
Abstract
Background:
This study aims to describe one center's experience in expanding a fetal telecardiology program through collaborative work with maternal fetal medicine (MFM) clinics with the goal of safely reaching mothers during the COVID-19 pandemic. We sought to define the extent of fetal telehealth conversion at a large fetal cardiac care center and evaluate the diagnostic accuracy for studies performed.
Methods:
At our center, fetal telemedicine expanded from one MFM site before the pandemic to four additional sites by May 2020. A retrospective review of fetal telecardiology visits between March 15 and July 15, 2020, was performed. The chart was reviewed for confirmation of diagnosis postnatally.
Results:
With pandemic onset, there was a large increase in the number of telemedicine visits with a total of 122 mothers seen between five MFM clinics. Fourteen mothers (11.5%) had abnormal fetal echocardiograms requiring additional follow-up, and seven mothers (5.8%) had a fetal echocardiogram suspicious for a critical congenital heart disease (CCHD). All the fetal echocardiograms suspicious for CCHD were confirmed on postnatal echocardiogram. To our knowledge, none of the normal fetal echocardiograms were found to have congenital heart disease postnatally.
Conclusions:
In response to the COVID-19 pandemic, we rapidly transitioned to fetal telecardiology using a variety of formats. This has reduced potential infectious exposure for pregnant mothers and minimized contact between physicians without compromising diagnostic accuracy. In our experience, the expansion of a telemedicine program requires strong initial infrastructure, prior relationships with MFM providers, and appropriate training among obstetric sonographers.
Introduction
In early March 2020, the novel coronavirus disease (COVID-19) was characterized a pandemic, and by the end of March, social distancing measures were enacted in many states across the United States and the District of Columbia (DC). For obstetric patients, each in-person prenatal care visit raises concerns for potential exposure to COVID-19. Telehealth has been cited as an approach to mitigate risk while continuing to provide prenatal care to obstetric patients, many of whom have underlying medical or fetal conditions putting them at increased risk for complications if they contracted COVID-19. 1
At our center before the COVID-19 pandemic, mothers with a referred indication for fetal echocardiogram were typically evaluated at a tertiary-care children's hospital for care with a pediatric cardiologist. In some practices, fetal echocardiograms were performed at a maternal fetal medicine (MFM) office with a pediatric cardiologist present.
With the spread of COVID-19 and increased social distancing measures in place, pregnant women face additional barriers to expert fetal cardiac evaluation. Given the significant close contact between the mother, the sonographer, and the pediatric cardiologist during normal visits and widespread shortages of personal protective equipment, many centers enacted a triage process during the pandemic. 2,3 Owing to extenuating circumstances of the pandemic, Children's National Hospital Cardiology department rapidly expanded upon its developing fetal telecardiology program to better serve the growing need for telehealth consultations. With challenging fetal cases before the pandemic, the pediatric cardiologist would obtain images in the MFM office in conjunction with the obstetric sonographer. However, during the expansion of telemedicine, the obstetric sonographers obtained these images independently.
A few prior studies have shown that telecardiology can be a feasible option to successfully risk-stratify fetal heart defects. In two medically underserved areas, mothers preferred having a local fetal cardiac evaluation over having to travel. 4,5 Prior studies have also reported using remote services for fetal ultrasound evaluations in areas with limited access to expert centers. 6 –8 To our knowledge, there are no prior articles describing efforts to expand fetal telecardiology during the time of COVID-19 pandemic and very limited data on fetal telecardiology in general. 4,5,8
The objective of this study is to describe our center's experience in rapidly expanding fetal telehealth services to safely reach patients during the COVID-19 pandemic. The study aims to evaluate the feasibility of a fetal telecardiology program during the COVID-19 pandemic, including assessing the number of patients seen, indication for fetal echocardiogram, and accuracy of diagnosis. It was hypothesized that fetal telecardiology visits would be accurate at diagnosing critical congenital heart disease (CCHD), but slightly less accurate than in-clinic fetal echocardiograms, however, that the difference in diagnosis would be minor and would not result in any adverse outcomes.
Materials and Methods
A retrospective review of fetal telecardiology visits between March 15 and July 15, 2020, was performed. Data were collected including location of study, indication for study, diagnosis, management, and follow-up recommendations. When available, the chart was reviewed for confirmation of diagnosis postnatally. The number of telemedicine studies performed during this 4-month period was compared with the number performed before the pandemic. This is a project undertaken as a quality improvement initiative at Children's National. As such it was designated as a quality improvement initiative, and not under the oversight of the institutional review board.
