
Abstract
Introduction:
Coronavirus disease 2019 (COVID-19) is a highly contagious viral infection. Hospitals worldwide have decreased face-to-face visits to reduce the exposure to the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Prenatal and postpartum care are essential for the health of women and their fetuses. Therefore, many hospitals have incorporated telehealth into their protocols.
Objectives:
The aim of this review was to determine how health care organizations are responding to the COVID-19 pandemic by incorporating telehealth visits into their protocols for obstetrics care, what services were converted to telehealth, and its benefits and barriers.
Method:
A computerized literature search was performed using PubMed and Cumulative Index of Nursing and Allied Health Literature (CINAHL) databases using terms, including “telehealth,” “virtual visits,” “obstetric,” “pregnancy,” “postpartum,” and “COVID-19” for articles published before October 2020. Peer reviewed articles and guidelines were included in this review.
Results:
A total of 25 articles were identified. Fifteen articles reported protocols. During this pandemic, protocols developed replaced some in-person visits with telehealth visits, when no testing or vaccinations are required. The main reported benefits were minimizing exposure to SARS-CoV-2 and the continuity to provide high-quality and safe care. Lack of access to high-speed internet and hardware and inaccessibility to patients were the most reported barriers.
Conclusion:
Telehealth provided the opportunity for reducing in-person visits during the COVID-19 pandemic. Some prenatal services could be completely provided through telehealth and others require medical equipment to be delivered. Health care organizations recognized that using telehealth could be continued beyond this pandemic, as they provided many benefits for patients, medical staff, and the organizations themselves.
Introduction
Coronavirus disease 2019 (COVID-19) is caused by the novel coronavirus that was first reported in Wuhan, China, in late 2019. 1 –3 It is a highly contagious viral infection that causes respiratory illness and persistent distortion of the lungs, which may result in severe symptoms and even death. 4 –6 In March 2020, the World Health Organization (WHO) declared the spread of COVID-19 a global pandemic. 7 By November 2, 2020, there were more than 46 million confirmed cases of COVID-19 and more than 1 million related deaths worldwide. 8 The WHO recommends social distancing, wearing masks, ventilating rooms well, cleaning hands more frequently, and coughing into the elbow or a tissue to prevent the spread of COVID-19. 9
Vulnerable populations, such as pregnant women, are at a higher risk of developing complications from viral respiratory infections. 10,11 However, pregnant women need continuous prenatal care to prevent morbidities and mortalities in both themselves and their fetuses. 12,13 Prenatal care includes nutritional and genetic consultations, and education about pregnancy, childbearing, breastfeeding, newborn care, and more. 12,14 Women in developed countries attend between 7 and 14 prenatal care visits during their pregnancies. 11,15 There are inconsistencies regarding the ideal number of prenatal care visits. For example, the WHO recommends a minimum of 8 visits, whereas the Royal College of Obstetricians and Gynecologists (RCOG) recommends a minimum of 6. 16,17 A study conducted by Carter et al. found that women who attend more than 10 visits during their pregnancies have a higher rate of intervention, such as induction of labor or cesarean delivery, with no more improvement in health outcomes than those who attend 6 or 8 visits. 18
Hospitals worldwide have reduced face-to-face visits, suspended elective procedures and nonurgent outpatient visits, and replaced some of these appointments with telehealth visits. These measures benefit both patients and health care professionals by encouraging social distancing and preventing unnecessary exposure to COVID-19. 19 –23 Telehealth is defined as “the use of electronic information and telecommunication technologies to support long-distance clinical health care, patient and professional health-related education, public health, and health administration.” 24 Telehealth comprises three categories: (1) synchronized (real time), (2) asynchronized (store-and-forward), and (3) remote patient monitoring. 25 On the other hand, telemedicine, which is used often interchangeably with telehealth by both consumers and health care providers, is considered part of telehealth that focuses on providing medical services on distance. 26
Telehealth has been used in the obstetrics field for several services, including consultations, ultrasounds, fetal echocardiography, and postpartum care. 27 The Obstetric (OB) Nest model, designed in the United States before the COVID-19 pandemic, replaces some physical obstetric care visits with telehealth. 28 OB Nest was widely accepted by patients and providers, and it was associated with stronger relationships between pregnant women and their care teams as well as increased continuity of care. 28,29 One study examined OB CareConnect telehealth program and found that pregnant women who received virtual care were more satisfied than in-person patients with the care they received. 30 Furthermore, a randomized trial by Barbour et al. found that using telemedicine for patients with low-risk pregnancies saved time and was associated with lower costs. 31
The aim of this scoping review was to determine how health care organizations are responding rapidly to the COVID-19 pandemic by incorporating telehealth visits into their protocols for obstetric care, what types of obstetric services were converted to telehealth, the benefits that telehealth can provide for medical practices, and the barriers these organizations are facing when implementing telehealth during the COVID-19 pandemic.
