
Abstract
Background:
Teleconsultations have been an indispensable part of the public health armamentarium during the COVID-19 crisis. Many physicians replaced face-to-face consultations with teleconsultations for the very first time. This study aimed to understand telemedicine uses by physicians during the lockdown period and explain the changes in their teleconsultation practices after the reopening of an outpatient department.
Methods:
A mixed-method analysis was used. First, a quantitative study was conducted with a retrospective analysis of the ratio of all teleconsultations and physical consultations between January 1 and July 31, 2020. Second, semidirective interviews were undertaken with physicians to better understand the dynamics of teleconsultation use.
Results:
In total, 28 physicians practiced 603 teleconsultations over the study period. The rate of teleconsultations was 0.2% before the lockdown (January 1 to March 15, 2020), reaching 19.5% during the lockdown (April 2020), and decreasing to 8.4% at the reopening of the physical outpatient facilities. Based on the dynamics of their teleconsultation uses, four medical departments were selected for the qualitative study component (neurology, urology, pneumology, and anesthesiology). From the semistructured interviews, the main uses of telemedicine were for patients living with “chronic but under control” conditions that received follow-ups. Physicians also identified practices to improve patient empowerment and nurse autonomy. The results of the anesthesiology department showed that teleconsultations must be more codified to meet the same standards of quality as face-to-face consultations.
Conclusion:
The COVID-19 outbreak and lockdown period triggered a wider use of teleconsultations and have allowed physicians to think about new uses and opportunities.
Introduction
Telemedicine activities have widely been described in many countries for a variety of uses, 1 –4 including epidemic situations in the past 10 years. 5 In the recent pandemic, not only has telemedicine been used directly for needs related to the outbreak but it has also become suitable for routine care that has been affected or disrupted by COVID-19. 6,7
In terms of its motivation for its use, an expressed deterrence for expanding telemedicine has often been about pricing. 8 During the COVID-19 crisis, telemedicine, particularly through the practice of teleconsultations, was a means to providing medical expertise while respecting social distancing. Many countries authorized or eased telemedicine reimbursement, 9,10 and even though it was the same in France, 11 recent legislative changes have extended the funding scope of its activities. Video teleconsultation and asynchronous tele-expertise have been reimbursed by the National Health Insurance Scheme since 2018 and 2019, respectively. 12,13 In this favorable environment, telemedicine was largely employed during the French lockdown period put into effect in March and April 2020, with an overall total of 5.5 million teleconsultations conducted nationwide by physicians, making up ∼27% of all medical consultations. 12
At a local level, the public hospital group in Troyes has been developing its own telemedicine strategy through two projects. The first has allowed linking specialist physicians with 36 nursing homes located in the region. 14 The second has been an outpatient teleconsultation program for patient follow-ups. During the lockdown period, telemedicine activity of the hospital grew considerably. Physicians who had never used telemedicine before started practicing it. Since the removal of the lockdown and reopening of outpatient physical consultations, however, there was a significant decrease in teleconsultations. The objectives of this study were to (1) understand how French physicians used telemedicine during the lockdown period for the COVID-19 outbreak, (2) explain the changes in teleconsultation practices after the reopening of the outpatient department, and (3) highlight levers for integrating telemedicine in the physicians' daily routine practices.
Methods
A mixed-method analysis was conducted with both quantitative and qualitative methods. A mixed-method analysis was chosen because it provides an understanding of large, complex, and multifaceted environments such as telemedicine. 15 Based on Caffery et al., we used a sequential explanatory design 16 and first conducted the quantitative data analysis before the qualitative study that helped to further understand the outcomes.
Our quantitative study was a monocentric and retrospective analysis of the ratio of all teleconsultations and physical consultations between January 1, 2020, and July 31, 2020. The same ratio for every medical department involved in the same period was also analyzed. From this first analysis, four medical departments were picked based on the dynamics of their ratio (Quantitative Study section), and semistructured interviews were conducted with physicians by the first author, male, PhD, and member of the hospital public health research team. In addition, the data of the qualitative study were analyzed using a thematic analysis approach. 17
Results
Quantitative Study
Within the six health care departments that practiced teleconsultations, 28 specialty physicians practiced remote consultations for their own outpatient consultations (n = 603) during the period from January to July 2020. Furthermore, teleconsultations for outpatient activity increased from 0.2% before the lockdown from January 1 to March 15, 2020 (n = 16) to 13.4% (n = 240) during the following lockdown period between March 16 to May 10, 2020. Its use peaked between April 6 to April 26, 2020, with the highest proportion of teleconsultations performed at 19.5% (n = 43) of the total number of teleconsultations (Fig. 1).
