
Abstract
Background:
Little is known about electronic consultation (e-consult) utilization during the COVID-19 pandemic when health systems rapidly implemented and scaled telehealth alternatives to in-person care. It is also unknown if e-consult utilization during the pandemic replaced or merely deferred the need for a specialty appointment. We evaluated if primary care providers' (PCPs) e-consult utilization and specialists' recommendations for specialty appointments changed after the transition to telemedicine during the COVID-19 pandemic.
Methods:
This cohort study used an interrupted time series analysis of e-consult utilization in a large, urban academic health care system between December 1, 2019, and June 27, 2020; the post-telemedicine time period began March 15, 2020. The primary outcome measure was the odds of an e-consult ordered during a PCP appointment; the secondary outcome measure was the odds of a specialist recommending a specialty appointment in an e-consult.
Results:
During 193,263 PCP appointments, 1,318 e-consults were placed to internal medicine subspecialties. Compared to the pre-telemedicine time period, the odds of a PCP ordering an e-consult increased (OR 1.04, 95% CI [1.02–1.07]) and the odds of specialists recommending specialty appointments increased (OR 1.11, 95% CI [1.06–1.15]).
Conclusions:
E-consult use increased following the transition to telemedicine in the context of the COVID-19 pandemic, suggesting that PCPs consider the e-consult a valuable tool for patient care when there is limited availability of specialty appointments. However, recommendations for specialty appointments following an e-consult also increased, suggesting that the e-consult may not replace the need for a specialty appointment.
Introduction
The use of e-consult (electronic consultation), which is a provider-to-provider asynchronous exchange of patient information using a secure electronic platform, 1 has emerged as a useful tool for primary care providers (PCPs) to quickly obtain nonurgent, patient-specific, expert advice from specialists. The COVID-19 pandemic forced health systems to rapidly implement and scale telehealth alternatives to in-person care to prevent exposure to the contagious respiratory virus. A recent study from Massachusetts General Hospital assessed COVID-19-associated changes in requests for e-consults before and after the start of the COVID-19 pandemic and found that e-consult utilization increased compared to traditional ambulatory specialty appointments after the COVID-19 public health emergency declaration in Massachusetts. 2 It is not known if this same trend was seen in other health care systems or if this phenomenon is specialty specific. Benefits of e-consult use include reducing the need for specialist appointments 1 ; however, it is not known if e-consults ordered during this time of rapid change in health care replaced or merely deferred the need for a specialty appointment.
At our institution, e-consults have been available as an alternative to in-person specialty appointments since 2018. 3 PCPs can choose whether to order an e-consult versus a referral for a specialty appointment, allowing autonomy of decision-making for the preferred method of obtaining specialty expertise. PCPs and specialty e-consultants have the understanding that if a question posed in an e-consult cannot be answered without evaluation of the patient, a specialty appointment will be recommended, and urgent appointments will be facilitated by the e-consultant. At the start of the COVID-19 pandemic in the United States, in-person specialty appointments were eliminated and replaced by telemedicine appointments in an attempt to slow transmission of COVID-19. The supply of specialty telemedicine appointments was reduced from the previous supply of in-person appointments as many specialists were redeployed to care for hospitalized patients with COVID-19. These shifts in type and supply of specialty appointments may have caused an increase in e-consults ordered as a way to overcome the limitation in specialty appointments. PCPs who may have previously favored requesting a specialty appointment to address certain issues may have instead ordered an e-consult for cases in the setting of limited specialty appointments. As a result, specialists may have been able to answer questions about management appropriately without the need for a specialty appointment.
With new limitations on access to specialty care in the context of the COVID-19 pandemic, we hypothesize that (1) the odds of a PCP ordering an e-consult during a PCP appointment increased after the transition to telemedicine for all specialties and (2) the odds of a specialty appointment recommendation in an e-consult decreased after the transition to telemedicine, particularly for specialties that utilize laboratory and imaging data to make recommendations such as endocrinology and hematology. By investigating these outcomes, we can understand PCPs' use of e-consults in the setting of a drastic shortage of specialty appointments, as well as understand the feasibility of an increased number of consult questions to be addressed using an e-consult without the need for a specialty appointment.