Methods
A scoping review is a type of literature review that aims to “map the literature on a particular topic or research area and provides an opportunity to identify key concepts; gaps in the research; and types and sources of evidence to inform practice, policymaking, and research.” 32 It was used in this study to rapidly map the current available evidence in this study area since the topic was not extensively reviewed before. 32,33 The findings of this review may be useful to policymakers, considering incorporating telehealth into obstetric care services. 32 This study followed the Preferred Reporting Items of Systematic Reviews and Meta-analysis (PRISMA) methodology with its extension for scoping reviews (PRISMA-ScR). 34 The study's protocol was not registered.
SEARCH STRATEGY
The search was conducted in three parts to find relevant published articles and gray literature. Initially, a computerized literature search was performed using PubMed and Cumulative Index of Nursing and Allied Health Literature (CINAHL) databases. Some of the search terms used were “telehealth,” “virtual visits,” “obstetric,” “pregnancy,” “postpartum,” and “COVID-19” (Table 1). The second search was conducted using Google and Google Scholar. The final search involved checking reference lists. The search identified all articles that discussed the use of telehealth in obstetric care during the COVID-19 pandemic. Eligibility criteria refined the selection according to the review objectives.
Search Strategy
COVID-19, coronavirus disease 2019; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2.
ELIGIBILITY CRITERIA
All articles that reported their prenatal and postpartum care protocols, benefits of using telehealth during the COVID-19 pandemic, or barriers inhibiting the use of telehealth during the pandemic were included in the study. Articles published in English before October 8, 2020, were included in the review. This scoping review included all types of articles, including all studies, guidelines, and expert opinions. Under circumstances such as a pandemic, when rapid responses are needed, expert opinions provide the best available evidence. 35 The authors excluded the articles that did not match the objectives of the study according to the inclusion and exclusion criteria described in Table 2.
Eligibility Criteria
GDM, gestational diabetes mellitus.
STUDY SELECTION
Two reviewers (H.M. and S.D.) conducted the search and extracted a total of 104 articles. Cohen's Kappa test was used to assess the agreement between the two authors, as proposed by Landis and Koch. 36 The reviewers independently performed the initial screening based on titles and found 53 articles eligible for abstract screening (kappa (κ) = 0.73; substantial agreement). Following abstract screening, 46 articles were included for full-text review (κ = 0.41; moderate agreement). Full-text screening yielded 18 articles to be included in the study (κ = 0.66; substantial agreement). The kappa coefficients were statistically significant (p < 0.005) (not a chance agreement). Discrepancies were discussed and resolved by consensus between the reviewers. Seven additional articles were identified as gray literature.
DATA CHARTING
Data charting forms were developed by the two authors (H.M. and S.D.) to determine the data to be extracted. HM charted the data and discussed the results with SD. Data regarding the included articles were extracted (Appendix Table A1). The data included author name, country, type of article, type of telehealth, medical services, settings, and key outputs. Other charting forms include obstetric services by type of visits, sources of protocols, protocols which identified types of visits in each time period, and benefits and barriers.
SYNTHESIS OF RESULTS
Included articles were analyzed according to the main outputs (protocols, benefits, or barriers). Sources of protocols were identified. Then, all protocols were grouped in a table to represent the agreement between them according to weeks and type of visits, a bar chart was used to represent the previously mentioned table. Types of obstetric services—such as ultrasound, laboratory tests, and education—are summarized in a table with frequencies. Benefits and barriers of using telehealth in obstetric care during the COVID-19 pandemic were grouped according to the beneficiaries (patients, providers, and health care organizations).
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
No ethical approval was required for the purpose of this article.
