
Abstract
Purpose:
To evaluate attitudes and perceptions toward virtual health (VH) and its usage among eye care providers before, during, and after the coronavirus disease 2019 (COVID-19) pandemic.
Materials and Methods:
In April and May 2020, an online survey comprised of questions regarding past and current VH practices, as well as plans for future use was distributed among eye care providers nationwide.
Results:
Of the 117 eye care providers who completed the survey, 96.6% were not using VH before the COVID-19 pandemic. In contrast, 77.4% reported using VH during the pandemic. The majority of visits were for red eye (64.4%, n = 56) and ocular surface complaints (58.6%, n = 51). Examination components tested virtually varied, but most respondents felt these were at least “somewhat reliable.” Almost half of respondents (45%) felt it was “very easy” or “somewhat easy” to implement VH and the majority (53.8%, n = 43) were able to get it up and running in under a week. The majority felt the transition to VH was positive (57.5%), however, only 50.4% (n = 53) of those providers planned to use VH regularly once able to see patients safely in clinic again.
Conclusions:
While the majority of U.S. eye care providers who responded were not using VH before the COVID-19 pandemic, just months into the U.S. outbreak, 77.4% were using VH in their daily practice. In general, providers used these platforms for urgent examinations, adnexal disease, and postoperative care most often. The majority felt the transition was a positive one, however, only half planned to continue regular use of VH once the pandemic ended.
Introduction
In early March, with the arrival of the coronavirus disease 2019 (COVID-19) pandemic in the United States, medical practices faced unprecedented challenges in delivery of care. To protect patients, providers, and staff, medical associations in addition to state and national legislatures released urgent and sweeping recommendations urging eye care providers to cease in-person evaluations for nonurgent issues. Thus, practices were limited to treating only urgent and emergent ophthalmic issues. With extended inability to care for patients in need, financial difficulties looming, and no definitive end to the pandemic in sight, practices faced another challenge: how to continue necessary care for patients while also staying afloat from a financial perspective. Thus, providers and practices across the country turned to virtual health (VH) for assistance.
Telemedicine has been used in primary care and other specialties for years where it has been used effectively and efficiently, especially in rural communities or where access to providers is limited. In eye care, however, its implementation has been slower. A 2017 review demonstrated that the majority of ocular telehealth services function via a “store-and-forward” methodology where patient images are taken and sent to a remotely located eye care professional. This technique is used in some emergency department settings across the country and has been used for screening of some chronic ophthalmic diseases where access to eye care providers is limited. 1 –4
While some previous investigations have shown this to be cost-effective and useful, its routine use in eye care before the COVID-19 outbreak was not widespread. 1,2,5 Barriers encountered include the need for expensive and high-quality imaging equipment as well as cumbersome Health Insurance Portability and Accountability Act (HIPAA)-compliant/secure imaging communications software. This method of VH also relies on primary or emergency care providers to perform examinations they may not be trained to complete and shifts the imaging burden to the treating provider. 1 Furthermore, these “store-and-forward” services still require in-person patient contact to obtain images, which was brought to a halt during the pandemic. In addition, not all eye care providers feel comfortable interpreting these images and providing recommendations remotely. 5
Reimbursement for telemedicine has also been a barrier to adoption as coverage for such services varied greatly and was notoriously limited by Medicare. 1 There have also been legal implications, centered around state licensing and credentialing as well as HIPAA regulations, which have limited VH's use and availability. Many of these barriers have been minimized since the pandemic began, however. For instance, the Center for Medicare and Medicaid Services and HIPAA regulations on telehealth were eased early on in the COVID outbreak. 6,7 Given these allowed changes and the rapid expansion of telehealth services, we sought to evaluate attitudes toward VH and its use among eye care providers before and during the pandemic, as well as opinions toward expected practices after the COVID-19 pandemic.
Materials and Methods
This project adheres to the Declaration of Helsinki, was reviewed by the University of Colorado Multiple Institutional Review Board, and was ruled exempt. An online survey (SurveyMonkey; Supplementary Appendix SA1) was sent out on multiple occasions between April 9 and May 17, 2020, to eye care providers nationwide through e-mail and list-serves associated with Ophthalmologic and Optometric Societies after appropriate approval was obtained. Specifically, it was sent to the American Glaucoma Society (AGS) and the American Society of Cataract and Refractive Surgeons (ASCRS). The total number of providers in each list-serve is 1477 for AGS and 6800 for ASCRS with some members in both groups.