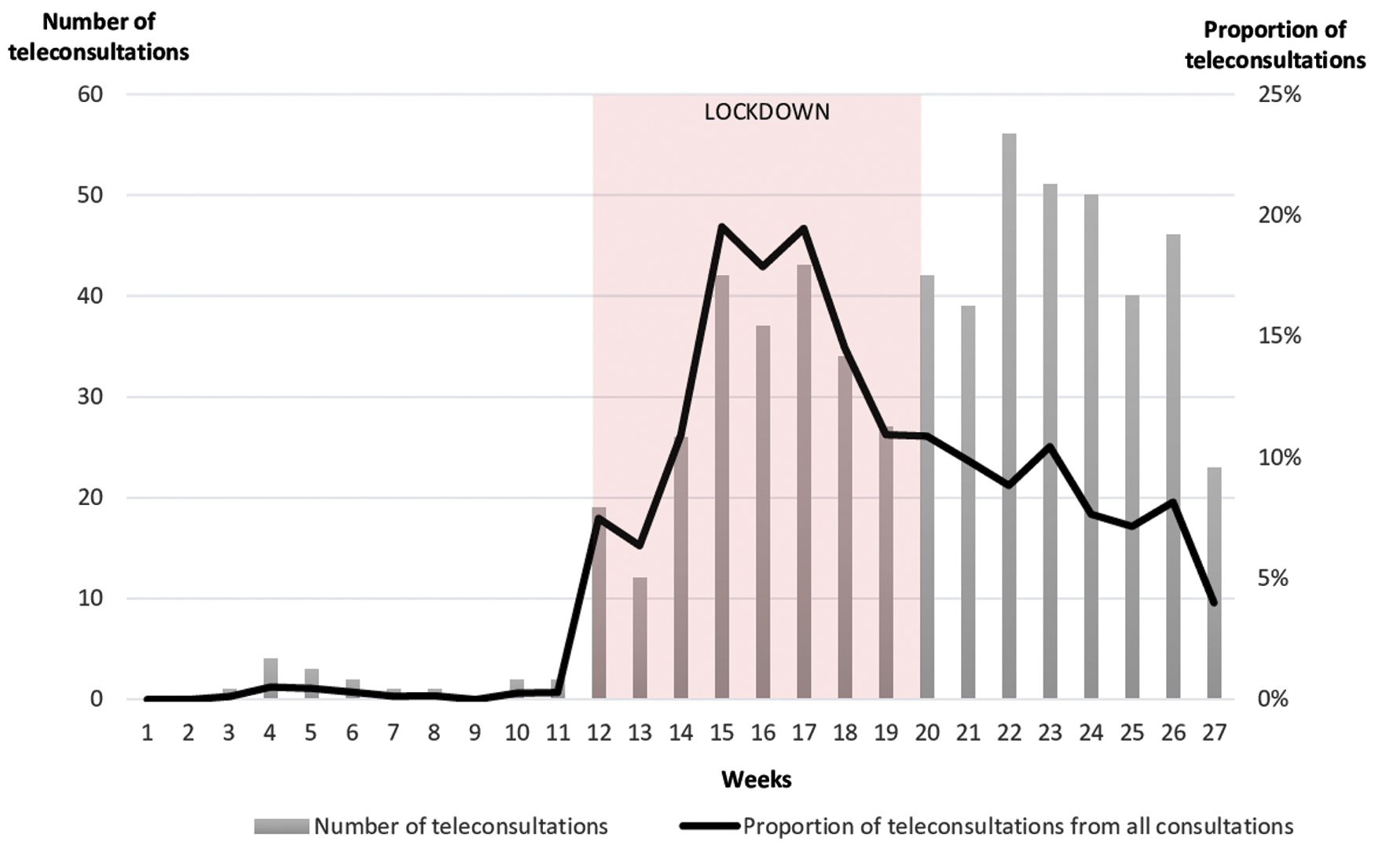
Number of teleconsultations during the COVID-19 outbreak at Troyes Hospital.
In terms of medical specialties, departments with the highest use of teleconsultations were anesthesiology, neurology, and urology, representing 84% of all teleconsultations. Outpatient teleconsultation activity in these three specialties reached 65% during the lockdown but decreased to 11% toward the end of it. Similarly, the proportion of teleconsultations also generally declined at the end of the lockdown between May 11 and June 30, 2020, from 19.5% to 8.4%, which may have been influenced by the reopening of the physical outpatient facilities.
The neurology department extensively used remote consultations during the lockdown period but completely stopped since it ended. The use of teleconsultations in the urology department decreased since the end of the lockdown and remained low in routine after. The pneumology department decreased its uses of teleconsultations during the lockdown but increased since July 2020. The anesthesiology department's use of teleconsultations during the lockdown was only for pregnant women in their last trimester. The use started in the lockdown and remained at a high number after its end.
