
Abstract
Background:
A 2012 systematic review by Oliver et al. of evidence-based research on telehospice included 26 research articles published between 2000 and 2010 on the use of telehospice connecting hospice professionals with caregivers and their care recipients. The present study replicated research by Oliver et al., extending the time frame from 2010 through 2020. The aim of this study was to answer the question—what is the current state of the evidence related to telehospice services?
Materials and Methods:
A systematic review was conducted for the time period 2010 to 2020 of the existing literature researching the topic of telehospice. Thirteen articles (five quantitative, six qualitative, and two mixed methods) were found that meet the inclusion criteria of the study. The Methodological Rigor Scoring Instrument was used to code the qualitative and quantitative articles separately to address methodological differences.
Results:
The most common findings were related to technology adaptation readiness for staff and caregivers. Studies assessed the use of telehospice that included incorporated technology, such as an electronic tablet, to provide synchronous communication between the provider and the patient/caregiver. Provider and caregiver attitudes regarding telehospice care were largely positive with studies reporting acceptance of telehospice as generally high.
Conclusions:
The past 10 years have yielded a small but significant body of research on telehospice. Published research on the topic reports a generally high level of patient and caregiver satisfaction about the experience, but limited findings have been published relating to patient outcomes. As adaptation of telehospice and technology has surged in the past year, it is expected that additional research on the impact of technology on clinical outcomes will emerge in the future.
Introduction
The worldwide pandemic of coronavirus (COVID-19) has accelerated the use of telehealth as a means to deliver health care in nearly every setting. Telehealth has been established as an effective means to manage chronic health conditions and provide episodic care for minor acute illness. Validation of telehealth assessment is important as clinicians attempt to make sound judgments in providing health care in the virtual realm. While telemedicine has been used for symptom management, especially during the pandemic crisis, research on the accuracy of virtual symptom assessment and management is in the beginning stages.
Advances in technology have become an accepted part of the health care environment. Telehealth can be defined as “the use of electronic information and telecommunications technologies to support long-distance health care, patient, and professional health-related education, public health, and health administration.” 1 Through the use of telehealth; patients, caregivers, families, and health care providers can be connected in a virtual environment. Telecommunication technology has been used in effective models for providing patient education virtually, as well as rendering clinical services for patients. 2
Telemedicine and e-health began in the 1960s with the use of unreliable broadcast and television systems, coupled with bulky equipment. Sixteen telemedicine projects (e.g., picturephone using switched network, broadband television, etc.) were identified in the United States in 1976. The National Aeronautics and Space Administration's remote monitoring of their crews served as a testbed for telemedicine technologies to improve the quality of health care delivery. 3
Two hospices in Michigan and Kansas began a telehospice project in 2000. 4 Doolittle et al. 5 continued the telehospice project in rural Kansas, using multidisciplinary team members providing for all aspects of supportive care, including psychosocial and bereavement care. IPads and secure videoconferencing used for remote staff meetings resulted in decreased travel and staff time, which increased confidence in using technology.
The Hospice Caregiving Research Network used technologies to support caregivers of patients at the end of life with the
With the rapid adoption of the internet and evolution of electronic devices, telehealth became an acceptable medium for providing health care to a larger audience. 8 Successful programs of telehealth for monitoring and communicating home care have expanded exponentially, especially for remote areas with little access to medical providers. Telehospice, a specialty form of telemedicine, bypasses barriers to quality end-of-life care by providing clinical and educational services through low-cost electronic devices (e.g., smart phones, tablets, laptop computers 9 ). Telehospice allows caregivers and individuals in home-based hospice care to communicate with hospice staff and family members, while meeting Health Insurance Portability and Accountability Act (HIPAA)-compliant requirements. According to the National Hospice and Palliative Care Organization, 10 55.7% of hospice patients in 2018 received care in their residence, making telehospice essential in the caregiving process.
According to the National Hospice and Palliative Care Organization, 10 $18.99 billion was spent on hospice care by Medicare in 2017. Nearly 50% of Medicare beneficiaries who died in 2017 were enrolled in hospice at the time of death, with 40% receiving care for 14 days or less. An additional 14% received care for more than 180 days. Routine level of home care accounts for 98.2% of days, providing evidence that the primary setting for hospice care is in the home. Supplies and services are delivered to the patient, which can incorporate a large geographic distribution for the patient population. The challenge of delivering timely hospice care to a wide geographic area has increased the interest in using telehospice.
