
Abstract
Background:
Health care is provided in developing countries, in a milieu of acute shortages of health care infrastructure and personnel. Governments are realizing that digital health through public private partnerships (PPPs) could address this issue. Literature review did not reveal reports on primary use of telemedicine or
Materials and Methods:
The authors report using digital health in a mega PPP project in nine districts in Andhra Pradesh, a state in South India, where millions are benefiting from TeRH. Strategies deployed to address operational, technical, and clinical challenges in virtually reaching the unreached deploying technology are described. A detailed analysis was made of services provided in 183 Urban Primary Health Centres (UPHCs) over 47 months.
Results
: 2,648,322 unique patients had quality digital health care. Of 11,055,936 consultations, 1,013,996 were specialist teleconsultations, including cardiology, endocrinology, general medicine, orthopedics and OB/Gynecology. 7,408,283 laboratory tests were done. Costs for laboratory tests was 28.84% of that in private laboratories. Cost per specialist teleconsultation was  165 (Rupees). Quality control of laboratories was ensured through remote monitoring.
165 (Rupees). Quality control of laboratories was ensured through remote monitoring.
Discussion:
Implementing digital health in PPP projects requires expertise across clinical, technology, contract management, financing, data standards, information security, project planning, and cost-effective implementation.
Conclusions:
This successful mega project has confirmed that given a dedicated cooperative team e-health in a PPP mode in a developing country is eminently doable. Digital health care records were introduced and maintained for 100% of the beneficiaries (2.6 million in this study). TeRH can now bridge the health care divide.
Introduction
Public private partnership (PPP) projects in health care are a recent phenomenon in India. Figure 1 illustrates the various PPP projects outsourced to Apollo Telehealth Services (
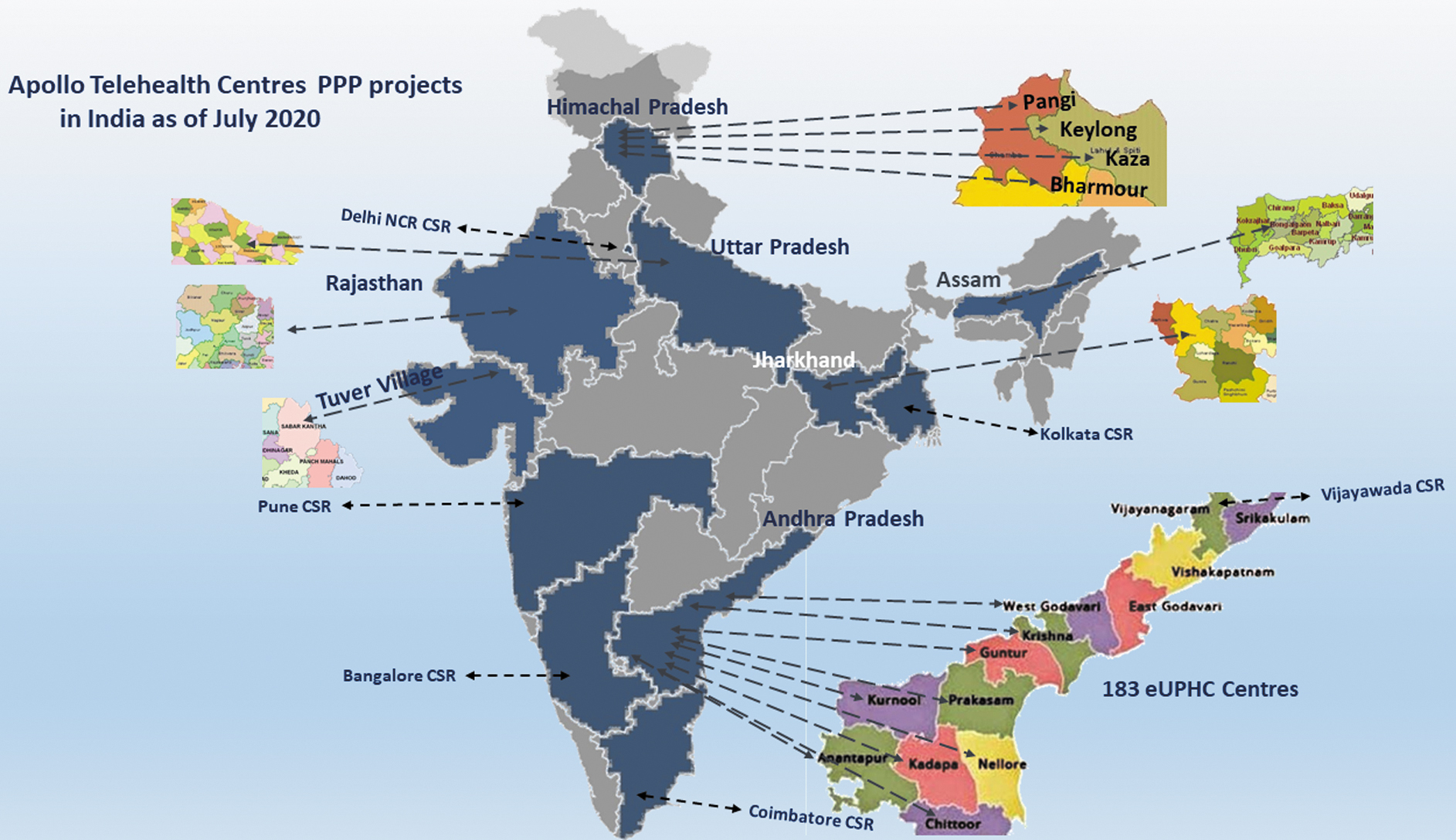
Apollo Telehealth Centres PPP Projects in India. PPP, public private partnership.
Basic and advanced health care needs of 20% of the state's population of 66 million was covered. The entire process was digitized. All digital services were free to the beneficiaries. Continuum of care was ensured. Technology ensured health care delivery, diagnosis, treatment, monitoring, and promotion of preventive remote health services. In this program, selected UPHCs were upgraded to electronic (digital) UPHCs. Telehealth services were added. This ensured essential primary and specialist health care for the urban poor, living in slums.