Qualitative Study
The qualitative study aimed to explain the quantitative outcomes. Four physicians, one from each of the four selected departments at the local hospital, participated in it and the description of the interviews is presented in Table 1.
Description of Interviews by French Physicians on Performing Teleconsultations During the COVID-19 Lockdown at Troyes Hospital
Teleconsultation as a tool to limit follow-up interruptions
Management of chronic conditions involves a systematic follow-up with some consultations needing a physical examination. Other follow-ups are based on anamnesis and analysis of complementary examination results. Both these types of follow-ups can be performed with a teleconsultation: “These were follow-ups of conditions for which anamnesis could be enough. Many conditions did not need a physical exam” (ID 1). Video consultations were considered an optimal strategy when a patient's health condition was stable and physicians showed limited interest in the management of more complicated situations. In these cases, teleconsultations were used by physicians as a tool to guide a care plan and prepare face-to-face consultations: “Most of the time, when everything was fine, it could be enough. But as soon as the patient's condition was not good, it was not easy to manage it remotely” (ID 1).
Using teleconsultations allowed the emergence of new practices that may improve patient empowerment: “I gave a peak flow meter to a patient who suffers from non-well-balanced asthma because it is a good tool for self-measurement. With these measures and a questionnaire our team developed, I am trying to improve her asthma remotely by teleconsultation” (ID 2). It also allowed to strengthen the autonomy of nurses, delegating certain follow-ups to them: “We have delegated some sleep disorders follow-ups to a nurse for 10 years now. At the beginning of the lockdown, I started to do them again [by teleconsultation] before saying: Wait a minute, our nurse does it better than us, she used to do it before, she can keep doing” (ID 2). Moreover, it revealed an invisible but time-consuming part of the physicians' job: “I stopped doing teleconsultations since the end of the lockdown, but this is something we could discuss because we already have remote consultations by phone, but they are not appreciated” (ID 1).
Teleconsultations also shook up conventional thinking. A physical consultation is a well-known formal exercise and it was now necessary for a practitioner to think of teleconsultation codes and conform them into their routine medical practice: “I even had a patient going to the supermarket. Her husband was driving, and their kids were playing at the back of the car… and she was talking to me. This is a medical consultation, so it needs to happen in a proper context. I don't even think this patient will remember she had an anaesthesiology consultation” (ID 4).
Specific feedback from the anesthesiology department
Since 2018, the anesthesiology department has conducted preanesthetic teleconsultations with prisoners. They have been aimed at limiting prisoner transfers and ensuring better privacy. During a teleconsultation, a physician from the prison's health department works with an anesthetist from the hospital. At the beginning of the lockdown period, anesthesiologists were acquainted with remote consultations and moreover were offered obstetric anesthesiology teleconsultations for pregnant women in their last trimester and women with interrupted pregnancies. Access to the operation rooms was restricted for emergencies only and the anesthesiology consultations related to these surgeries were kept face to face.
According to one of the physicians interviewed, despite the implementation of the recommendations from the French Society of Anaesthesiology and Resuscitation (SFAR), obstetrical anesthesiology teleconsultations during the lockdown were not fitted well with quality standards. Transferring the clinical examination to a doctor may have allowed doing the exact same consultation as one that is face to face. On the contrary, patients did not have physical medical assistance during their obstetric anesthesiology teleconsultations. It was only a form of preconsultation that must be completed on the day of delivery or hospitalization: “What we did with the maternity department were minimal consultations. Just for the patients to have some notions of anaesthesiology, like taking an epidural on the day they come to deliver a baby. But we only did step one on three of the usual anaesthesiology consultation and we had to complete answering questions later during the physical exam” (ID 4).
Taking an obstetric anesthesiology teleconsultation outside of extreme health care situations where physical consultations are not possible or cause high risk did not seem to be as favorable: “Considering the COVID-19 outbreak, this is a solution we should keep in mind. But apart from it, I prefer face-to-face consultations with pregnant women” (ID 4).
Improvements of an existing outpatient teleconsultations program
The lessons learned from using teleconsultations during the lockdown period can be used to restructure the outpatient teleconsultation program in the Troyes local hospital. Whenever possible and with the consent of patients, each physician should be able to offer a teleconsultation. Thus, it is possible to alternate the use of face-to-face consultations and teleconsultations ensuring regular and appropriate follow-ups by reducing travel for patients living far from the hospital. To do so, physicians have to change their minds and habits too: “For some follow-ups, we could individually pick some stable patients and propose to them to alternate face-to-face consultations with teleconsultations” (ID 1).
