
Abstract
Introduction:
The nationwide shortage of pediatric cardiologists in medically underserved areas poses a challenge to congenital heart disease (CHD) screening requiring echocardiography, resulting in transfer of neonates to regional Level III/IV Neonatal Intensive Care Units (NICUs). This study aimed to evaluate the accuracy, safety, and cost-effectiveness of tele-echocardiography for advanced CHD screening at a Level II NICU managed by a hybrid telemedicine system.
Methods:
Retrospective chart review of infants requiring tele-echocardiography at a Level II NICU. Patient demographics, echocardiography indications, and findings were analyzed. Agreement between tele-echocardiography and conventional echocardiography findings was assessed. Transport cost savings were calculated based on preventable transfers to Level IV NICU. Descriptive statistics were computed for demographic and clinical variables.
Results:
Over 5 years, 52 infants were screened for CHD. Thirty-two infants (62%) had findings consistent with minor CHD or normal neonatal transitional physiology. Twenty infants (38%) had abnormal findings requiring follow-up with either a conventional echocardiography as inpatient at the regional Level IV NICU or as outpatient after discharge. Only 5 infants (10%) required transfer to a Level IV NICU for CHD management, whereas 15 infants (29%) were scheduled for outpatient follow-up. Strong agreement was noted between tele-echocardiography and conventional echocardiography findings. No case of critical congenital heart disease (CCHD) was missed. Tele-echocardiography saved $260,000 in transport costs.
Conclusions:
Tele-echocardiography can be accurate, safe, and effective in CHD screening, preventing unnecessary transfer of most infants to regional Level III/IV NICUs, saving transfer costs.
Introduction
Congenital heart diseases (CHDs) remain one of the most important causes of infant mortality and are responsible for 1 out of 18 infant deaths. 1 The global prevalence of CHDs, especially mild types, has significantly increased over the past decade, whereas the prevalence of other types has remained stable. 2 The current incidence is about 8–10 per 1,000 (0.8–1%) live-born, full-term births, and it is around 10 times higher in preterm infants (8.3%). 3 –5
Approximately 25% of babies with CHD have a critical CHD (CCHD) and they often require surgery or other interventions during infancy. 2 The prenatal detection rate for CHD remains low and variable (range 11.8–53.4%). 6 Although many newborns with CCHD are symptomatic and identified soon after birth, others are not diagnosed until after discharge. Delayed diagnosis can result in increased morbidity and mortality. 7
Universal newborn screening for CCHD using pulse oximetry is widely recommended. 8 –10 A positive CCHD screening requires prompt evaluation with echocardiography interpreted by a pediatric cardiologist. In addition, echocardiography may be required for infants who may present with an isolated murmur or infants with significant respiratory distress to rule out CHD. 11 With pediatric cardiologists being scarce in rural areas, these infants are often transferred to facilities offering a higher level of care. 12
Increasingly, telemedicine has proven to be effective globally at linking resource-poor regional hospitals with tertiary medical centers offering services, including pediatric cardiology and advanced neonatal care. 13 –16 More recently, with the COVID-19 pandemic, telemedicine has increased in utility and acceptance worldwide. 17 –23 Telemedicine with remote interpretation of echocardiograms could be an effective option for determining which neonates require urgent transfer to a tertiary care center. 14,24 This approach supports an integrated web model of pediatric health care regionalization where telemedicine averts the need for transfer. 25
In 2013, neonatologists at an Oklahoma City academic center with a Level IV Neonatal Intensive Care Unit (NICU) started providing specialty NICU care at a hospital with a Level II NICU. Historically, this rural hospital provided neonatal services with the support of local pediatricians. In recent years, to improve the quality of neonatal care and in compliance with the American Academy of Pediatrics (AAP) recommendations, in-house neonatal services were made available utilizing a hybrid form of telemedicine. 26
This hybrid telemedicine system provides 24/7 neonatal nurse practitioner (NNP) coverage in the NICU and the delivery room. The covering neonatologist rounds in-person 3 days a week and off-site the remaining 4 days through telemedicine, including emergencies. This system allows an off-site neonatologist to manage patient care by coordinating with an on-site NNP. Unlike standard telemedicine programs, this initiative combined traditional and telemedicine patient–neonatologist encounters. The implementation and achievement of this program has been presented elsewhere. 27,28 Building on the success of this original project, this program expanded to include telemedicine for retinopathy of prematurity screening. 29,30 In 2014, the hybrid system expanded again to implement advanced CHD screening, which sometimes resulted in patients' transfer to the Level IV NICU. The goal of this study was to assess the accuracy, safety, and cost-effectiveness of conducting tele-echocardiography for advanced CHD screening of infants in a Level II NICU managed by a hybrid telemedicine system.