The survey included questions regarding VH practices before and during the pandemic, as well as plans for future use after. It also included questions regarding which patients were seen by providers using a VH platform and sought to identify the examination components tested and investigate opinions on the reliability of these measurements. In addition, there were questions on diagnostic testing obtained as well as cleaning protocols of devices during the pandemic. On June 30, 2020, the survey was closed and the responses were evaluated. Basic frequencies and percentages were reported for all survey responses provided. Missing data varied for each survey question and were minimal.
Results
A total of 117 providers completed the online survey between April 9 and June 30, 2020. Completion rate, defined as respondents who completed the entire survey after starting, was 91% and average time to complete the survey was 3 min and 50 s. As shown in Table 1, the majority of respondents (n = 105) reported working in an academic setting (36.2%, n = 38), followed by providers in large private practice groups (22.9%, n = 24) and small private practice groups (21.0%, n = 22). Responses regarding number of years in practice varied.
Characteristics of Responders and Past, Current, and Future Use of Virtual Health
COVID, coronavirus disease; MD/OD, Doctor of Medicine/Doctor of optometry; VH, virtual health.
The majority of respondents were not using VH before the COVID-19 outbreak. Of the four respondents using VH before the pandemic, only 1 was using video visits. Others reported using telephone calls (n = 3) or secure messaging over a patient portal (n = 2). In contrast, 77.4% (n = 89/115) reported using VH at the time of survey completion. Frequency of VH visits varied with most providers answering either “several times per week” (49.4%, n = 43/87) or “rarely” (24.1%, n = 21/87) (Table 1). A majority of respondents reported using video visits (83.9%, n = 73/87) and telephone calls (90.8%, n = 79/87) as their primary VH modality. Secure and nonsecure e-mails and secure messaging over patient portals were also used. Video platforms used (n = 84) included Doximity video (31.0%), Doxy.me (27.4%), Zoom (26.2%), FaceTime (25.0%), platforms integrated into EPIC/HAIKU/CANTO (11.9%), and more rarely, Skype (3.6%), Amwell (2.4%), Otto Health (2.4%), and WhatsApp (2.4%).