A systematic review of evidence-based research on telehospice was conducted by Oliver et al. 11 Their review included 26 research articles that had been published between 2000 and 2010 on the use of telehospice connecting hospice professionals with caregivers and their care recipients. The present study replicates research by Oliver et al., 11 extending the time frame from 2010 through 2020.
Although both the technology and research for telehealth technology has grown dramatically over the last decade in home health care, less focus has been placed on the use of such technology in hospice care. Using virtual telehospice visits, caregivers have access to hospice staff 24/7, providing support when challenging situations regarding symptom management. This access can increase caregiver confidence and comfort with providing end-of-life care in the home. Research on telehospice has been conducted over the last 10 years and results will extend the understanding of research identified by Oliver et al. 11 The purpose of this study was to conduct a systematic review of the literature to discern available research and address the question, what is the current state of the evidence related to telehospice services?
Materials and Methods
A systematic review was conducted to assess the body of evidence that has been generated since the systematic review published by Oliver et al. 11 Databases (e.g., CINAHL, PubMed, and PsycINFO) were searched for studies published between January 1, 2010 and May 1, 2020. The review by Oliver et al. 11 was replicated using their initial search terms of “telehospice,” “telemedicine and hospice,” and “telehealth and hospice.” Search terms of “technology and hospice,” “videoconferencing and hospice,” and “electronic tablets and hospice” were added to attempt to capture additional relevant evidence and allow for titles that may not include the terms “telehealth” or “telemedicine” directly, but still were pertinent to the scope of the review. Inclusion criteria included being published in English, having been peer reviewed, and reporting empirical findings. Exclusion criteria were non-English language publications, articles that were not peer reviewed, and opinion articles. All articles were reviewed for relevance, with a total of 13 articles matching the search criteria. Data from included articles were organized into a table for evaluation. To minimize bias in scoring each article, initial data extraction and scoring was completed independently by the two authors. The author who was involved in one of the selected studies did not score her work. Scoring was conducted using the Methodological Rigor Scoring Instrument (MRSI) described by Oliver et al. (Table 1). 11 The MSRI provides coding for both qualitative and quantitative articles separately to address methodological differences. In addition, scores were obtained for the pertinence of the studies to the field. The complete scoring guide is available in the article by Oliver et al. 11 Based on this rating guide, articles could have high methodological ratings, but low significance to the field or vice versa. Being able to distinguish between methodological rigor and importance to the evidence base is considered to be necessary when a growing body of research is being disseminated. To ensure inter-rater reliability, each author scored the articles independently. They then met to discuss their scoring. Scoring consensus was obtained for both the methodological rigor and significance to the field for each article.
Qualitative and Quantitative Scoring Guide
Results
Although the process of the search and review of the current literature was replicated from the Oliver et al. 11 study, the resulting volume and quality of evidence were considerably less for the subsequent 10-year time span. The initial search strategy identified 31 relevant published articles. After the review of the abstracts and elimination of duplicates from the combined databases, a list of 18 articles was generated. Next, full articles from the list were reviewed with the inclusion criteria applied, resulting in the removal of five additional articles. A total of 13 articles met the inclusion criteria and comprised the unduplicated, peer reviewed empirically based telehospice studies published between January 1, 2010 and January 1, 2020. An additional two articles were found through manual search (Fig. 1).