Methods
STUDY DESIGN, SETTING, AND PARTICIPANTS
This cohort study examined e-consult utilization in outpatient practices between December 1, 2019, and June 27, 2020, which includes time periods before and after the COVID-19 pandemic-related transition to telemedicine. This study was approved by the Montefiore/Albert Einstein Institutional Review Board. Montefiore Medical Center, the academic medical center of the Albert Einstein College of Medicine in the Bronx, New York, provides primary and specialty care in a network of outpatient practices, with over 3 million visits annually. Primary care practices include teaching sites, which are Federally Qualified Health Centers (FQHCs) or FQHC Look-Alikes, which include medical trainees and attending physicians with academic appointments; and nonteaching sites, which include FQHCs and community sites without medical trainees. Most patients (∼75%) are publicly insured by Medicaid and/or Medicare.
At our institution, an ambulatory e-consult program increased access to expert advice in multiple specialties. 3 When a consult question does not require a patient evaluation or patients have barriers to appointments (such as scheduling conflicts or difficulty with transportation), PCPs have the option of ordering specialty e-consults as an alternative to a referral request for a specialty appointment. Within the e-consult order, PCPs answer two prompts: (1) Please provide a brief summary of the patient and (2) Please provide your questions for the e-consultant. They have the ability to ask questions about the need for appointments; however, there is no specific field for appointment requests. Both teaching and nonteaching sites have the same access to e-consults and specialty appointment referrals; however, in a previous analysis of e-consult use at our institution, it was discovered that PCPs at teaching sites were more likely to order e-consults than PCPs at nonteaching sites. 3 Specialists review the e-consult order and give recommendations along with an assessment of whether a patient requires a specialty appointment to complete the consult question. As an incentive for participation, PCPs and consultants are compensated a flat amount for each e-consult completed; this stayed consistent during the study period.
The week starting March 15, 2020, outpatient practices eliminated all nonurgent in-person appointments and transitioned to telemedicine, starting with telephone appointments, and later followed by an option for telephone or video appointments. During this transition to telemedicine, PCPs retained the ability to make referrals for specialty appointments. Many PCPs and specialists were deployed to the inpatient setting to care for patients with COVID-19, thereby restricting the number of available outpatient appointments and disrupting the normal workflow for scheduling appointments. Thus, PCPs were encouraged through communication between physician leaders to order e-consults if specialty expertise was needed. After the surge of patients with COVID-19 declined starting June 2020, in-person appointments for primary and specialty care gradually increased.
VARIABLES AND DATA SOURCE
An e-consult is defined as an electronic communication between a PCP and specialist provider initiated by a PCP placing an e-consult order in the electronic medical record. A PCP appointment is defined as either an in-person or virtual (telephone or video) encounter, which includes an internal medicine or family medicine PCP and patient. A specialty appointment is defined as either an in-person or virtual (telephone or video) encounter, which includes a specialist and patient. The pre-telemedicine time period was from December 1, 2019, to March 14, 2020, and the post-telemedicine time period was from March 15, 2020, to June 27, 2020. In the pre-telemedicine time period, all appointments were in person. In the post-telemedicine time period, all appointments were conducted through telemedicine platforms (telephone and video) from March 15, 2020, to June 7, 2020, and a minority of visits were in person from June 7 to June 27, 2020. Implementation of e-consult orders for specialties included in this study occurred from February 2018 to November 2019. Thus, to compare time periods with similar length, we evaluated the months immediately preceding the transition to telemedicine. The primary outcome measure was the odds of an e-consult being ordered during a PCP appointment before and after the transition to telemedicine. This was stratified by site type (teaching or nonteaching) and e-consult specialty. The secondary outcome measure was the odds of a specialist recommending a specialty appointment in an e-consult before and after the transition to telemedicine. This was stratified by e-consult specialty. We included internal medicine specialties that were available for e-consults before the study period: cardiology, endocrinology, gastroenterology, hematology, hepatology, infectious disease, and rheumatology. All data were obtained from the electronic medical record system.