Regarding the type of ocular issues respondents (n = 87) treated via VH, the most common responses were acute red eye (64.4%, n = 56/87), ocular surface issues/complaints (58.6%, n = 51/87), eye pain (47.1%, n = 41/87), glaucoma (43.7%, n = 38/87), and postoperative patients (39.1%, n = 34/87). Other responses included annual examinations, cataracts, diplopia, diabetic eye disease, macular degeneration, uveitis, and eyelid/oculoplastics issues although these were less common, all reported by 11 respondents or less (Fig. 1).
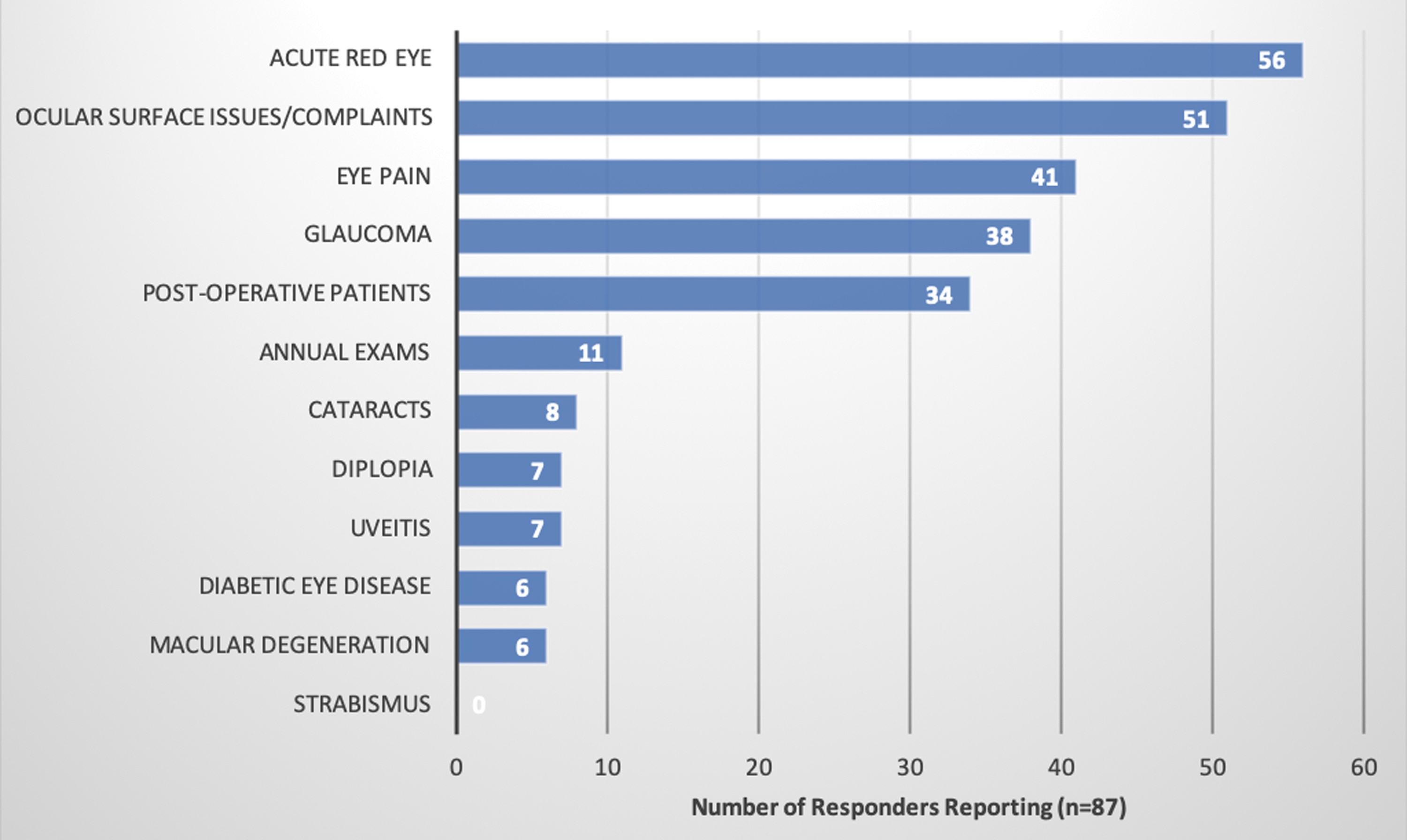
Which diseases have you followed and/or treated through virtual health platforms?
Concerning ocular examination components assessed during VH visits, the majority of respondents were not checking visual acuity (VA) routinely. Of 86 questioned respondents, 53 (61.6%) answered that they checked VA rarely or never. Only 2.3% (n = 2) reported checking VA routinely (Table 2). VA, when assessed, was checked via an eye chart the patient pulled up on the computer (31.2%, n = 15/48), a printable eye chart sent to the patient (29.2%, n = 14/48), or via an app that the patient downloaded (18.8%, n = 9/48). Other responses (n = 10/48) included a subjective report of the patient's vision and using readily available reading material such as a newspaper or magazine. No respondent felt that VA testing via these virtual methods was “very reliable,” while 50.0% (n = 24/48) felt this was “somewhat reliable” (Table 2). Other examination components routinely checked during VH visits are listed in Figure 2. Of these, external examination/lids and lashes (81.7%, n = 67/82), conjunctiva and sclera (74.4%, n = 61/82), mood and affect (65.9%, n = 54/82), and extraocular movements (54.9%, n = 45/82) were the most common answers. Similar to the VA assessment, the majority of providers felt this evaluation was “somewhat reliable” (51.2%, n = 42/82), while another quarter felt it was “somewhat unreliable” (26.8%, n = 22/82) (Table 2).