In addition to its occasional use, teleconsultations could become the gold standard of the management of some pathologies. After the first face-to-face consultation (legal requirement), all follow-ups could be managed remotely. Two topics that emerged quickly were follow-ups of osteoporosis (mainly based on biological examination) and follow-ups of sleep disorders: “The management of sleep apnea using a continuous positive airway pressure machine and the follow-ups consultations are well-codified. I think all the sleep apnea follow-ups could be done remotely” (ID 2).
In addition, a wider use of teleconsultations was shown to free up clinical time for other consultations needing a face-to-face interaction, especially when delivering a difficult prognosis: “Face-to-face consultation slots are scarce. To look at a blood test, you do not need a 30-minute consultation. Teleconsultation is time-saving” (ID 3).
Furthermore, the Troyes outpatient teleconsultation program may need to be reorganized to be fully operational. One key suggestion could be introducing the program more effectively to as many physicians as possible: “We started remote consultation by phone because we didn't know a teleconsultation service was available. We have discovered it later” (ID 1). It may also be necessary to invest in telemedicine software licenses and equipment in which case both should not be a limitation for physicians to use telemedicine: “Do we have digital tablets enough? We are five physicians [in neurology] doing consultations, sometimes at the same time. At the hospital scale, lots of physicians are consulting at the same time a day” (ID 1).
Finally, new procedures and workflows should be produced from the appointment booking to the sending point of the consultation reports and prescriptions, passed by the management of network failures if it occurs during a teleconsultation: “In the beginning, I was badly organized. I am also always late to face-to-face consultations, but you cannot be late during teleconsultations because people cannot wait for you behind a blank screen for more than 5 minutes. […] For now, I have sent a report after every teleconsultation not by sending an e-mail but by posting it because I didn't know if it was allowed or not” (ID 2).
From the experiences at the anesthesiology department, working on a charter of teleconsultations may seem to be mandatory now and it should be sent to the patients and signed before the teleconsultation begins to get their informed consent followed with an explanation of the rules to ensure a high-quality consultation.
Discussion
Despite telemedicine being legal in France since 2009, as well as practiced since 2004 and fully reimbursed since 2018, physicians still have opportunities to apply it in their daily practice. This study aimed to understand the motivations of physicians to use telemedicine based on their experiences during the COVID-19 outbreak. It is considered an initial step in improving the outpatient teleconsultation program at the Troyes Hospital in France. Based on our interview findings, the COVID-19 outbreak and first lockdown triggered the use of teleconsultation but did not allow it to be routine practice.
Moreover, telemedicine for nurses may improve the current quality of care by strengthening the autonomy of nurses. 18 In our study, a specialist nurse who dealt with sleep disorders kept having her own follow-up teleconsultations, and another was also about to commence teleconsultations for patients with intestinal stomas. In a recent literature review, Markus Biehl identified factors present in cases of the successful deployment of information technology and communication projects. 19 To date, the outpatient teleconsultation program in Troyes does not fit all those factors.
To gain a stronger experience in the COVID-19 outbreak, the practice of teleconsultations at the Troyes Hospital should be improved and a focus should be given to reconsider the current situation including the purpose, organization, expected benefits for patients, physicians, and institution. This consideration should be performed with as many health care providers as possible, as well as health authorities and patient organizations in a coconstructive approach. Moreover, there is a need to define and implement the clinical guidelines and adapted training for health care professionals, in addition to dedicated telemedicine strategies and protocols for hospitals and health care facilities aimed at supporting such changes. These actions will allow us to better face global health challenges in the future.
This was a preliminary study with several limitations. One limitation was that our study had a monocentric selection of physicians and an undocumented data saturation as a qualitative study. Nevertheless, the results helped us identify relevant points for future studies and to better organize the teleconsultation outpatient department: from appointment booking to the process of sending medical reports and prescriptions.
Conclusion
This study aimed to understand the use of telemedicine from French physicians at a local French hospital before and after the lockdown period during the COVID-19 outbreak. Our findings indicated that physicians mainly used telemedicine for follow-ups of already known patients. Physicians also envisioned telemedicine practice for improving patient empowerment and the autonomy of nurses to also apply teleconsultations in their practice. This study was the first step to renew the outpatient teleconsultation program in the Troyes Hospital. Further research using mixed-methods methodology is needed to improve understanding in the future.
Footnotes
Acknowledgments
The authors thank all physicians who participated in this project.
Authors' Contributions
C.C., R.O., and S.S. conceptualized and designed the study. C.C. collected the quantitative data. R.O. and S.S. contributed to the quantitative analysis. C.C. conducted the semistructured interviews. C.C., R.O., and S.S. contributed to the qualitative analysis. C.C., R.O., and S.S. contributed to the discussion and wrote, reviewed, and edited the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.