Each UPHC had six employees, including one MBBS doctor, two auxiliary nurse midwives (ANM), one laboratory technician, one desktop support engineer, and one general assistant all available from 9.00 am to 5.00 pm 365 days a year. Additional outreach services included yoga and nutritional sessions deploying staff nurses. eAushudhi an ePharmacy Government of Andhra Pradesh software for supply and stock management of 158 different medicines was deployed.
Telemonitoring of Laboratories Ensuring Quality Control
Figure 2 depicts functioning of technology-enabled laboratories. Each of 183 UPHCs has laboratories conducting 41 tests across hematology, biochemistry, pathology, microbiology/serology. Each laboratory was equipped with a semiautomatic analyzer for biochemistry, a cell counter for clinical pathology along with rapid diagnostic kits, and a microscope.

Laboratory investigation process.
All laboratories are remotely monitored. Laboratory inventory control and management, quality of laboratory technician's expertise is authenticated by ensuring protocol adherence. Results are provided within 4 h.
Telemonitoring of all laboratory processes is continually done by a remote expert team. A remote quality assurance system tracks health of devices, reagents, and consumables. All UPHC laboratories are ISO 9001:2015 standardized. In addition to Internal Quality Control, an External Quality Assessment System is implemented. Laboratory Information Management System is an updated software with well-defined verticals, maintaining workflow with data tracking, downloading support and data exchange interfaces. Over 47 months, the mean tests done per patient was 4.1 (varying from 3.7 to 4.8). Patient electronic medical record (EMR) with updated test results is accessible to the consultant. Dedicated modules were made for patient data capture, quality control, and inventory management. During the study period, 7,408,283 laboratory tests were completed with an uptime of 99.3%.
Operational Details
A grievance redressal process, with a toll-free number was available in all UPHCs to resolve issues. To improve patient experience, cold, filtered drinking water in an ultrahygienic air-conditioned environment was provided (nonexistent in government UPHCs). Patient satisfaction was monitored. Field operations and monitoring was carried out by managers supervised by a chief medical officer. All operations were standardized in a paperless environment. Biometrics was used. As all services are under the umbrella of the National Health Mission (NHM), Reproductive, Maternal, Neonatal, Child and Adolescents Health, immunization, anemia, nutrition counseling services were also provided.