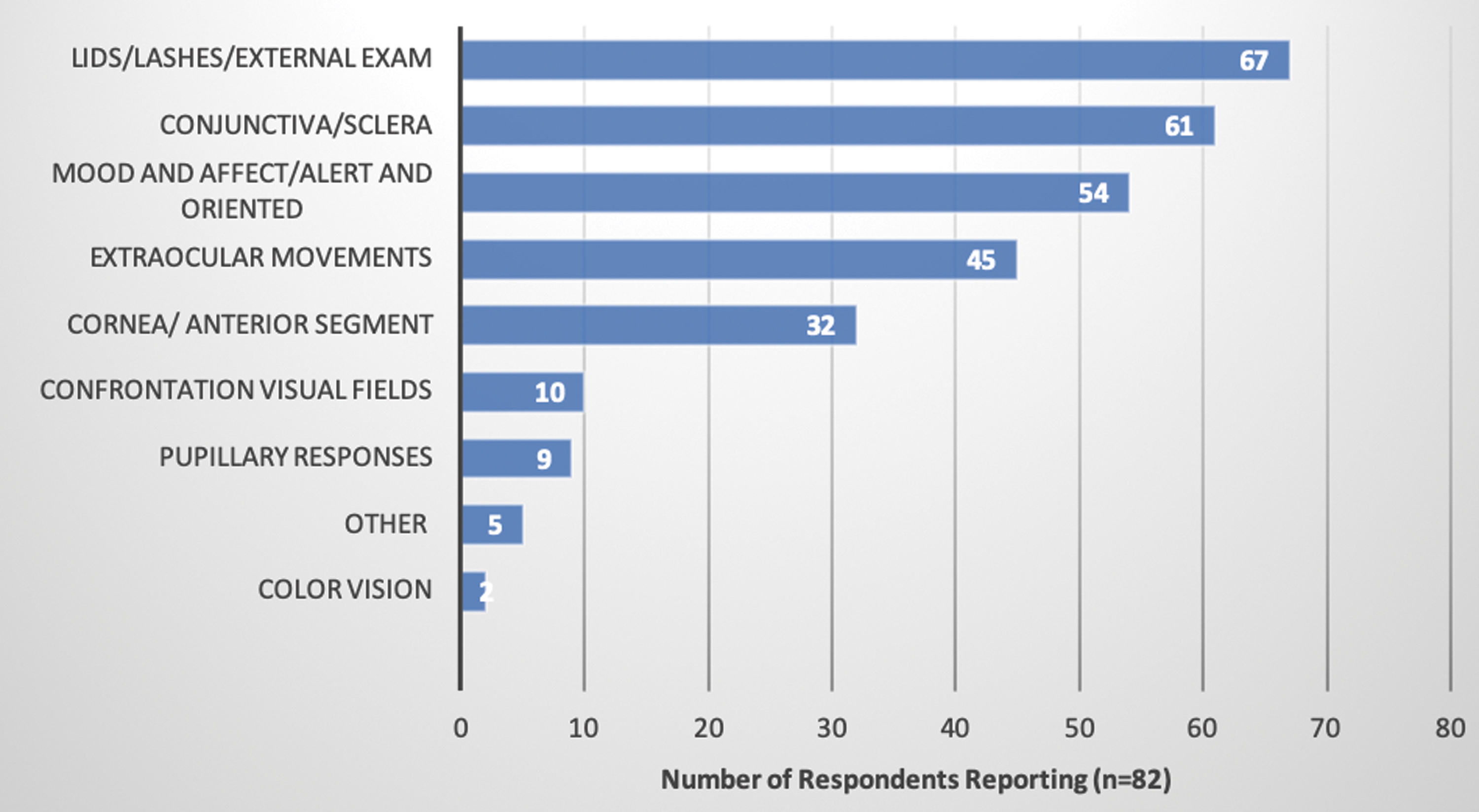
Which other examination components do you routinely check on telehealth visits?
Visual Acuity and Other Ocular Assessments via Virtual Health
VA, visual acuity.
Given the difficulties with assessment of certain examination components and obtaining diagnostic tests virtually, we asked whether hybrid visits comprising a limited in-person visit (for testing, VA only) with a subsequent virtual visit were performed. These hybrid-type visits were performed by 30.1% (n = 25) of the 83 respondents, while 66.3% (n = 55) did not perform these. For urgent patients who required an in-person visit, 41.9% (n = 44/105) of respondents were still obtaining diagnostic testing on any patient they normally would have, while another 41.9% (n = 44/105) were only obtaining testing on patients in whom there was concern for progression of disease. A minority of respondents (6.7%, n = 7/105) stopped all testing or obtained testing only on rare occasions (9.5%, n = 10/105).
Given the risk of contamination of imaging machines, we then asked whether providers who were obtaining imaging had changed their protocols or setup. Of 98 responders, 62.2% (n = 61) stated they changed nothing, 11.2% (n = 11) were unsure, and 26.5% (n = 26) responded that they had made changes. These changes included but were not limited to disinfecting machines after use, social distancing, installing new air filters, extending the time between each patient and/or each test, rotating or limiting which machines were used, moving machines to separate rooms or increasing spacing between machines, limiting the number of tests per day and/or per patient, requiring patients to wear masks during testing, adding plastic shields to machines, and limiting the number of patients and staff members allowed in the room. While many respondents answered they were limiting the number of tests per day or increasing the amount of time between each test, 58.6% (n = 58/99) stated their practice either did not have an official protocol in place or were unsure regarding protocols. Cleaning wipes or solutions used for disinfection varied, and included CaviWipes, alcohol wipes/solutions, Clorox and Lysol wipes, and bleach.