ANALYSIS
Data were analyzed with interrupted time series analysis, which is used to evaluate health intervention outcomes where there is a clear differentiation of the pre-intervention period and the post-intervention period. 4 All analyses were conducted using logistic regression. The primary outcome variable was whether an e-consult was ordered during a PCP appointment (yes/no); the secondary outcome variable was whether a specialty appointment was recommended in an e-consult (yes/no). The key independent variables included time periods before transition to telemedicine, which measures the pre-transition time effect corresponding from December 1, 2019, to March 14, 2020, time periods after transition to telemedicine, which measures post-transition time effect corresponding to March 15, 2020, to June 27, 2020, and an indicator variable of transition, which measures the immediate effect due to the transition. In the first model, the weekly odds of e-consults for selected internal medicine specialties during a PCP appointment visit were examined before and after the transition to telemedicine adjusted for PCP site type. In the second model, the first model was repeated for each e-consult specialty. In the third model, the weekly odds of specialty appointments recommended in an e-consult were examined before and after the transition to telemedicine. In the fourth model, the third model was repeated for each e-consult specialty. For each outcome, we examined the rate of change in weekly odds pre-telemedicine, the immediate effect of transition to telemedicine on the odds, and the rate of change in weekly odds post-telemedicine. We also compared the rates of change in weekly odds (after vs. before) using chi-square tests.
Results
During the study period from December 1, 2019, to June 27, 2020, PCPs at 20 sites completed a total number of 193,263 appointments; 107,229 pre-telemedicine and 86,034 post-telemedicine. During this time, 1,318 e-consults were placed to cardiology, endocrinology, gastroenterology, hematology, hepatology, infectious diseases, or rheumatology; 729 e-consults to pre-telemedicine; and 589 consults to post-telemedicine. Less than half of all e-consults recommended a specialty appointment; 333 pre-telemedicine and 289 post-telemedicine.
UTILIZATION OF E-CONSULTS
Before the transition to telemedicine, there was random variation in the weekly odds of e-consult orders during PCP appointments (Fig. 1). Following the transition to telemedicine, the weekly odds immediately decreased and then the slope increased (Fig. 1). This pattern was seen in both teaching and nonteaching sites; however, throughout the study period, teaching sites had higher odds of ordering an e-consult per PCP visit compared to nonteaching sites (Fig. 1).
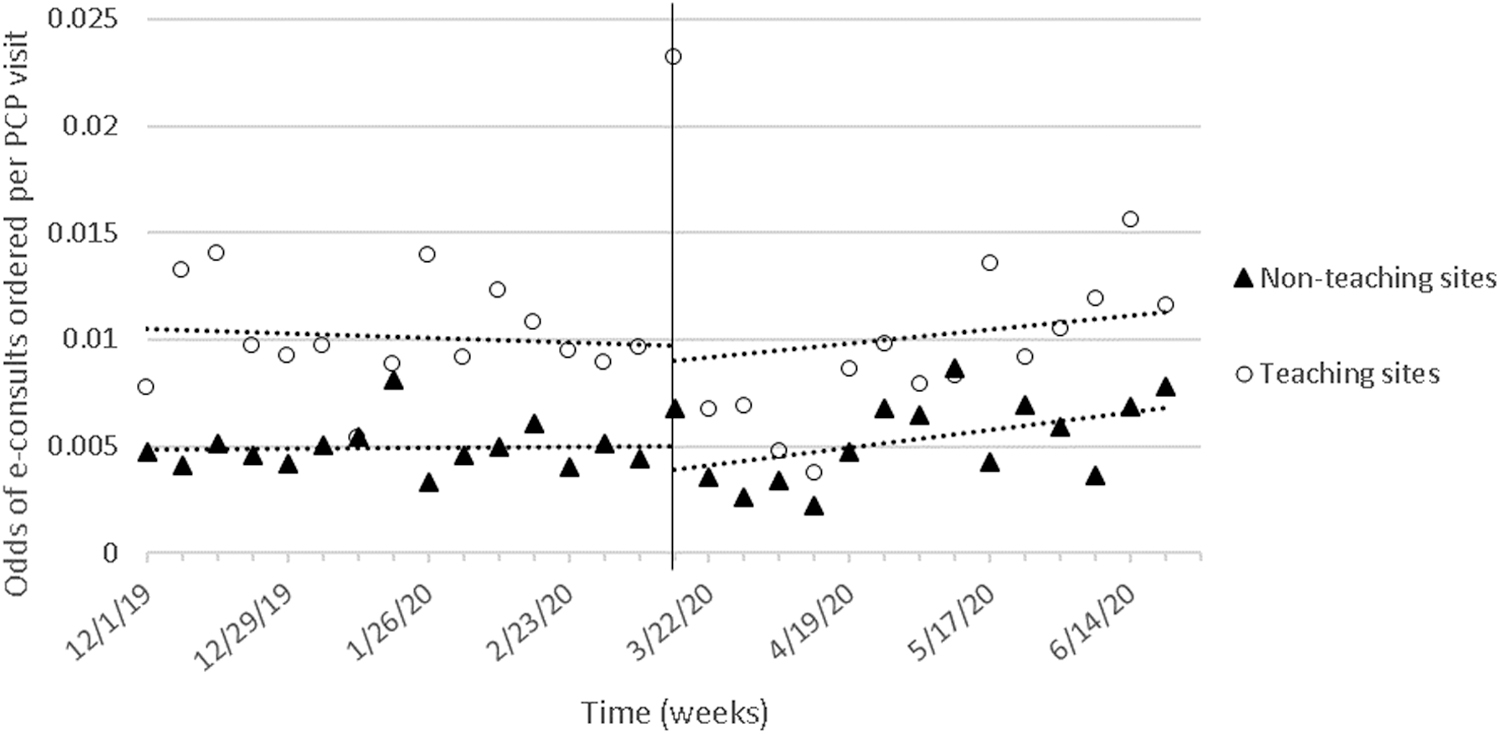