COVID-19 and Implementation of Digital Health Care in UPHC
UPHC staff participated as a frontline surveillance team in COVID-19 screening. Infected patients were identified, isolated, and provided optimized care. During the process, some of the staff got infected.
Materials and Methods
Telemedicine Services
The on-site family physician in each center had access to cardiology, orthopedic/rheumatology, general medicine, and endocrinology specialists. From February 29, 2020 Ob/Gyn teleconsultations were also available. All services are remotely monitored, using real-time application data capture into patient EMR's and a centralized dashboard. The processes involved in fixing an appointment for teleconsultation is given in Figure 3.
Teleconsultation appointment process.
Figure 4 shows teleconsultation in progress with a specialist facilitated by a paramedic. Figure 5 shows patients collecting free medicines from the digitized pharmacy and Figure 6 shows entries being made in EMR by a paramedic.

Patient having teleconsult in presence of paramedic.

Collecting medicines at on-site pharmacy.

Entries in EMR made by paramedic. EMR, electronic medical record.
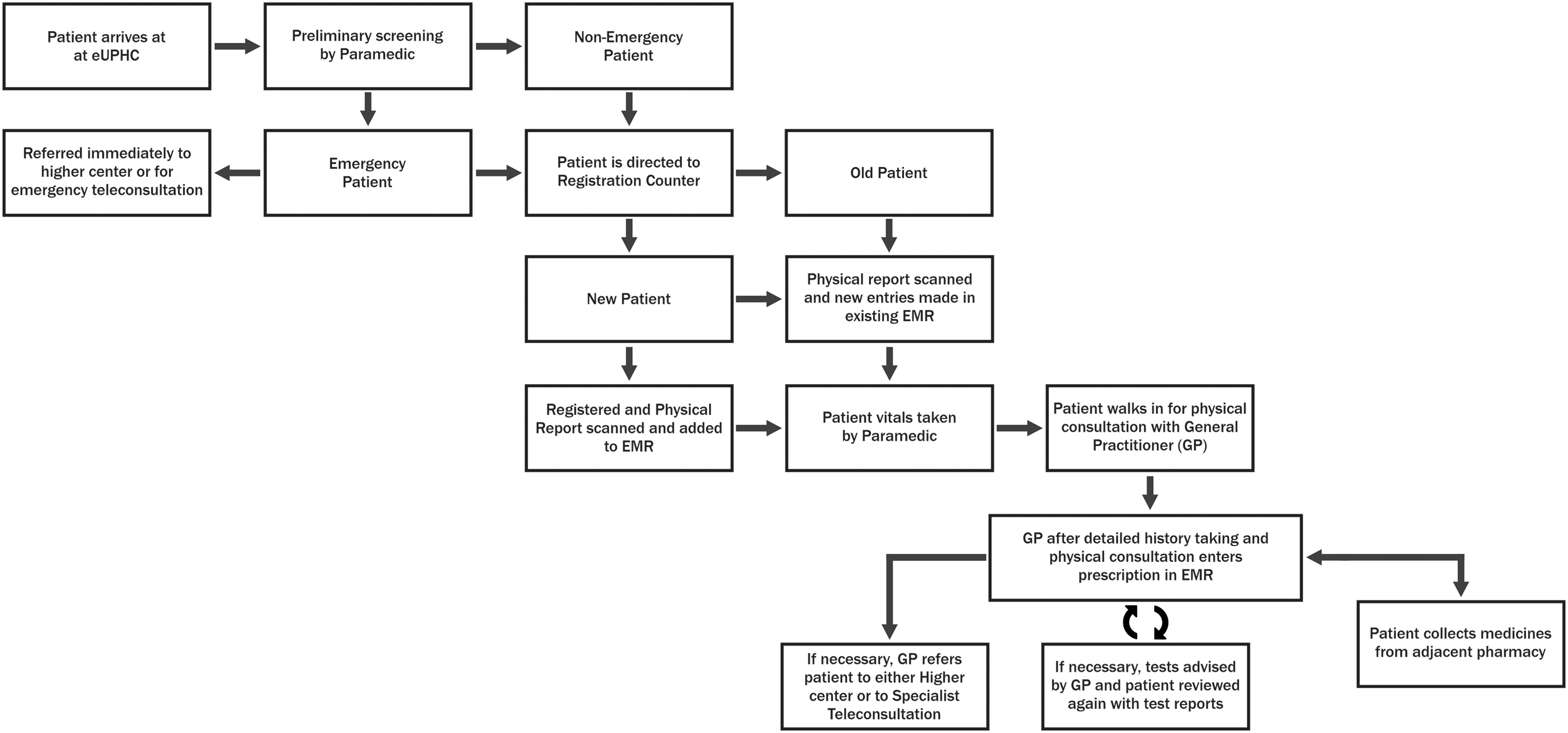
The model practiced is hybrid care at a scale that has not been done before, where patients are being seen both in-person and, depending on necessity and circumstances online by specialists. All patients are generally seen by an in-person GP who triages them to teleconsults and other options if necessary. This happens at all the 183 remote sites.
Digital Medical Records and Quality Assurance
All transactions are paperless. A comprehensive software tracks patient's health profile. Embedded standardized data options ensure negligible data entry errors. Data are stored in highly secured database cloud servers. Compliance with National Health Mission (Government of India) directives is ensured through reporting formats. Quality Assurance Protocols address technical and clinical aspects of all services ensuring quality and optimal resource utilization, resulting in a credible, sustainable, intrinsic Quality Management System (QMS). A dedicated audit team evaluates the QMS. Continuous classroom, virtual training, retraining, to ensure appropriate knowledge, skills, and behavior is carried out. Pre- and postassessments confirm training effectiveness. All UPHCs are ISO 9001:2015 standardized.