Regarding ease of VH implementation into practice, the 80 responding providers were split (Table 3). Those who felt implementation was either “very easy” or “somewhat easy” made up 45.0% (n = 36) of respondents, while another 40.0% (n = 32) felt it was either “very difficult” or “somewhat difficult.” Implementation and training of staff were relatively swift though. The majority (53.8%, n = 43/80) were able to get VH running in their practice in under a week and 37.5% (n = 30/80) said it took “one to three weeks.” Furthermore, training staff took <5 h for the majority of providers (81.0%, n = 64/79).
Questions Regarding the Specifics of Incorporating Virtual Health into Practice
The primary reported limitation to implementation centered around examination and testing (87.5%, n = 70/80). A significant number also felt they had difficulty understanding how VH fits into their practice (52.5%, n = 42/80), it was unclear which patients to use VH on (45.0%, n = 36/80), or they had trouble running the visits (37.5%, n = 30/80). Other limitations reported (n = 23/80) were pushback from staff, partners, or elderly patients, financial constraints, lack of compatible technology on the patient side, administrative issues from overseeing authorities, and difficulties with consenting patients and patient expectations.
Despite these difficulties, 57.5% (n = 46/80) felt the transition to VH was a positive one (Table 3). As shown in Table 1, predicted future use of VH after the pandemic varied from “never” to “routinely,” but over half of respondents to this question (50.4%, n = 53/105) planned to use VH “routinely” or at least “sometimes,” although definitions of these plans were not further investigated or defined by the survey. Furthermore, despite this plan for about half of respondents to continue using VH at some level postpandemic, most of the responding providers still felt that after the pandemic “less than 5%” of their visits would remain VH (46.8%, n = 44/94) and no provider thought that >30% of their visits would remain virtual.
Discussion
The COVID-19 pandemic brought about rapid and widespread changes to the health care system, the most dramatic of which was likely the urgent cessation of all elective and nonurgent care. During these times, VH has been one avenue adopted to maintain some level of care for patients in need. In this study, we describe the attitudes toward VH, the frequency and type of usage, and predicted future utilization of VH within eye care. This is the first survey to our knowledge to evaluate attitudes toward and usage of VH within eye care that is not limited to a “store-and-forward” methodology.
In our survey, only 4 of 117 eye care providers were using VH routinely in practice before the pandemic. Despite its relative novelty in our field, however, providers across the country quickly understood the practicality and opportunities VH offered, with the majority of respondents using VH in their practice at the time this survey was collected (77.4% of 115 answering providers). Although it is important to note that still almost 23% of responding providers were not using VH, even in the midst of the pandemic, when most routine eye care was prohibited or at least urged not to occur.
Still, these results highlight the increase in VH visits, specifically real-time video visits, performed during the pandemic, compared with prior eye care. Before the pandemic, only 1 respondent was using video visits. Whereas during the pandemic, 73 of the 87 (84%) providers who were using VH and answered the question on which forms of VH they were currently using were employing video visits. In light of the difficulties placed on medical practices during this time, penalties for violations of HIPAA were relaxed, thus allowing practices to use communication services not previously available to them for VH. Despite these relaxed regulations, the two most commonly used video platforms in our survey were Doximity video and Doxy.me, both HIPAA-compliant platforms. The next most commonly used platforms, however, were Zoom and FaceTime, which are not HIPAA compliant unless a specific Zoom health care version is purchased.
One of the VH services available to some extent in eye care before the pandemic was remote consultation for eye care triage and emergency services. 1,4 Our results mirror this as the most commonly treated ocular complaints in our cohort were acute and triage issues such as red eye, ocular surface complaints, and eye pain. Nonetheless, glaucoma care, chalazion and eyelid issues, and postoperative patients also made up a significant number of issues addressed by responding providers, demonstrating the capabilities of VH beyond urgent eye care.
Despite the fact that before the COVID-19 pandemic, telehealth use in eye care was only in its infancy, respondents were able to implement these new practices somewhat rapidly and with ease. A majority of answering providers (57.5%) endorsed that the transition to VH was a positive one and a high proportion (45%) of those felt it was easy to implement into their practice. The majority were able to have VH up and running within a week and have staff trained to assist with virtual visits within a few hours. Still, some providers had difficulty. In fact, 35% reported it was “somewhat difficult” to implement VH in their practice.