Results
The search strategy summarized in Table 1 yielded 108 total articles. Following the removal of duplicates (n = 4), 104 articles remained for the title and abstract screening. This screening excluded 58 articles from the study. The full text of 53 articles were reviewed, including seven gray literature articles and guidelines identified from Google search, Google Scholar, and reference screening. Ultimately, 25 articles matched the review objectives according to the inclusion and exclusion criteria. (Fig. 1) displays the flow of article selection according to the PRISMA guidelines. 37 The details of the included articles are summarized in Appendix Table A1. The majority of the included articles originated from the United States (n = 14, 56%). 11,22,23,38 –48
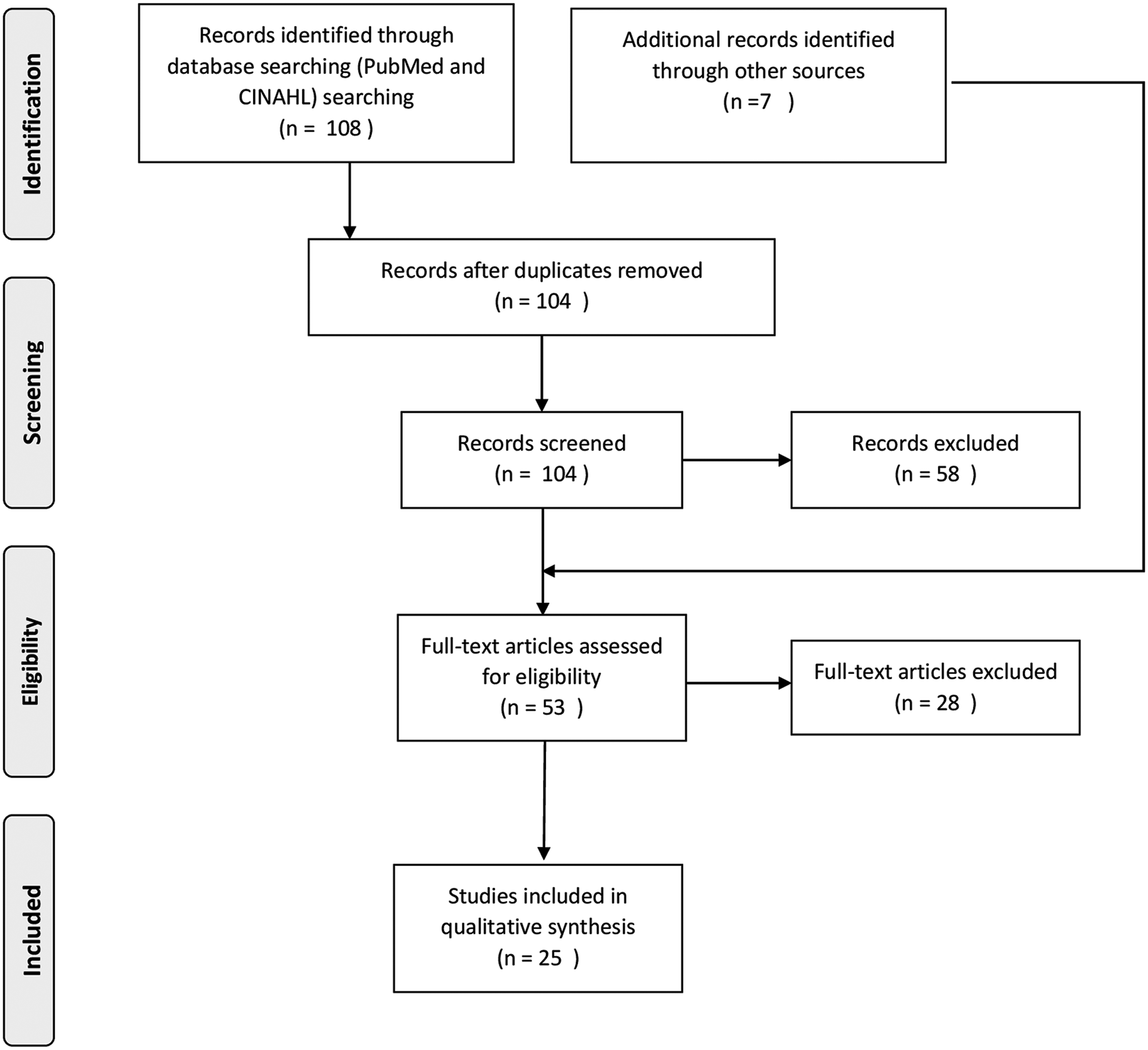
PRISMA flowchart for included articles. CINAHL, Cumulative Index of Nursing and Allied Health Literature; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
OBSTETRIC CARE SERVICES
According to the articles included in this review, variation exists in the frequency of patients' obstetric visits and modes of delivery. However, some articles suggested conducting all obstetric visits virtually, except those that require laboratory testing, ultrasound, or other procedures. 11,17,20,23,41,42,49 Services such as ultrasounds, laboratory tests, physical examinations, genetic screenings, and vaccinations cannot be done virtually from home (Table 3). One exception is the protocol set forth by Dosaj et al., in which contracted pharmacies provide self-swab kits for sexually transmitted infection screenings. They also plan to provide a mail-in option for the collected specimens. 42 Another suggestion for reducing in-person visits is to group services that require women's attendance into one visit per trimester. 42
Obstetric Services by Types of Visits
1-h GCT, one-hour oral glucose challenge test; BP, blood pressure; GBS, group B streptococcus; HIV, human immunodeficiency virus; OGTT, oral glucose tolerance tests; RBC, red blood cells; ROS, review of systems; Rx, medical prescription; TDAP, tetanus, diphtheria, pertussis; TOLAC, trial of labor after cesarean.
Telehealth visits can be conducted to provide education, review medical history, discuss testing options and results, and conduct mental health and surgical site checks. 17,21 –23,40 –42,48,50,51 Health care providers can assess incisions and surgical sites for normal deliveries or cesarean sections using high-quality skin images sent by patients. 23,38,41,42 Telehealth can also be used to provide family support during delivery. 