Community Linkage
Accredited Social Health Activist (ASHA) and ANM's were links between community and UPHC. They ensured referrals, follow-ups, counseling, survey, and distribution of vitamins and family planning products. They tracked and followed up antenatal and postnatal mothers, newborn babies, and patients with communicable diseases. Suspected cases (including COVID-19) were referred to UPHCs. Responsibilities include promoting immunization and health education. Table 1 compares digital health care services presently offered to what was available earlier. IRB approval Ref AIMSR/IRB/RC/2020/10/001 was obtained for the study.
Comparison of Pre-Existing Manual with Present Digital Services in Urban Primary Health Centres
ANC, antenatal care; ASHA, Accredited Social Health Activist; eUPHC, electronic Urban Primary Health Center; KPI, key performance indicators; PHC, Primary Health Center; UPHC, Urban Primary Health Centre.
Results
From November 2016 to July 31, 2020 a total of 11,055,936 consultations were provided to 2,648,322 unique patients. Of the 1,013,996 teleconsultations 57,922 was for cardiology, 308,251 for endocrinology (predominantly diabetes) 419,815 was for general medicine, 226,300 for orthopedics, and 1,708 gynecology (teleconsults started on February 29, 2020). 155,080 unique patients with hypertension and 189,717 with diabetes had 2,821,726 and 3,195,553 consultations (direct and remote consults). Communicable diseases identified included dengue (2,588), malaria (2,235), tuberculosis (3,861), and leprosy (114). 250,980 women were registered for antenatal checkup. Of these, 61,106 were found to be anemic, 799 had hypertension, and 1,456 diabetes. 567,383 children were registered for immunization. 3,186,885 doses were given cumulatively. Steady increase in utilization of digital health care services is shown in Figure 7. Despite total lockdown enforced from March 25, 2020 to June 8 and August 5, 2020 (unlocked in phases), eUPHC services were provided and utilized.

Total male and female consultations at UPHC. UPHC, Urban Primary Health Centre.
Cost-Effectiveness of Digital Health Care
Prinja et al.
