation of key items after each simulation run was more complete overall in scenarios with an MED. In the first trial, two of three key items (pre-existing conditions/information and allergies) showed a statistically noticeable difference in scenarios with an MED. The second trial confirmed these results for all described key items (pre-existing conditions/information, medications, and allergies). For the second trial, it was decided that participants were previously informed about the concept of the MED, but would not have any additional patient health information available to them in the scenario environment. While not having this information accessible may have been a major hindrance, these conditions were implemented to highlight the possible benefits of an MED for the primary outcome (identifying unwanted preclinical actions). The trials are, however, still considered comparable with one another due to the scenarios being nearly identical and there were only small variations in the trials' setups. The reported findings for both trials indicate that the use of MEDs in emergency care could be beneficial since the documentation and handover to the (fictional) clinic in scenarios with MED were superior. Additionally, participants of the trials perceived the benefits of MEDs for diagnostics and therapy mostly as “high” or “very high.” In 2015, Born et al. have reported similar positive results for the perceived overall benefits of MEDs by emergency physicians, clinicians, and paramedics. 10
Despite the promising findings, several limitations should be mentioned. First, the crossover design was chosen to realize a sufficient number of simulation runs despite the small number of participants caused by the limited funding and capacity. This doubles the number of scenarios examined when compared with a hypothetical parallel-group trial with the same number of participants.
Taking the crossover design into account, statistical analyses yielded valid results even in the presence of a period effect. The analyses did not provide any indication that a carryover effect existed. However, since a carryover effect cannot be ruled out, it is unclear if the chosen crossover design is fully appropriate in this setting.
Second, the MEDs used in the scenarios were paper based, unlike the planned implementation with EHC storage. Any influence that technology (e.g., card readers) might have could therefore not be considered. However, we focused on the impact this compacted information might have on day-to-day practice in EMSs, where generally no structured health information is available.
Third, misinterpretation by the experts during the conducted video analyses cannot be ruled out. Therefore, two experts had to make joint decisions to minimize this risk. A similar approach in a simulation study has been described previously. 14
Fourth, simulated emergency scenarios with actors and SPs are not able to fully imitate real emergency situations. Moreover, the individual behavior of the SPs and actors can also differ in parts between the runs and might thereby influence comparability, regardless of a scripted scenario. The simulations were also exceptional situations for the participants, involving videotaping and an examination-like situation. Interpretation of findings and any attempts at generalization or transfer of results to clinical practice should therefore be done with caution. Nevertheless, comparable experimental setups of simulation studies and general use of simulations in prehospital research have been described earlier. 14 –16
Last, some potential limitations in the real-world usage of the MED itself need to be mentioned. Since it is stored on an EHC, there is always the possibility that a patient might misplace the card or is unable to tell the emergency team where the card is located. It is therefore suggested that emergency teams be informed about the most frequent locations where patients keep their health cards as part of an additional MED training course. Patients with an MED should also be advised by their general practitioner about where best to keep their EHC at home or while on the road.
While implementation of MEDs had previously been scheduled for the beginning of 2018, 17 rollout has been prolonged by technical and legal hurdles. Suitable card readers are now obligatory in doctor's practices and are currently being rolled out. 18 By mid-2020, patients should be able to choose to store their MED on their EHC. 9 The continued research of MEDs is therefore strongly recommended. Field tests in prehospital EMSs are encouraged once the necessary technology has been implemented.
Footnotes
Acknowledgment
The authors thank Phillip Arthur Lloyd Swayne for proofreading the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the European Union and the Ministry of Health, Equalities, Care and Ageing of the State of North Rhine-Westphalia (MGEPA
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.