Methods
This retrospective study assessed the use of tele-echocardiography in screening for CHD in infants at Comanche County Memorial Hospital (CCMH) in Lawton, Oklahoma. CCMH, a community medical facility about 90 miles (145 kms) southwest of Oklahoma City, has an 8-bed Level II NICU serving a busy maternal delivery unit with >1,200 newborn deliveries per year. The Department of Pediatrics' Section of Neonatal and Perinatal Medicine, located at the University of Oklahoma Medical Center (OUMC) in Oklahoma City, manages the telemedicine program for CCHD screening. This study involved a convenience sample of infants evaluated for CCHD using telemedicine from January 2015 to December 2019.
The Institutional Review Board (IRB) at OUMC and the research committee at CCMH approved the study, granting a waiver of informed consent because the data were collected retrospectively from electronic medical records (EMRs).
Inclusion Criteria
Infants who meet AAP criteria for Level II NICU care and (1) who failed AAP-endorsed CCHD screen through pulse oximetry or (2) had signs and symptoms concerning for possible CHD. 31
Exclusion Criteria
Infants transferred to a regional Level IV NICU because of the following criteria: (1) infants hemodynamically unstable or (2) infants who were concerning for CCHD and required to be transferred to level IV NICU for urgent echocardiography and management.
Imaging Personnel and Procedure
Our group utilized interactive or real-time telemedicine for CHD screening, as sonographers at CCMH had no or little experience in performing echocardiography in the neonatal population. When tele-echocardiography was indicated, the NNP on call in the NICU at CCMH contacted the Children's Heart Center at OUMC and arranged a time for a pediatric cardiologist to be available for the tele-echocardiogram. Overall, four sonographers at CCMH performed echocardiography and five pediatric cardiologists at OUMC were involved in remote interpretation. The in-house echocardiogram sonographer at CCMH was notified and arrived 15–20 min before the tele-echocardiography to connect with the Polycom® HDX 7000 unit (Poly, Inc.) in the NICU. The echocardiograms were performed on a GE machine using 8 and 12 Hz probes. Images were obtained in the standard long axis, short axis, four chambers, suprasternal, and subcostal views. M mode was obtained to assess cardiac function. Images were transmitted from CCMH to OUMC through T-1 and T-3 lines at a bandwidth of 768 kilobits per second. After reviewing the initial images, the cardiologist then guided additional imaging in real time with instructions on optimal image utilization for confirmation of diagnosis. Given the live or synchronous nature of the system used, none of the echocardiography required repetition due to poor image quality. A verbal report of the results was given to the NNP or the attending physician in the NICU. If the attending neonatologist was not present, the results were verbally communicated by the NNP. Final results were shared with the infant's family by the NNP or the attending physician on service. A formal echocardiography report was then uploaded into the CCMH EMR within 24 h of the imaging procedure.
Follow-Up Strategy
The degree and severity of the heart disease determined the follow-up strategy. Infants with no CHD required no follow-up; those with minor CHD required follow-up in an outpatient setting upon discharge, whereas patients with major CHD were urgently transferred to the regional Level IV NICU at OUMC for further management.
The study team developed a scoring system for the accuracy of the tele-echocardiogram results by comparing the tele-echocardiography with conventional (transthoracic) echocardiography findings, performed at either at a Level IV NICU in Oklahoma City, Oklahoma, or in an outpatient setting. A cardiologist compared the in-person echocardiography findings versus those completed through telemedicine and assigned an agreement score. An agreement score of 1 indicated perfect agreement between studies or expected lesion resolution based on the clinical course. A score of 2 reflected minor disagreement between the findings that did not affect patient management. A score of 3 was assigned if the follow-up study revealed a different finding or a new clinically important finding.