The weekly odds of e-consults ordered during a PCP appointment before and after the transition to telemedicine associated with the COVID-19 pandemic. The vertical line on March 15, 2020, indicates the week of transition to telemedicine. e-consult, electronic consultation; PCP, primary care provider.
The interrupted time series analysis reflects these findings (Table 1). For all specialties combined (Table 1, Model 1), in the pre-telemedicine period, there was no significant change in odds of an e-consult order from week to week. There was a significant decrease in odds of e-consults ordered at the immediate transition to telemedicine (OR 0.78, 95% CI [0.62–0.98]). In the post-telemedicine period, the weekly odds of a PCP ordering an e-consult increased (OR 1.04, 95% CI [1.02–1.06]). The change in odds of an e-consult ordered per week was greater after the transition to telemedicine compared to before (OR 1.04, 95% CI [1.02–1.07]). Throughout the entire study period, the odds of a PCP ordering an e-consult were less at nonteaching sites compared to teaching sites (OR 0.51, 95% CI [0.46–0.57]).
Logistic Regression for the Weekly Odds of an Electronic Consultation Being Ordered During a Primary Care Provider Appointment During Different Study Periods (Before Transition to Telemedicine, at the Start of the Telemedicine Transition, and After the Transition to Telemedicine) by Primary Care Site Type (Nonteaching vs. Teaching)
Model 1 evaluates all internal medicine specialties participating in e-consults and Model 2 was repeated for each specialty individually.
95% CI, 95% confidence interval; e-Consult, electronic consultation; OR, odds ratio; PCP, primary care provider.
When looking at specialties individually (Table 1, Model 2), in the pre-telemedicine period, there was no significant change in odds of an e-consult being ordered from week to week in any of the specialties. In the post-telemedicine period, for a few specialties, the odds of e-consults being ordered increased each week: gastroenterology (OR 1.09, 95% CI [1.03–1.15]) and rheumatology (OR 1.10, 95% CI [1.03–1.17]); for the remaining specialties (cardiology, endocrinology, hematology, hepatology, and infectious disease), there was no significant change. When comparing the rate of change in the post-telemedicine versus pre-telemedicine periods, for endocrinology, there were increased odds of an e-consult being ordered per week (OR 1.06, 95% CI [1.01–1.11]); for the remaining specialties, there was no significant difference. When compared to teaching sites, nonteaching sites had lower odds of ordering an e-consult during a PCP visit for all specialties during the entire study period, except for infectious diseases in which the odds of ordering an e-consult during a PCP visit were similar between teaching and nonteaching sites.