Since 2003, Children's National pediatric cardiologists have partnered with MFM offices with the overall goal of increasing prenatal detection rates of CCHD. Children's National is a large tertiary care pediatric hospital, located in Washington, DC, and serving the larger DC metropolitan area. Through expanding fetal cardiology services to MFM offices, the goal was to reach mothers in regions farther away from the hospital. Sonographers at these MFM offices received hands-on in-person training on fetal echocardiography views and technique through working with the pediatric cardiologists during bimonthly clinics.
The fetal telemedicine program at Children's National was added to fetal cardiology services in July 2019 to allow pediatric cardiologists to provide fetal and cardiology services at multiple locations, to increase access to care outside typical weekly clinics, and minimize service interruptions. Before March 15, 2020, fetal telemedicine visits had been conducted at one community MFM site. However, with the outbreak of COVID-19, and given the barriers for obstetric patients to attend in-person fetal cardiology clinic visits, there was an increased demand for fetal telemedicine services. By May 2020, five MFM clinics were participating in fetal telemedicine, with the closest <4 miles away and the farthest 23 miles away. Four pediatric cardiologists provided fetal telehealth services during this time. When possible, the fetal tele-echocardiography was performed at the same time as the fetal anatomy scan or the fetal growth scan to minimize additional clinic visits for the mother.
At the first MFM telemedicine site that was piloted before the pandemic, a telehealth linkage was established (hardware/CODEC provided by ViTel Net, Inc. [McLean, VA], VIDYO used for connectivity). Four rooms were set up with cameras and the study could be viewed live. The cameras also allow for direct conversations with the pediatric cardiologist reading the study. At all sites, after the study was completed, picture archiving and communications system (PACS) access through a secure remote desktop was used for image review and reporting through the MFM imaging system (Table 1). Patients were imaged from the standard fetal echocardiography views, and studies were transmitted to be reviewed in real time or later in the day. The sonographers all had prior experience and training with fetal echocardiography views from when the pediatric cardiologist was in office for consultations. When the study was performed live, additional views could be requested by the pediatric cardiologist reviewing the study.
Telehealth Technology at Maternal Fetal Medicine Clinics
DICOM, Digital Imaging and Communications in Medicine; MFM, maternal fetal medicine; PACS, picture archiving and communications system.
After the fetal echocardiogram was complete, the pediatric cardiologist reviewing the study would counsel the family on the results through videoconferencing or set up a follow-up appointment to discuss in person with the family. The patient would be instructed whether additional follow-up was required at the MFM clinic or at the tertiary care children's hospital.
Results
Expansion of Fetal Telemedicine:
Between March 15, 2020, and July 15, 2020, there was a large increase in the number of studies performed through telecardiology with a maximum of 53 studies performed in April 2020, increased from an average of 5–6 studies per month (Fig. 1). A total of 122 mothers were seen through fetal telecardiology visits between the five MFM clinics. A total of 152 fetal scans were performed. The majority of mothers had their initial visit through telehealth. Four mothers were first seen at the tertiary care children's hospital and had subsequent follow-up through telehealth visits. By comparison, during the same time period, 153 mothers (159 fetal scans performed) were evaluated in person at MFM offices and 180 mothers (226 fetal scans performed) in person at the tertiary care children's hospital.