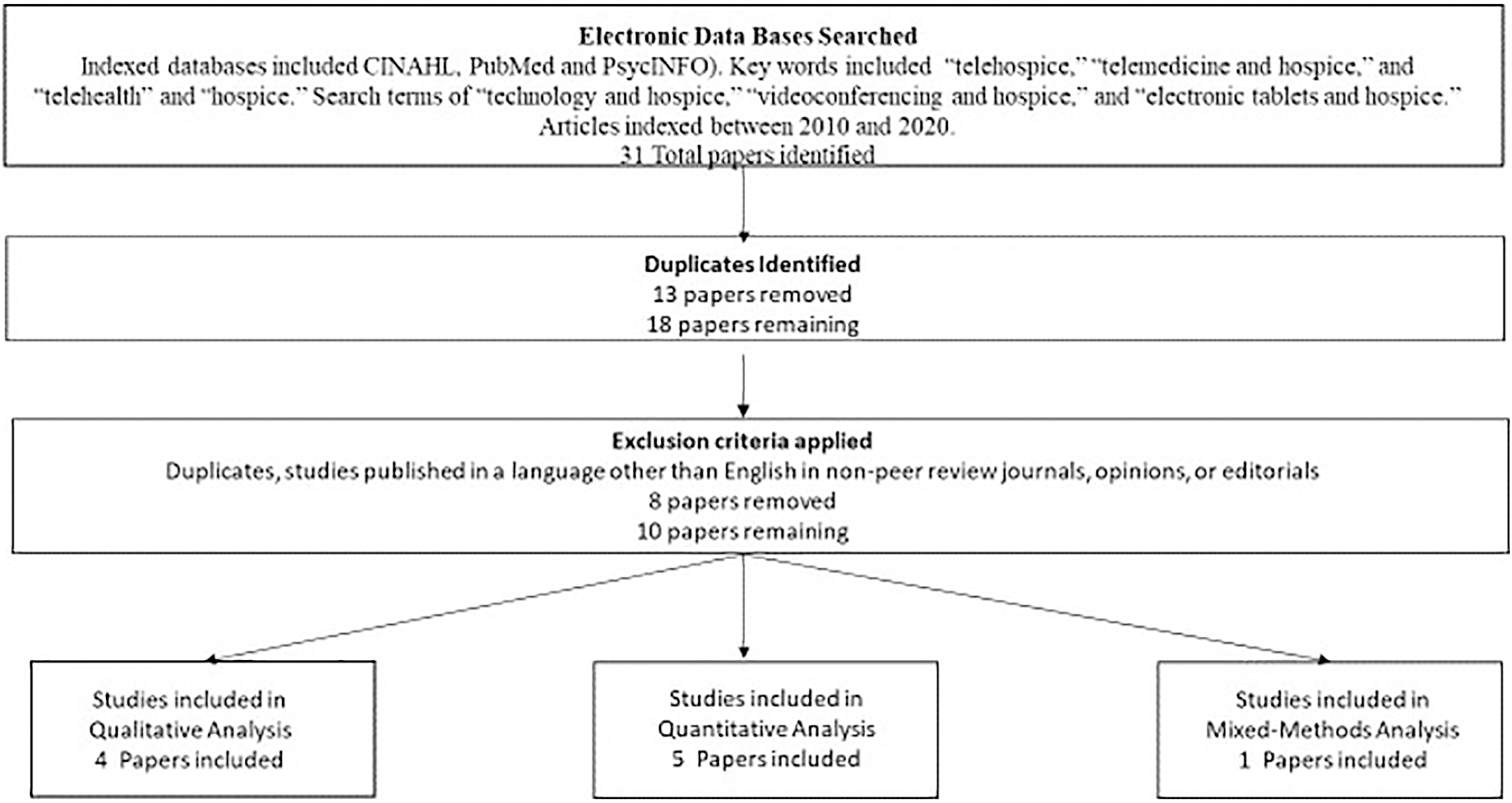
Process for systematically selecting articles (adapted from Oliver et al. 2012).
The findings of the individual studies were categorized into study design, sample size, setting, objectives, findings, and data sources. Six studies used qualitative methodologies, with five studies employing a quantitative research design. Two studies used a mixed methods design. Sample sizes ranged from 1 to 15 in the qualitative studies and from 50 to 917 participants in the quantitative research studies.
The most common findings were related to technology adaptation readiness for staff and caregivers. Studies assessed the use of telehospice that included incorporated technology, such as an electronic tablet, to provide synchronous communication between the provider and the patient/caregiver. Provider attitudes regarding telehospice care were largely positive, 5,12 with studies reporting staff acceptance of telehospice as generally high. The caregiver and patient attitudes were also largely positive. 12 –14 The patients and caregivers overwhelmingly reported that the technology was helpful to them in the caregiving role and provided comfort to themselves and patients. When education was provided through the telehospice intervention, participants reported satisfaction with the intervention. 14,15 Some studies reported that the caregiver did not use the telehospice unit but continued to endorse the use of telehospice.