40 Other services can be conducted virtually depending on patients' and hospitals' resources. For example, patients at home can measure vital signs and fetal heart tones if they have devices such as blood pressure (BP) cuffs, cardiotocographs, weight scales, and dopplers. 20,22,40,42,48 Providers can also teach women how to measure fundal height so they can report it virtually. 42 Hokkaido University Hospital mails a cardiotocograph and a sphygmomanometer to each pregnant woman to be used during a telehealth visit and returned afterward by a delivery company. 20 It also mails any medication prescribed during telehealth encounters. 20 Anesthesia consultations can be performed by emailing questionnaires to women. 21 The Department of Obstetrics and Gynecology (OB/GYN) at the University of Illinois at Chicago (UIC) used telehealth another way; they used a temporary routing provider schedule allowing physicians to present at the hospital 1 week to provide in-person appointments and stay at home the next week to provide telehealth care. 42
TELEHEALTH PROTOCOLS FOR OBSTETRICS CARE DURING COVID-19 PANDEMIC
Fifteen articles proposed or reported protocols, representing 60% of the total articles included in this review. 5,11,17,21 –23,38,40 –43,48,50 –52 Only nine articles reported postpartum care in their protocols. 5,11,17,22,23,38,41,50,51 The majority of the protocols were developed based on expert opinions, literature reviews, or recommendations by scientific societies (n = 13; 86.7%). The sources of these protocols are listed in Table 4.
Sources of Protocols
ACOG, American College of Obstetricians and Gynecologists; APRO, Pacific Regional Office; INESS, Institute of Economic and Social Studies; NICE, The National Institute for Health and Care Excellence; OB, Obstetrics; SMFM, Society for Maternal-Fetal Medicine; UIC, University of Illinois at Chicago; UNFPA, The United Nations Population Fund; WHO, World Health Organization.
More than half of the 15 protocols (n = 9; 60%) recommended fewer than seven face-to-face visits. 5,11,21,41,48,50 –52 On the other hand, these protocols recommended between 2 and 8 prenatal telehealth visits. The majority of the included articles proposed more frequent in-person visits than telehealth visits (n = 10; 66.7%) (Table 5). 11,17,22,23,38,40,42,43,51,52
Obstetric Visit Protocols During the COVID-19 Pandemic
“○” indicates option of F2F or TH visits.
Optional visits are counted in the total of telehealth visits only.
F2F, face-to-face; T, total; TH, telehealth; Wk, week.