Transport Cost Savings
According to our institutional policy, any transport from hospitals >45 miles away is done through air transport, as we have one neonatal transport team that serves infants all over the state of Oklahoma. We calculated transport cost savings by multiplying the total number of study patients at the satellite Level II NICU by the standard transport cost per patient. Following our institutional transport guidelines, all patient transfers for the study cohort would qualify for air transport. The transport cost per patient was calculated as base cost ($3,352) + mileage cost ($23.91 per nautical mile × distance between the two hospitals). Base and mileage costs were for Rotor transport by the company Air Methods®.
Data Collection
Maternal and neonatal demographic information, which included race, gender, birth weight, gestational age, and inborn/out born status, was collected. Echocardiography indications and findings, as well as data related to hospital course, were obtained from existing EMR from CCMH and OUMC. Data from these records were recorded in a secure database on an encrypted network at OUHSC. Any collected paper documents related to the study were kept secure in a locked file cabinet within locked offices of the Neonatal-Perinatal Section, Department of Pediatrics.
Statistical Analysis
Descriptive statistics were computed for demographic and clinical variables. The agreement scores between tele-echocardiography and conventional echocardiography performed at either a Level IV NICU or in an outpatient setting are reported in full due to the small sample size.
Results
Over 5 years, telemedicine was used to screen 52 infants for CHD. Thirty-two infants (62%) had findings consistent with minor CHD or normal neonatal transitional physiology. Twenty infants (38%) had abnormal findings that required follow-up with either a conventional echocardiography as inpatient at the regional Level IV NICU or as outpatient after discharge. Fifteen out of the 20 patients with abnormal findings were scheduled for a follow-up echocardiogram in outpatient settings; 3 of those were lost to follow-up. Only 5 (10%) infants out of the total patient cohort required transfer to a Level IV NICU for the management of their CHD, whereas 47 (90%) infants were able to be managed at Level II NICU or could be discharged for outpatient follow-up (Fig. 1).