Outcomes measured were patient perceptions of the role of telehospice in pain management, 16 acceptability of seeing hospice providers through telehealth for pediatric patients, 12 caregiver perceptions of education efficacy through telehealth, 15 identification of organizational facilitators of telehospice use, 17 impact of telehospice parenting program on parental self-efficacy, 14 quality of videoconferencing platforms for telehospice implementation, 18 ability of caregiver and nurse to identify facial expressions associated with emotion, 19 emotional comfort of caregivers using telehospice, 13 and feasibility of telehospice in a rural setting. 5 In assessing the relevance of the evidence, scores for the included studies were consistent with the Oliver et al. 11 review, with actual scores ranging from 3 to 15 for both quantitative and qualitative studies. The six quantitative methodological studies had a mean score of 12.1 (range of 7–15) representing low to medium strength of evidence. The studies were quasiexperimental or comparative designs. Lack of randomization and lack of a power calculation weakened most of the evidence as none of the studies reported completion of power analysis. The seven qualitative methodological studies were evaluated using the rigor scoring instrument as described by Oliver et al. 11 Scores ranged from 5 to 11 of a possible total score of 15, indicating low to medium strength of evidence. In reviewing the individual components of the quality scoring, the weakest components involved the sampling and participant description within the studies. This weakness may have been a necessary limitation, as several studies had small sample sizes, necessitating some lack of detail to protect participant anonymity. Additionally, a number of articles were focused largely on technologic capacities of organizations, experiences in using technology, or organizational characteristics that limited the applicability of some instrument items in evaluating these studies. The two mixed methods studies were scored in both the qualitative and quantitative tools (Table 2).
Scoring of Studies in Telehospice
Baldwin et al. 17 identified the subthemes that are outlined in the Conceptual Framework for Ambulatory Care Nurses Scope and Standards of Practice for professional telehealth nursing 20 are the patient, nurse, and the environment. In hospice care, “patient” is the holistic unit of the patient themselves as well as the caregiver and family that participate in the care. The “nurse” is included in an interdisciplinary team, which is inclusive of health professionals. Both technology and health care systems are components of the “environment,” which allows the connection between nurse and patient (Table 3).
Data Evaluation Findings
CMP, condition management protocol; PEACE, Palliative/End-of-Life/Assessment/Care Coordination/Evidence; TACP, technology-assisted care pathways.
Caregiver/Patient
The Lewis et al. 14 study showed significant improvements in caregivers' skills and self-efficacy in supporting their children coping with their parents' cancer. They also found improvements with historical controls on parents' anxiety, depressed mood, self-efficacy, parenting skills, and children's behavioral/emotional adjustment. Cameron and Gugala 13 surveyed 667 hospice caregivers, with results of their retrospective mixed methods study providing support for the efficacy of using telehospice with caregivers of home-bound patients. Most respondents reported being comfortable using telehospice with caregiving. The results indicated that as comfort levels with telehospice increased, caregivers were more willing to use virtual health care again. Allsop et al. 16 found that patients perceived that telehospice could be a component of managing their pain during hospice services. Caring for a person at the end of life can be stressful and having the ability to contact a professional at any time of the day or night provides comfort to the caregiver and their family. Weaver et al. 12 noted that the time between discharge from hospital to home-based palliative care is vulnerable. This change could be addressed with the virtual transitions model that provides cost-effective continuity of care. For families in rural settings, the telehealth modality decreased travel and time, while maintaining the link with hospice professionals.
Health Professionals
The use of technology to link health professionals with patients and family caregivers has been recognized as a potential solution to access to hospice care and has evolved as an essential tool during the COVID pandemic. This pandemic necessitated the rapid integration of screen modalities into palliative care, which warranted consideration of barriers and challenges of telehealth. Prior studies revealed reasons for care providers' concerns about telehealth that include lack of training, lack of incentive, lack of equipment availability, lack of perceived easiness of equipment use, and uncertainty of patient eligibility for telehealth. The established requirements for successful telehealth include provider training; user friendly, reliable, accessible, secure technology; and clear connectivity. The greatest concern of health care providers is the impact of virtual interactions on communication is the fear of decay in the quality of health care. 12
Weaver et al. 12 used qualitative methods with a group of hospice nurses and uncovered a concern with telemedicine use in palliative care and hospice. They identified the concern as whether the communication modality could be a facilitator or a barrier. Participants, including nurses, pediatric patients, and family caregivers, expressed fears about virtual interaction that could have a potential for depersonalized team and family experiences, especially with sensitive topics. Nurses shared concerns about telehealth and its impact on professional roles and autonomy, and quality of care. They also voiced concerns about not being present to assist a patient in situations that could require hands on care, such as an adverse medication reaction. This finding was significant as many studies examined acceptance of the interventions by patients, but the Weaver et al. 12 study examined nurse acceptability.