RECOMMENDATION FOR SPECIALTY APPOINTMENT AFTER AN E-CONSULT
Before the transition to telemedicine, the odds that a specialty appointment recommendation was made in an e-consult increased over time. During the transition to telemedicine, there was an immediate decrease in the odds of a specialty appointment recommendation made, followed by an increase in odds of a specialty appointment recommendation made (Fig. 2).
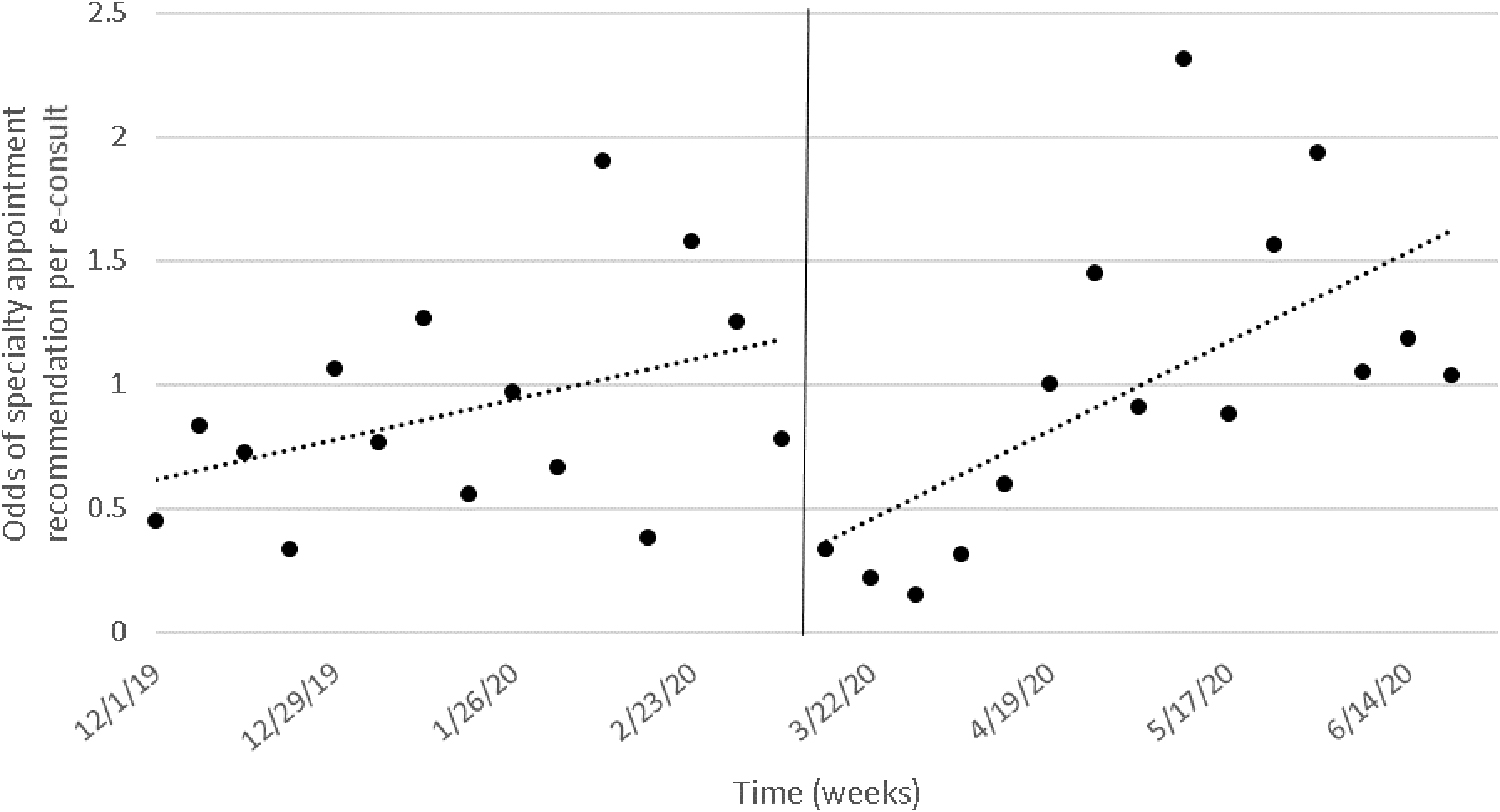
The weekly odds of an e-consult recommendation for a specialty appointment before and after the transition to telemedicine. The vertical line on March 15, 2020, indicates the week of transition to telemedicine.