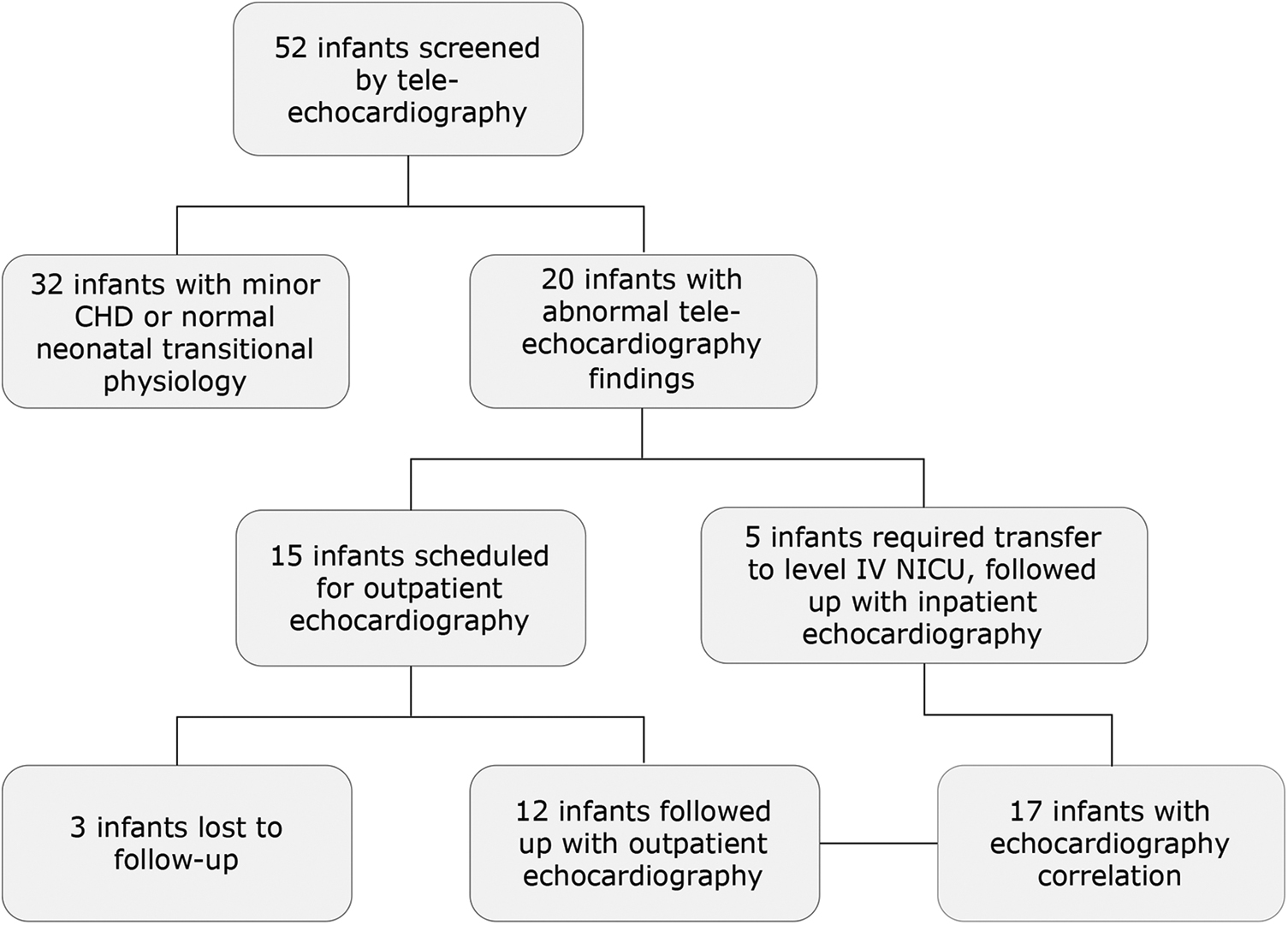
Study flow diagram.
Patient demographics are listed in Table 1. Indications for tele-echocardiography are listed in Table 2. Isolated murmur was noted to be the most frequent indication, followed by infant of diabetic mother with or without a murmur. Strong agreement was observed in majority of patients between echocardiogram findings obtained through telemedicine and those obtained by conventional echocardiography performed as either inpatient (Table 3) or outpatient settings (Table 4). Tele-echocardiography findings of patients lost to follow-up are listed in Table 5. No case of CCHD was missed.
Demographic Characteristics
Indications for Tele-Echocardiography
CCHD, critical cardiac heart disease.
Level of Agreement Between Tele-Echocardiography and Inpatient Conventional Echocardiography Findings
Agreement score of 1 = perfect agreement between occasions, or expected lesion resolution based on the expected clinical course; 2 = minor disagreement between the findings that did not affect management; 3 = different finding or new clinically important finding.
AS, aortic stenosis; COA, coarctation of aorta; HOCM, hypertrophic obstructive cardiomyopathy; LV, left ventricle; LVOTO, left ventricular outflow tract obstruction; PDA, patent ductus arteriosus; PFO, patent foramen ovale; PS, pulmonary stenosis; RA, right atrium; RV, right ventricle; TGV, transposition of the great vessels; VSD, ventricular septal defect.
Agreement Between Tele-Echocardiography and Outpatient Conventional Echocardiography Findings
Agreement score of 1 = perfect agreement between occasions, or expected lesion resolution based on the expected clinical course; 2 = minor disagreement between the findings that did not affect management; 3 = different finding or new clinically important finding.
ASD, atrial septal defect; HCM, hypertrophic cardiomyopathy; LVH, left ventricular hypertrophy; PPS, peripheral pulmonary stenosis.
Echocardiography Findings on Patients Lost to Follow-Up
DAA, ductal arteriosus aneurysm.
Finally, the estimated transport cost savings with the implementation of tele-echocardiography in the analyzed period of time was $260,000 (No. of patients enrolled in the study who were able to stay at the satellite Level II NICU [47] × transport cost per patient: base cost [$3,352] + mileage cost [$23.91 per nautical mile × 91 miles]).