2
in a study of 14 Primary Health Center (PHCs) and Community Health Center (CHCs) in North India in 2013 demonstrated that  8.8 million (Rupees) was the annual cost for 7 PHCs with a per capita annual cost of
8.8 million (Rupees) was the annual cost for 7 PHCs with a per capita annual cost of  170.8 for preventive, curative, and promotive services. Human resources (HR) then accounted for >50% of overall costs. In this study, operational cost included salaries, HR, consumables, travel, administrative charges, and printing. 728.20 million rupees would have been spent by the underprivileged community on laboratory tests alone at a mean cost of
170.8 for preventive, curative, and promotive services. Human resources (HR) then accounted for >50% of overall costs. In this study, operational cost included salaries, HR, consumables, travel, administrative charges, and printing. 728.20 million rupees would have been spent by the underprivileged community on laboratory tests alone at a mean cost of  3,807 instead of
3,807 instead of  584.84 million actually incurred at UPHCs at a mean cost of
584.84 million actually incurred at UPHCs at a mean cost of  946. In comparison with UPHC only 31% tests are available in other PHCs. Figure 8 and Table 2 depict cost of delivering digital health services. This robust review clearly proves that enabling digital health eventually results in considerable cost savings. The impact becomes more as capital expenditure is one time. This study has revealed that per capita costs progressively decreases over the years. Impact is considerable. Costs for laboratory tests was 28.84% of that in private laboratories. Cost per specialist teleconsultation was
946. In comparison with UPHC only 31% tests are available in other PHCs. Figure 8 and Table 2 depict cost of delivering digital health services. This robust review clearly proves that enabling digital health eventually results in considerable cost savings. The impact becomes more as capital expenditure is one time. This study has revealed that per capita costs progressively decreases over the years. Impact is considerable. Costs for laboratory tests was 28.84% of that in private laboratories. Cost per specialist teleconsultation was  165.
165.

Cost of delivering digital health services.
Unit Costs of Delivering Digital Health Care Services @ Urban Primary Health Centre
Unique patient cost includes immunization, pharmacy, laboratory, physician, and specialist teleconsultation, maternal and child health, and initial management of communicable and noncommunicable diseases. OPD, Out Patient Department.
Discussion
Universal health care delivery poses a significant challenge. Digitization of services in a PPP mode addresses most issues. Cloud-based EHR systems in a e-PPP model reduces paperwork and improves efficiency. 3 Brazil, Canada, and China have adopted PPP in health care. 4,5 Establishment and management of robust telemedicine and digital health PPP programs presuppose a focus on overall digital health framework. This includes financing, affordability, data standards, information security, project planning, implementation, evaluation, and establishing a transparent procurement process. 6 Most primary and secondary health care services are provided in government sector and high-tech tertiary care by the private sector. A properly implemented PPP can provide rational, affordable, and comprehensive care. India has a history of PPPs in health, partnering with nonprofit and for-profit organizations. 7 This is leading to improvement in health care using digital technology, good infrastructure, and medical expertise. McKinsey has opined that PPP could improve health care delivery in India by 2022. 8 Through this model, health care delivery could be standardized while maintaining a high quality of service. 9 Technology-enabled remote health care is a recent phenomenon. 10 Publications suggest that telemedicine is set to grow in India over the next 5 years 11 and e-health will help reaching the unreached. 12 India is well positioned to give exemplary digital health solutions through PPPs. 13 –15 The world's largest health care program Ayushman Bharat is one such example. 16 Medical opinions, consultation, diagnosis, and surveillance are possible in a cost-effective and efficient manner through an all India telemedicine network. 17 Private players with expertise and managerial experience in deploying health care Information and Communication Technology networks increase access to quality health care. 18 Teleconsultations have been provided at camps for screening noncommunicable diseases. 19 Operational challenges, including setting up of Tele-Emergency Services in remote areas in the Himalayas in a PPP mode, have been reported. 20,21 Innovations include using solar power for providing digital health services in remote areas. 22 Barriers to adoption of telemedicine include technology integration, interoperability, standardization, security, time constraints, and financing. Governments can provide technology but proactive health professionals are needed to use equipments. Hurdles relate to reimbursement, policies governing telecommunication and information technologies, development, and licensure. Telehealth adoption is a complex behavior determined by a large set of psychosocial factors and issues related to health care organizations. 23
Program implementation for eUPHCs started with planning optimum HR and proper training. Improving stakeholder participation, increasing problem assessment capacities, and developing local leadership to promote community programs was critical. After a need assessment study, an end-to-end turnkey solution, on a program management approach with measurable milestones and monthly reports was initiated. A devoted passionate team of telemedicine specialists, clinicians, and program managers using HR from the local community identified and circumvented hosts of issues. This resulted in standard operating procedures (SoPs), service level agreements, fixing accountability, and responsibility. Measurable goals were defined. Regular auditing, deploying objective impact assessment tools, performance indicators, grievance redressal mechanisms, and escalation and evaluation matrices were used. Creating a motivated team to administer and implement well thought-out SoPs, with good “Man Management” helped fulfill primary objectives of delivering remote health care.