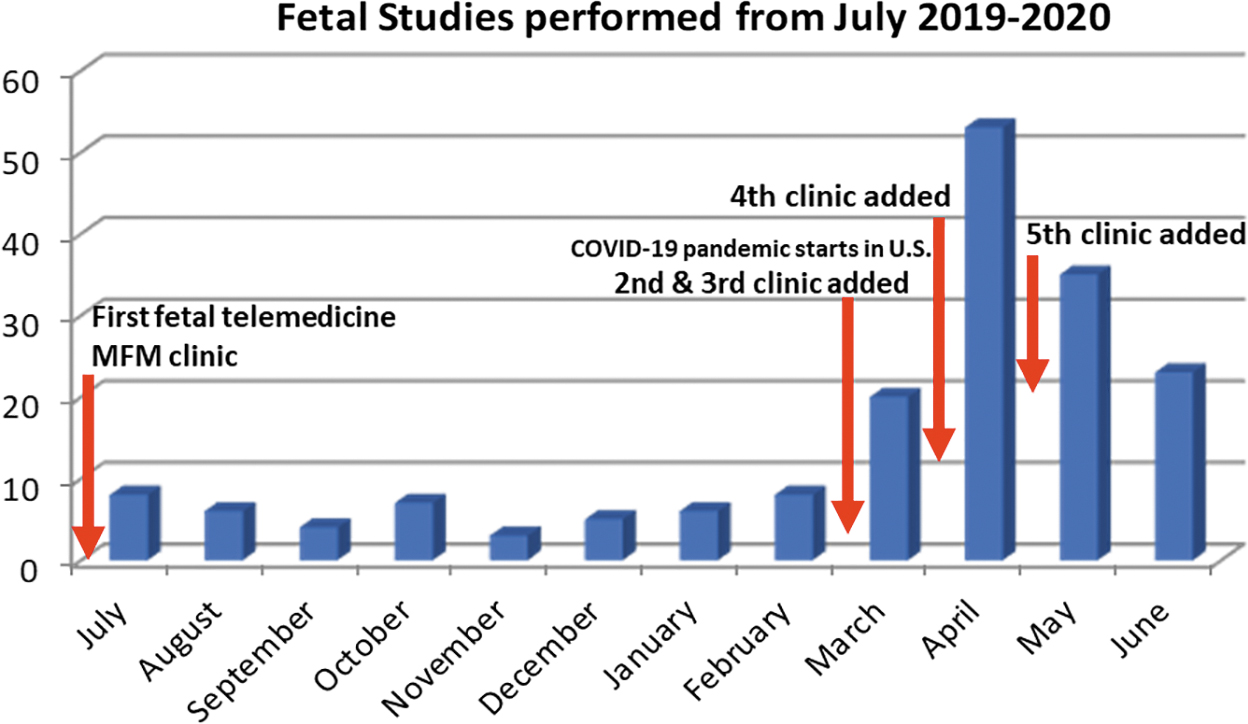
Expansion of fetal telemedicine over time.
Indications for Fetal Telecardiology
The most common indication for fetal telehealth echocardiogram was in vitro fertilization (n = 36; 4 with twin gestation). Other indications included abnormal findings on general fetal ultrasound, fetus with genetic abnormalities, fetus of a mother with diabetes mellitus, fetus with a family history of a cardiac abnormality, fetus of a mother with SSA antibodies, monochorionic or dichorionic twin pregnancy, and fetus of a mother with medication exposure (Fig. 2).

Indication listed for initial fetal echocardiogram. In some cases, there was more than one indication for fetal echo. *IVF category includes four multiple pregnancies. FH, family history; IVF, in vitro fertilization; US, ultrasound.
Abnormal Studies
There were 14 mothers (11.5%) who had abnormal fetal echocardiograms at their telehealth visit requiring additional follow-up, and a total of 19 abnormal fetal echocardiograms (12.5%) were performed during this time. Of all the mothers who participated in fetal telecardiology, 5.7% (n = 7) had fetal echocardiograms suspicious for a CCHD including hypoplastic left heart syndrome, hypoplastic left heart variant, interrupted aortic arch, tetralogy of Fallot, and tetralogy of Fallot with major aortopulmonary collaterals (Table 2). Two of these patients had their initial diagnosis made at an in-person fetal cardiology clinic visit, and had subsequent follow-ups with telemedicine. The remaining five diagnoses of CCHD were initially made by fetal telecardiology services, with four scheduled for subsequent in-person clinic follow-up and counseling. One mother was followed exclusively with fetal telecardiology visits until delivery.
Congenital Heart Diseases Diagnosed and/or Followed by Fetal Telecardiology
Postdelivery Follow-Up
All of the fetal echocardiograms suspicious for CCHD were confirmed postnatally with no alteration in diagnosis. To our knowledge, none of the normal fetal echocardiograms were found to have congenital heart disease (CHD) postnatally.
The majority of fetal echocardiograms with non-CCHD were also confirmed postnatally. Two fetal echocardiograms with non-CCHD, double aortic arch and mild transverse arch hypoplasia, were found to have normal postnatal echocardiograms. However, the same diagnoses were made on follow-up in-person fetal echocardiograms before delivery. For the double aortic arch, the patient will follow up at 1 year with consideration for magnetic resonance imaging if there are symptoms.