The interrupted time series analysis reflects these findings (Table 2). In all specialties combined, in the pre-telemedicine period, there was an increase in weekly odds of a specialty appointment recommendation (OR 1.04, 95% CI [1.01–1.08]), followed by a significant immediate decrease due to the transition (OR 0.38, 95% CI [0.24–0.61]), and finally followed by a significant increase in weekly odds (OR 1.11, 95% CI [1.06–1.15]) during the post-telemedicine period. This increase in specialty appointment recommendation was greater during the post-telemedicine period compared to the pre-telemedicine period (OR 1.06, 95% CI [1.01–1.12]) (Table 2, Model 3).
Logistic Regression of Weekly Odds of a Specialist Recommending an Appointment in an Electronic Consultation During Different Study Periods (Before Transition to Telemedicine, at the Start of the Telemedicine Transition, and After the Transition to Telemedicine) *
Site type variable is not included in this analysis.
Model 3 evaluates all internal medicine specialties participating in e-consults and Model 4 was repeated for each specialty individually.
When looking at specialties individually (Table 2, Model 4), in the pre-telemedicine period, there was an increase in weekly odds of specialty appointment recommendation in endocrinology (OR 1.09, 95% CI [1.02–1.15]); for the remaining specialties (cardiology, gastroenterology, hematology, hepatology, infectious disease, and rheumatology), there was no significant change. In the post-telemedicine period, two specialties experienced an increase in the weekly odds of specialty appointment recommendation gastroenterology (OR 1.13, 95% CI [1.01–1.26]) and infectious disease (OR 1.31, 95% CI [1.10–1.57]); for the remaining specialties (cardiology, endocrinology, hematology, hepatology, and rheumatology), there was no significant difference. When comparing the rate of change in the post-telemedicine versus pre-telemedicine periods, the following specialties had an increase in weekly odds of specialty appointment recommendation: gastroenterology (OR 1.20, 95% CI [1.01–1.42]), rheumatology (OR 1.39, 95% CI [1.06–1.81]), and infectious diseases (OR 1.33, 95% CI [1.07–1.66]).
Discussion
The COVID-19 pandemic forced health care systems to adapt by transitioning from in-person visits to primarily telemedicine in early 2020. As anticipated, we found that PCPs increased their use of specialty e-consults after the transition to telemedicine when the availability of outpatient appointments was limited. The rapid decrease in e-consult orders at the immediate start of the transition to telemedicine likely reflects the abrupt nature of the transition and the overburdening of resources at the start of the COVID-19 pandemic. The overall increase in e-consult use may reflect PCPs' adaptation to the new system and the new momentum and routine created for ordering e-consults. This is consistent with previous findings that e-consult utilization increased compared to traditional ambulatory referrals following the limitation in appointments in the context of the start of the COVID-19 pandemic. 2
In particular, we found that endocrinology had a significant increase in the use of e-consult by PCPs following the transition to telemedicine compared to before. Although in pre-telemedicine times, a PCP might readily refer a patient to endocrinology for diabetes management, when such a referral is not easy to arrange, a PCP may be more willing to communicate with an endocrinologist through e-consult because of the availability of data for use (e.g., blood glucose readings and number of units of insulin administered). For all other specialties, except hepatology and infectious disease, we found a positive trend in use of e-consult in the post-telemedicine period versus the pre-telemedicine period; however, this trend was not statistically significant. Previous studies have evaluated PCPs' complex perceptions of e-consults, with some PCPs reporting positive experiences due to perceived empowerment in being able to manage a patient's care further than usual, while other PCPs viewed the shift in care responsibility negatively. 5 –7 In times of severe shortage of specialty appointments, PCPs may be more willing to use the e-consult to communicate with specialists regarding patient care.