Discussion
Our study demonstrates that the real-time echocardiography by telemedicine is extremely effective in providing prompt and accurate diagnosis of CHD. This approach becomes particularly attractive and feasible in medically underserved areas (MUAs), as an invaluable tool for remote and rural centers, which present unique challenges in delivering rapid access to specialty care. 32 –34
This study also highlights that this is a cost-effective way to provide expert pediatric cardiology care in MUAs. Without the use of tele-echocardiography, many of these babies would have undergone unnecessary transfer to a tertiary center for further evaluation, which would have significantly increased costs. 35,36
The most common indications for telemedicine echocardiogram in this study were heart murmur, followed by infants of diabetic mothers, and respiratory distress with or without an audible murmur, among others. In accordance with other published studies, possible CHD accounted for the most common indication for tele-echocardiography. 37 –39 The study found strong agreement between telemedicine echocardiography and conventional echocardiography in a majority of the neonates confirming prior studies' findings. 37 Only two patients out of the total patient cohort had minor findings (one with a small ventricular septal defect and another with trivial pulmonary stenosis) that were missed during tele-echocardiography. Both cases occurred early in the study and were likely due to lack of sonographer experience performing echocardiography in neonates. Although real-time tele-echocardiography provides training and proficiency opportunities for sonographers with limited formal instruction in pediatric echocardiography, getting additional training in neonatal echocardiography for sonographers in a Level II NICU would be ideal to bridge some of these gaps.
Most importantly, this study indicates that telemedicine is highly effective for CHD screening in a Level II NICU, as no cases of CCHD were missed. Furthermore, out of the total cohort, only 10% of babies were noted to have significant CHD needing transfer to a tertiary care center for further management, whereas the majority of the patients who had tele-echocardiograms had only minor or no heart disease and could either remain at the Level II NICU or be safely discharged home for outpatient follow-up. This finding is consistent with data from large studies in which the majority of the neonates could be effectively managed at a Level II NICU facility similar to ours. 35
There is also a significant benefit with respect to the psychological and emotional well-being of the family in caring for such babies in remote areas, as this prevents unnecessary anxiety and emotional distress from separation. 27 This approach allowed close family participation in the infant's care, since families were now closer to home. Provision of CHD screening through telemedicine in satellite NICUs supports this overall goal by preventing the unnecessary transfer to a tertiary referral hospital so that the infant can continue to receive level II NICU care closer to home.
To our knowledge, this is the first report of the use of tele-echocardiography to screen CHD in a level II NICU utilizing the hybrid form of telemedicine. 28 We were uniquely situated, as there were no upfront additional equipment costs since we were already using telemedicine in our NICU for other indications. In addition, we already had the advantage of and considerable experience in understanding some of the logistics and technical aspects of performing successful telemedicine studies. Our group has previously demonstrated that hybrid telemedicine is a safe and effective way to extend intensive care to late premature neonates in MUAs. This service had a great impact, as it showed the approach had significant benefits, such as reduction of costs associated with transport, limited duration of hospitalization, use of a higher level of care only when needed, and optimizing bed occupancy at a referral level IV NICU. 27
This study had some limitations. Although it was a retrospective study, the data were collected prospectively, and no subject was excluded for lack of data. The small sample size reflecting the relatively small size of the level II NICU could be another weakness. Some infants were lost to follow-up as outpatients, which limited our ability to assess accuracy by comparison with conventional echocardiography if needed. The reasons for lack of follow-up are not entirely clear, but could be due to expected resolution of minor lesions, thereby impacting the primary care physicians' referral or due to the family's perception about the need for follow-up in some minor lesions.
Conclusions
Tele-echocardiography can be safely and effectively utilized in advanced CHD screening, preventing the unnecessary transfer of the majority of infants to regional Level III/IV NICUs, resulting in major transport cost savings.
Ethics and Consent
This study was approved by the IRB of both institutions.
Footnotes
Acknowledgment
We thank Kathy Kyler for editorial support.
Disclosure Statement
No competing financial interests exist. The authors have indicated they have no financial relationships relevant to this article to disclose.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. No external funding for this article.