PRENATAL CARE
The first trimester of pregnancy refers to weeks 1–13 of gestation. 53 For this trimester, 60% (n = 9) of the protocols suggested that the initial visit (up to week 10) should be a telehealth visit. 5,11,17,21,23,38,40 –42,48 Second visit, between weeks 11 and 13, should be a face-to-face visit. 11,17,21,23,38,40 –42,50,52
The second trimester refers to weeks 14–27 of pregnancy. 53 The protocols included in this review suggested two telehealth visits during this trimester, one between weeks 14 and 17 (n = 10; 66.7%) 11,17,21,23,38,40,41,43,48,51 and another between weeks 23 and 26 (n = 11; 73.3%). 11,21,22,38,40 –42,48,50 –52 Furthermore, 14 (93%) of the protocols recommended one face-to-face visit between those two visits. 5,11,17,21 –23,38,40 –43,48,51,52
The third trimester lasts from the 27th week until the pregnancy ends, which is usually in the 40th week. 54 More frequent visits are recommended during this trimester (see in Table 5). Of the protocols included in this review, 86% (n = 13) recommended a telehealth visit in weeks 29 to 35. 5,11,21,22,38,40 –43,48,50 –52 All protocols recommended a face-to-face visit in week 36, with the exception of Vivanti et al.'s protocol, which did not propose any visit (n = 14; 93%). 5,11,17,21 –23,38,40 –43,48,50 –52 Most protocols recommended in-person visits between the 27th and 28th weeks and during the 40th week (n = 11; 73.3%), (Table 5) and (Fig. 2) demonstrate the included protocols in further detail regarding frequency and types of visits.

Types of prenatal postpartum visits by weeks. PP, postpartum; Wk, week.
POSTPARTUM
Nine of the included articles discussed postpartum care. 5,11,17,22,23,38,41,50,51 The follow-up appointments in this stage occur from the first day of delivery until 8 weeks postdelivery. More than half of the articles suggested either virtual postpartum visits (n = 5; 55.6%) 5,11,22,23,41 or a combination of virtual and in-person visits (n = 3; 33.3%). 17,38,50 Only one article recommended that postpartum visits be exclusively in person. 51
BENEFITS OF TELEHEALTH FOR OBSTETRIC CARE AND ASSOCIATED BARRIERS DURING THE COVID-19 PANDEMIC
Benefits
Benefits of using telehealth during the COVID-19 pandemic were reported in 13 articles (52%), of the articles included in this study. 11,20,23,39,40,42 –44,46,47,55 –57 (Table 6) categorizes these benefits by patients, medical staff, and health care organizations. These benefits are also subcategorized into three main categories: access to care, maintaining high-quality care, and economic benefits. Benefits were primarily reported under the “patients” category (n = 19; 65%), followed by the “healthcare organizations” category (n = 6; 21%) and, finally, the “medical staff” category (n = 3; 10.7%).
Benefits of Using Telehealth for Obstetric Care During the COVID-19 Pandemic
PPE, personal protective equipment.
ACCESS TO CARE
The most commonly cited benefits for patients in this category were continuity of care (n = 5), 40,42,44,47,55 followed by greater access to services for patients in rural areas (n = 3), 39,46,47 and increased appointment attendance rates (n = 2). 43,47 Health care organizations experienced similar benefits, and, most importantly, they expanded care provision to more locations (n = 3). 39,46,47
MAINTAINING HIGH-QUALITY CARE
The most commonly reported benefits in this category were minimized exposure of both patients and medical staff to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) (n = 10), 11,20,23,39,40,42,44,47,56,57 providing high-quality care to patients (n = 5), 42,43,47,55,57 safe delivery of care (n = 4), 20,42,43,47 and the promotion of social distancing (n = 3). 43,46,47
ECONOMIC BENEFITS
Economic benefits include the following: convenience for patients with increased childcare responsibilities, which helped to reduce the need for childcare assistance (n = 3) 40,43,44 ; low user burden (n = 2) 43,56 ; less time away from work (n = 2) 43,56 ; eliminated transportation and parking costs (n = 2) 42,43 ; and reduced waiting times (n = 2). 43,47 Only one benefit—the reduction of travel time—was reported for medical staff providing care from home (n = 1). 47 Two benefits were reported for health care organizations; these included preservation personal protective equipment (PPE) (n = 3) 23,40,47 and accommodation of clinical staff who were suspected or confirmed to have the virus (n = 2). 47,56
BARRIERS
Nine (36%) of the included articles reported barriers faced when implementing telehealth during the COVID-19 pandemic. 39,40,42 –45,47,55,56 Health care organizations faced the largest number of barriers (n = 10), followed closely by patients and medical staff (n = 9 for both). Barriers were also divided into three categories—technical, time, and other barriers.