Technology
Technical difficulties as a barrier to implementation and acceptance were recurrent findings. 2,6,16,17 Researchers used a variety of technological components and videoconferencing platforms to accomplish their interventions. None of the studies allowed for participants to use their own personal mobile devices. With the rapid evolution of technology, and increased accessibility of telemedicine through personal smart devices, such as phones and tablets, additional future work that incorporates these consumer technologies would be warranted to truly assess feasibility and impact on patient outcomes.
Patient/caregiver acceptance of technology was discussed in several publications. 12,13,15,16 Generally, participants were accepting the use of technology for the provision of care, although there was discussion of the need to adapt the interaction and technology to enhance the participant–staff interaction. This may be somewhat improved if studies were reproduced using present technology. The adoption of software that offers greater video clarity, such as Zoom and Facetime, has increased the need for HIPAA-compliant software that supports communication. Demiris et al. 18 found Web-based videoconferencing to be superior to video phones. The Schmidt et al. 19 study explored the ability to caregivers and nurses to identify facial expressions associated with emotion using video platforms. Given the significant advancement that has occurred in video streaming over the past years, their positive findings are likely even more relevant in today's clinical setting. The next 10 years may also show newer and more efficient software and hardware that supports virtual visits and communication between health care providers and caregivers, patients, and families.
Health Systems
Several positive aspects associated with telehospice need to be recognized for the health care systems. Ingram et al. 21 identified digital health technologies as a valuable tool in end-of-life care in community settings, especially with the role-of-care coordination. Two health care systems, Mayo Clinic and Medtronic, developed technology-assisted hospice and palliative care coordination. 21 Combining medical and engineering institutions, a technology-assisted patient care platform was created to connect patients and caregivers to high-quality, evidence-based clinical care. They suggested that patients given this option for care had a longer median length of hospice care than the national average, fewer hospital days, and high levels of patient and caregiver satisfaction. In addition, proactive continuous symptom management for nausea, dyspnea, and pain were reported. Health systems can integrate telehospice into existing community programs as a supplemental, cost-effective treatment option.
Palliative and hospice systems that serve patients and caregivers in rural and underserved areas should consider implementing telehealth programs to increase quality of life, communication, relationship, and decrease symptom burden. 12 She cautioned that this type of program should be adjuvant, with face-to-face palliative care remaining primary. Palliative and hospice systems need to acknowledge that nurses often consider telehealth as an impersonal modality that minimizes the actual value to human touch. 12
Cameron and Gugala 13 discussed the importance of organization support in facilitating internet connectivity and response time of health care providers to caregivers and their care recipients. Maintaining a caring relationship between hospice providers and caregivers when using virtual connections is important for telehospice acceptance. Further exploration of facilitators and barriers to telehospice use would be beneficial to understand the potential of telehospice to improve access to care and prepare for telehospice implementation.
One article focused specifically on the organizational features associated with telehospice implementation. 17 Using logistic regression analysis, the authors asserted that organizations with established directors and a master's degree were more likely to use telehospice to deliver care. A negative association was found between having a director whose background was in nursing and telehospice use.
Health care systems need to consider telehealth to connect health care providers, patients, and caregivers to enhance communications and improve quality of life. Telehealth can promote timely symptom management that could avoid delays in care management due to travel and now with the COVID pandemic. Telehealth is on the cusp of a new horizon in health care that can increase connections with vulnerable populations who present challenges for meeting face to face.