Responses varied with regard to future plans to use VH, but it is important to note that 50.4% of respondents answered they planned to use VH either “sometimes” (39%) or “routinely” (11.4%) even after being able to see patients safely in clinic again. While these responses were not further defined in this survey, this is still a significantly greater proportion of respondents than those who reported using VH routinely before the pandemic (3.4%) and highlights the potential for further expansion of VH into eye care.
Moving forward, VH still has limitations to overcome in eye care. Respondents encountered difficulty understanding the role of VH and which patients these visits are best suited for. Logistical issues, technologic limitations, and administrative and billing issues were also encountered. Previous surveys have demonstrated that 82% of eye providers were willing to participate in telemedicine, even pre-COVID-19. However, that same survey also reported that 59% were not confident in their ability to provide an opinion on patient care via these mechanisms. 3,5 Some of this hesitancy likely lies in the inherent limitations of ocular examinations via virtual media. In our survey, the majority of respondents felt that assessing VA and other examination components was only “somewhat reliable” and a high proportion felt it was “somewhat unreliable.” Furthermore, 87.5% of answering providers identified examination and testing limitations as a primary barrier that parallels the findings of this previous study. Some currently available technology could improve this. For glaucoma patients specifically, home monitoring of intraocular pressure can be performed via the iCare Home and Sensimed Triggerfish contact lens sensor and at-home and virtual reality visual field tests are also available for disease monitoring, but these have not yet been widely adopted clinically. 8,9 Retinal cameras, smartphone, and ophthalmoscope adaptors are also commercially available to capture and send photographic images, providing another imaging option for hybrid-type VH visits in the future. 8
Early in the pandemic, no specific guidance was provided regarding the use of imaging and testing modalities or cleaning protocols. Thus, as expected, when queried regarding the use of diagnostic testing, responses were split. Furthermore, there was no consensus on cleaning or social distancing protocols with regard to diagnostic equipment, although many respondents did list changes they used to spacing of machines, testing protocols, or sanitization procedures. This highlights the need for additional guidance as information regarding contamination rates and appropriate cleaning protocols emerges.
A major limitation of this study is the small sample size (N = 117). The survey was distributed to 1477 members from the AGS and 6800 members from the ASCRS, in addition to other e-mail distributions, but the response rate was low. However, a response rate could not accurately be calculated as the true denominator is unknown because of significant overlap in members between the groups. Furthermore, variations in practice by geographic location and between rural and urban areas could not be assessed as the geographic location was not captured. In addition, limitations to reimbursement for telemedicine services have been a suggested barrier to adoption of VH in the past. 1 Furthermore, strict rules around state licensing and patient privacy exist, which may limit a provider from caring for a patient outside of the state where he or she practices and is licensed. 1,6 Financial and legal effects or motives were not directly evaluated in this study.
Future directions include investigation into regional differences in VH usage and attitudes and the effects of reimbursement changes on adoption. This survey was conducted as the first phase of the pandemic was beginning to transition and practices were getting notifications that they could resume care for routine issues. Therefore, responses regarding the future use of VH may be an underestimation of future VH visits. As the pandemic continues and we face the second wave of infections and closures, it will be important to readdress this issue and assess how attitudes and usage evolve.
Conclusions
The COVID-19 pandemic spurred a rapid expansion of telehealth services. Before the pandemic, the vast majority of eye providers who responded to our survey were not using VH. However, within just weeks of the outbreak, more than 3 out of 4 providers were using VH for triage, acute care, or other reasons in their practice. Most providers felt that the transition was positive and relatively easy, with some notable difficulties, and a substantial number of providers predict they will use some form of VH in their practices moving forward. Still, significant limitations exist around imaging and testing capabilities, including basic ocular examination components. Future technological advances may improve the quality and ability to perform a detailed ophthalmic examination through VH platforms and would facilitate more widespread adoption in our field.
Footnotes
Authors' Contributions
C.E.C.Y., L.K.S., and M.Y.K. contributed to the creation of this project. J.L.P. and C.E.C.Y. analyzed and interpreted the survey data. All authors reviewed the data, contributed to, read, and approved the article, including the tables and figures.
Disclosure Statement
The authors certify that they have no financial or nonfinancial conflicts of interest to disclose.
Funding Information
This work was supported by a challenge grant to the Department of Ophthalmology from Research to Prevent Blindness, Inc. The sponsor or funding organization had no role in the design or conduct of this research.
Supplementary Material
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.