Unexpectedly, we found that the odds of specialists recommending an appointment following an e-consult increased in the post-telemedicine period compared to the pre-telemedicine period for all specialties combined. In the pre-telemedicine period, the majority of e-consults were completed without the need for a specialty appointment, while post-telemedicine, approximately half of e-consults led to a specialty appointment. When looking at specialties individually, we found that the odds of specialists recommending an appointment following an e-consult increased in the post-telemedicine period compared to the pre-telemedicine period for gastroenterology, rheumatology, and infectious disease. This suggests that for the increased number of e-consult questions, specialists believe a direct interaction with the patient is necessary to appropriately treat and manage the patient's care. It also suggests that the e-consult and the associated communication between PCP and specialist alone may not be able to meet patient's needs. While many e-consult programs measure success by the ability to answer questions without the need for a specialty appointment, 1,8 –10 we believe that the use of an e-consult to facilitate timely specialty care should not be considered an e-consult failure. Others have also reported that e-consults can serve as a valuable tool to expedite specialty appointment referrals since this may be necessary to prevent the potentially detrimental consequences of delaying specialty care. 11 In challenging situations such as the COVID-19 pandemic of 2020, e-consults may serve as a way of expediting patient evaluation and management in the primary care setting through PCP-specialist collaboration, which would otherwise be delayed, given shortages of specialty appointments.
An important limitation in our study is that the COVID-19 pandemic was associated with many unique challenges in staffing and patient care in our system, which may not be generalizable to other health systems. Because New York City was the epicenter of the first wave of COVID-19 in the United States, the health care system was overburdened in terms of staff and resources, while simultaneously transitioning to telemedicine. In addition, we did not examine the specific questions in the e-consult pre-telemedicine and post-telemedicine. E-consults could have been placed explicitly to facilitate future specialty appointments as opposed to a means of obtaining expert advice on patient management. Although we did not consider this a failure, other hospital systems might place greater value in avoiding a specialty appointment altogether. Also, without in-person PCP appointments, there may have been a decrease in abnormal laboratory or imaging findings, which may have previously prompted an e-consult or specialty appointment request. As a result, there may have been fewer e-consults ordered than if laboratories and imaging were ordered at the usual frequency. Finally, we did not qualitatively evaluate PCP decision-making regarding ordering an e-consult and specialist decision-making regarding recommendation for a specialist appointment; PCPs may have been less selective about e-consult utilization in post-telemedicine times, which may have had an impact on the need for specialty appointments. Because we compared consecutive months rather than the same months in two different years, there may be unmeasured confounders related to seasonal variation in health care utilization and reasons for PCP visits. While the holiday season may impact the volume of PCP visits, we do not expect that the proportion of visits with questions requiring specialty expertise would change significantly.
Conclusions
We found e-consult use increased during the COVID-19 pandemic, suggesting that the e-consult is a valuable tool for PCPs using telemedicine. However, recommendations for specialty appointments following an e-consult also increased, suggesting that the e-consult may not entirely replace traditional specialty appointment referrals. Further research should be conducted to explore PCPs' and specialists' perceptions of the utility and importance of e-consult use in the context of telemedicine and limitations in appointment availability, which may streamline the outpatient specialty referral system and improve patient care.
Footnotes
Authors' Contributions
C.L. made substantial contributions to conception and design of work, interpretation of data for work, and drafting the work. C.Z. made substantial contributions to design of study and the analysis of data for the work, revising the work. S.R. made substantial contributions to conception and design of work, acquisition and interpretation of data for work, and drafting and revising the work. C.L., C.Z., and S.R. gave final approval of the version to be published.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.