Virtual OPs were scheduled at predetermined times and days, depending on local convenience. Specialist Telecamps would ensure maximum utilization of the specialist's limited time. Figure 9 shows the medical call center at Apollo Hospitals, Hyderabad, to which each center was remotely connected for specialist teleconsultations. By leveraging communication technology, this first of a kind PPP initiative, extended outreach of a quaternary care hospital, bringing specialized care to the underprivileged. Technology enabled Remote Health Care reduced load at government tertiary hospitals and out-of-pocket expenditure for the public.

Digital Health Care Call Centre, Apollo Hospitals, Hyderabad.
Scope of the partnership was extremely focused due to the low-resource budget-constrained setting, making follow-up and a detailed impact analysis challenging.
Conclusions
PPPs in health care are an important element of the World Bank Group's response to country health challenges. From 2004 to 2015, the Bank Group had approved 78 such projects. Inevitable transition to smart technologies will have a significant impact on health care processes and governance. Robust telemedicine and digital health PPP programs presuppose a focus on overall digital health framework. This communication has addressed teething problems of implementing digital health divide and demonstrated that delivering digital health care in an emerging economy is doable. This experience can now be extrapolated to other regions in India and other countries as well.
Footnotes
Authors' Contributions
Dr. Krishnan Ganapathy conceptualized the article. He was the principal coordinator with rest of the team tying all loose ends, primarily responsible for writing the entire article, highlighting the unique features, and reviewing the literature and ensuring that the final product fulfilled specific requirements of the journal. Mr. Santos Das was single point of contact to ensure that all formalities were complied with; proposal design and development; collected data and carried data analysis and interpretation, modifying and reviewing as requested by the principal author. He contributed in development of tables, graphs, and made available photos as requested; critical review and feedback. Dr. Sangita Reddy was in charge of conceptualization; leadership in actual execution of the whole project since inception of the services; provided total administrative support required and reviewed the article. Mr. Vikram Thaploo supervised collection of data and oversaw operational details of the entire project, provided necessary administrative support, and reviewed the article. Dr. Ayesha Nazneen supervised the entire delivery of digital health care from a clinician's perspective, contributed in obtaining data and data interpretation, and reviewed the article. Dr. Akhila Kosuru contributed in data analysis, discussed the results and contributed in compiling the raw data and integrating all loose ends, and reviewed the article. Mr. Uday Shankar Nag was primarily responsible for obtaining raw data at the field level, helped in coordination and sorting out various administrative issues as this is a PPP project with government.
Acknowledgments
The authors thank Mr. Bhaskar, MD, National Health Commission (NHM) and Commissioner, H&FW, and Mr. K. Apparao, State Program Manager, NHM of the Government of Andhra Pradesh, for permission to use information from the UPHCs. The authors also thank Mr. Sourov Banerjee, Mr. Ganesh Petkar, Mr. Viplav Kirthi, Dr. Meghnath Reddy, and N. Satish Kumar of ATHS for their support in collecting data, and Ms. Lakshmi for secretarial assistance.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding received for this article.