TECHNICAL BARRIERS
Technical barriers were the most commonly reported. Patients faced seven technical barriers, including a lack of high-speed internet connection (n = 4), 43 –45,56 a lack of smart devices (n = 3), 40,42,56 initial setup technical difficulties (n = 2), 40,44 and other technical barriers (Table 7). Medical staff members were affected by similar barriers; additionally, they experienced challenges in virtual interaction with families due to lack of video (n = 1), 45 inaccessibility of patients' medical information when providing care from home (n = 1), 56 and difficulty familiarizing patients with telehealth software (n = 1). 45 Health care organizations faced four technical barriers: a lack of videoconferencing hardware (n = 2), 43,45 unfamiliarity with telehealth administration and scheduling (n = 1), 44 a lack of integration between telehealth systems and Electronic Health Records (n = 1), 56 and the need for additional information technology (IT) staff (n = 1). 44
Barriers to Telehealth in Obstetric Care During the COVID-19 Pandemic
EHR, Electronic Health Records; IT, information technology.
TIME BARRIERS
Time barriers affected only health care organizations. Those barriers included the lack of time necessary to implement a telehealth service (n = 2), 42,43 the need for rapid integration (n = 1), 44 and the lack of time to test the system (n = 1). 44
OTHER BARRIERS
Other barriers included patients' concerns about the privacy of telehealth visits (n = 1) and the quality of health information provided online (n = 1). 56 Medical staff faced five barriers in this category, including difficulty reaching patients and conducting virtual visits because patients did not answer calls or reply to text messages (n = 3), 45,47,55 and difficulty translating for non-English-speaking patients (n = 2). 44,55 Two articles reported that health care organizations faced high implementation costs 39,40 and two reported compliance and billing issues. More information about the barriers can be seen in Table 7.
Discussion
OBSTETRIC CARE PROTOCOLS AND SERVICES
Many hospitals and health care organizations have adopted new protocols to engage telehealth in their obstetric care schedules to encourage social distancing and reduce in-person visits. 11,23,51 Although telehealth has been used previously in obstetrics care, several hospitals started using it only as a response to the COVID-19 pandemic. 38,40,47 Two of the previously adopted protocols are the OB Nest model and the OB CareConnect Program. 58,59 Mayo Clinic developed the OB Nest model for low-risk pregnancies to provide patient-centered care that allows pregnant women to play more active roles in their prenatal care and reduces in-person visits. 58 This model was used to develop similar protocols during the COVID-19 pandemic. 11,43 The OB CareConnect Program offers virtual visits as an option to provide more convenient obstetric care. 59 Both the OB Nest and the OB CareConnect Program recommend a total of 14 prenatal visits, 5 of them are telehealth and 2 postpartum visits, the first of which is to be held virtually 1 week after delivery. 58,59
Prenatal care usually consists of 7 to 14 in-person visits. 11,15 However, protocols proposed during this pandemic have replaced some in-person encounters with telehealth visits, therefore reducing the number of face-to-face visits between 3 and 9. At least 66% (n = 10) of the articles agreed on the time periods during which many of these visits should be conducted (Fig. 2). Protocols developed before the COVID-19 pandemic also agreed on many of these time periods. For example, both the OB Nest and the OB CareConnect models agree that virtual visits should be held during weeks 14–17, 23–26, and 29–35. 58,59 Furthermore, both of them proposed face-to-face visits during weeks 11–13, 18–22, 36, and 40. 58,59
Telehealth visits during the COVID-19 pandemic provide similar services to those before the pandemic. These services include education and home monitoring measurements, (e.g., vital signs and weight). 58,59 Both the OB Nest and the OB CareConnect models provide home monitoring devices to pregnant women, which in turn provides empowerment and enables patient-centered care. 58,59 From the protocols proposed during the pandemic, it is noticeable that hospitals that rely on patients to measure vital signs have fewer face-to-face visits in their schedules. 20,40 –42,48
All postpartum visits for normal pregnancies without delivery complications can be conducted virtually. However, protocols developed before the pandemic suggested one virtual visit and one in-person visit. 58,59
OBSTETRIC TELEHEALTH BENEFITS AND IMPLEMENTATION BARRIERS DURING THE COVID-19 PANDEMIC