Discussion
This is the first study to describe the experience of expanding fetal telecardiology services during the COVID-19 pandemic. Owing to extenuating circumstances of the pandemic, our fetal telecardiology program rapidly expanded and it proved to have good accuracy. During the 4-month period reviewed, 122 mothers were seen by fetal telecardiology services and five new diagnoses of CCHD were made. Two prior diagnoses of CCHD were able to be followed up by fetal telecardiology. Fetal telecardiology was found to be accurate in those diagnosed with CCHD, with no significant diagnostic errors using telecardiology.
The previously developed infrastructure of training and working with sonographers at MFM offices proved to be crucial in the rapid expansion of telemedicine. The obstetric (OB) sonographers' prior experience of performing fetal echocardiograms with a pediatric cardiologist on site allowed for expertise with studies being performed independently during telemedicine.
Previous studies have shown fetal telecardiology to be a feasible way to diagnose CHD. Mothers have reported a high level of satisfaction, and typically preferred telehealth visits to an in-person appointment at the local hospital. 4,5,9 Our study showed that >120 mothers were able to successfully be seen during the COVID-19 pandemic. In addition, telecardiology benefited mothers by reducing additional COVID-19 exposure and other barriers to additional in-person fetal clinic visits. Telecardiology also reduced additional exposure for providers and sonographers.
With the COVID-19 pandemic, telehealth has rapidly expanded across the country to continue to provide pediatric cardiology care. 2 However, recent publications have discussed the challenges of fetal cardiology given the need for an in-person fetal echocardiogram during the visit, and have, therefore, suggested weighing the risk of exposure against the utility of performing the study. 2,3 The American Society of Echocardiography has published a statement for triaging mothers based on the risk profile. 10 Based on this statement, many of the mothers seen by our telemedicine fell into the “low-risk” group. However, our study found that patients of all risk groups can be evaluated by telecardiology services in collaboration with an MFM physician. Our experience with fetal telecardiology was concordant with the statement, which noted that telehealth can serve as the initial screening for CHD, provide interval follow-up counseling for known CHD, and provide additional maternal support offsite. 10 In our fetal telehealth experience, the majority of new diagnoses of CCHD were referred for an in-person follow-up visit to allow for additional echocardiogram images and counseling.
Prenatal detection of CCHD in the United States for patients requiring surgical intervention within 6 months of birth remains ∼40%, and there is significant variability across regions and types of heart defects. 11,12 It remains unclear how the COVID-19 pandemic will ultimately affect the prenatal detection of CCHD. However, given the scaling back of programming and fetal clinics across the country, there is risk for a decrease in prenatal diagnoses during this time period. Expansion of fetal telemedicine programs may reduce barriers to detection and is an area for future research.
This is the first study describing efforts to expand fetal telecardiology during the time of the COVID-19 pandemic. Our center's experience with expanding fetal telecardiology services demonstrated that it is a feasible way to reach mothers without sacrificing the accuracy of diagnosis. However, the expansion of a telemedicine program requires strong initial infrastructure, prior relationships with MFM providers, and appropriate training among obstetric sonographers.
This study describes a single-center experience. While we documented no inaccurate or missed diagnoses, we cannot confirm outcomes for those diagnosed with a normal heart. However, no patients were referred to our center who had a normal fetal echocardiogram during their telecardiology visit.
Conclusions
The fetal telecardiology model of working collaboratively with MFM providers is a feasible strategy to reduce potential exposure for pregnant mothers during the COVID-19 pandemic without compromising diagnostic accuracy. This fetal telecardiology model may be useful even after the pandemic is over to improve rates of prenatal detection of CCHD. Future studies are needed to assess MFM, sonographer, and patient perspectives on fetal telecardiology during the COVID-19 pandemic. The effect of fetal telecardiology on health care spending is also an area for future research.
Footnotes
Authors' Contributions
All authors contributed to a portion of the conceptualization and design of this study. Drs. Sheri Hamersley, Kimberly Hickey, Homa Ahmadzia, Richard Broth, Thomas Pinckert, Craig Sable, Mary Donofrio, and Anita Krishnan collaboratively conceptualized and designed the fetal telecardiology expansion discussed in this article. Dr. Bryanna Schwartz, Dr. Jen Klein, and Ms. Megan Barbosa performed further conceptualization for the format of the article and performed data acquisition. All authors worked on drafting or providing critical revisions to the articles' content. All authors approved of the final version submitted.
Disclosure Statement
No competing financial interests exist.
Funding Information
Philanthropy from the Seelig Cardiology Research Fund.