Discussion
Systematic reviews can be defined as a type of research synthesis that is conducted to identify and retrieve evidence that is relevant to a particular question or questions. In addition, these reviews appraised and synthesized results of this search to inform practice, policy, and in some cases, identify a need for further research. 22 Systematic reviews involve a detailed and comprehensive plan along with a search strategy developed a priori. A goal is to reduce bias by identifying, appraising, and synthesizing all relevant studies on a particular topic. Often, systematic reviews include a meta-analysis component that involves using statistical techniques to combine data from several studies into a single quantitative estimate or summary effect size. 23
The gold standard for research is usually randomized controlled trials. However, in examining the available research on this topic, many diverse methodologies, including qualitative, quantitative, and mixed methods studies, were used to explore the evidence. A quality improvement study was included to describe the process of using telehospice as a vehicle for continuous symptom control. The generated evidence could inform future research in this developing field.
The identification of 13 empirical studies in the 10-year span provided evidence that limited research had been published on this topic. Although the use of technology in health care has grown exponentially, research on outcomes of this adaptation has been limited. One large gap in the literature is patient outcome evidence. Instead, emphasis was placed on patient acceptance and satisfaction with the intervention. An increased focus on building evidence for the utility of telehospice is imperative. The Hospice and Palliative Nursing Association
24
has set research priorities for the years 2019–2022 which include: Conduct studies using implementation science principles and frameworks to facilitate the successful adoption and integration of evidence-based hospice and palliative nursing into routine care. Provide appropriate measures to capture the penetration, effectiveness, and sustainability of palliative care programs. (p. 3) Assess the use and effectiveness of various implementation strategies (i.e., methods to enhance the adoption, implementation, and sustainability of a clinical program or practice) to successfully integrate palliative care services in routine practice. (p. 3) Explore the caregiver's perspective of technology to identify the uptake, use, and acceptability of technology to support caregivers. (p. 2)
Although these research priorities do not mention telehospice specifically, a research priority using technology could be included to strengthen evidence regarding adoption and integration of evidence-based virtual hospice and palliative care. Barriers to adoption of telehospice include nursing staff readiness and perceptions, connectivity, and technical quality challenges, as well as gatekeeping by the hospice staff, and limiting access to patients and caregivers for research.
Facilitators of technology adoption include financial incentives for telehospice and strong support for this method of communication from patients and caregivers. Doolittle et al. 5 found that staff's positive attitude and feelings of organizational support was a positive predictor of telehealth success. The hospice staff reported that telehospice saved travel time and enhanced their job satisfaction. A benefit to the family was that bereavement services were readily available through an iPad.
Next Steps
Additional work could result in clinical pathways that are specific to the provision of hospice care through telemedicine. Because patient assessments can be impaired by limitations of the technology, additional research regarding the fidelity of symptom assessments would be helpful in establishing telehospice interventions as true equivalents of face-to-face care. The body of literature has not established criteria for determining triage pathways where telehospice is appropriate or when face-to-face interventions are required. Considering the potential for technical interruptions when conducting assessments using telehospice, alternative plans should be in place to provide quality of care for hospice patients. Clinical processes that incorporate telemedicine should have alternative plans in the case of technology failure, which is of particular importance with vulnerable populations, such as patients receiving hospice care.
Ethical considerations should incorporate the mandates of HIPAA to ensure that patients and their caregivers are protected from potential breaches of confidentiality. Selecting software that is HIPAA compliant when using telehealth with hospice patients. Clinical outcomes associated with telehospice use that need to be researched include symptom management with time frames for interventions, length of stay on hospice service, use of inpatient and respite services, and caregiver efficacy with the role. This research can provide a basis for expansion of telehealth to other medical fields, especially when providing patient care in places and times with limited access to health care.
In examining studies with lower scores, the authors acknowledged limitations in the application of the scoring tool. Studies that were focused on the technological aspects of the telehospice intervention were challenging to score using the tool. Adaptation may be necessary for future work to better incorporate works from across disciplines and emphasizing exploration of technology.
Conclusions
The past 10 years have yielded a small but substantial body of research on telehospice. Published research on the topic reports a generally high level of patient and caregiver satisfaction about the experience, but limited findings have been published relating to patient outcomes. As adaptation of telehospice and technology has surged in the past year, it is expected that additional research on the impact of technology on clinical outcomes will emerge in the future.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank the researchers who have completed works to bring forward the evidence on telehospice. They would like to thank June Cline for her editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.