The benefits and barriers reported by the articles included in this review were primarily described from the authors' viewpoints. Only one article qualitatively studied the benefits, barriers, and facilitators of implementing telehealth in obstetrics during the COVID-19 pandemic; this article also emphasized the scarcity of data on the use of telehealth in obstetric care. 44 Another article by Holcomb et al. measured patient satisfaction, which covered some benefits and barriers from patients' perspectives. 43
BENEFITS
Telehealth is not a new concept in obstetric care. 60 It was implemented primarily to reduce the cost of care, demedicalize the pregnancy experience, and provide more convenient care. 29,59 However, according to the available evidence, the most commonly cited benefit during the COVID-19 pandemic was the reduction of the exposure to the virus by way of reducing in-person visits. 11,20,23,39,40,42,44,47,56,57 A study conducted in 2004—at the time of the SARS virus—found that using telehealth to provide care for patients provides an opportunity to reduce the exposure to the virus. 61 Telehealth was also used during previous disasters to increase access to health care services. 62 Receiving adequate and equal prenatal care was a problem even before the COVID-19 pandemic. 63 During this pandemic, the barriers to accessible health care have been increased; this was particularly true during lockdown, when women had increased childcare responsibilities and were concerned about catching the virus. 23,42,55,56 Thus, telehealth offers the opportunity to deliver safe, high-quality, specialized, and continuous prenatal care. 20,40,42 –44,46,47,55,57
Another valuable benefit is the preservation of PPE. 23,42,47 This was especially beneficial in hospitals where there was a shortage of PPE and an associated rise in cost, while the WHO emphasized the importance of wearing masks to prevent COVID-19 infection. 9,64 PPE helps keep health care systems functional by maintaining the health of providers and preventing them from airborne transmission of SARS-CoV-2. 65
Many hospitals plan to continue using telehealth even after this pandemic, as it provides opportunities to expand their care coverage to other locations, including rural areas. 11,23,39,40,45 –47
BARRIERS
Many barriers inhibited the rapid implementation of telehealth during the COVID-19 pandemic. These barriers are similar to those affecting telehealth in general, but some may be mitigated or eliminated.
Technical issues and start-up costs are two barriers that were recognized before the pandemic and still exit presently. Technical issues include a lack of access to a high-speed connection, a lack of smart devices and equipment, and difficulties setting up or logging into telehealth software. 40,42 –45,56,66 Start-up costs include the costs of the platform, internet, equipment, additional IT support, and training. 39,40 To overcome some of these technical issues and decrease the initial costs, the telehealth program of the Parkland Health and Hospital System in Texas has implemented audio-only virtual visits. 41 Wu et al. suggested another way to reduce the initial cost of telehealth by relying more on “store-and-forward telemedicine,” for example, uploading glucose levels and BP measurements to an online platform to be reviewed by a consultant or receiving educational materials through online conferencing. 56 Two articles reported challenges using translation services during telehealth visits, which may be mitigated if any clinic team member speaks the patient's language. 44,56
Telemedicine has been underutilized in previous disasters because of reimbursement and licensing barriers. 62 However, the need to comply with Health Insurance Portability and Accountability Act (HIPAA) regulations and the lack of reimbursement for telehealth visits were two of the barriers mitigated during this pandemic in the United States. 11,40,66,67 The Office for Civil Rights at the Department of Health and Human Services decided not to impose any penalties for noncompliance with HIPAA regulations during the COVID-19 pandemic. 68 Furthermore, insurance companies in countries such as the United States and Australia began to reimburse virtual visits. 40,67,69 In addition, resistance to change was one of the most frequently cited obstacles in a previous systematic review of telehealth barriers. 66 However, none of the articles included in this review reported resistance to change during this pandemic, therefore indicating that telehealth could be one of the best solutions in disastrous times.
Time was a great obstacle with regard to implementing an integrated and tested system for some hospitals, whereas the pandemic accelerated the implementation of some planned (but not yet implemented) programs. 42 –44,48
LIMITATIONS
There are two limitations to this review. First, only English articles were included in this review. Second, there was a lack of rigorous studies evaluating the benefits and barriers of using telehealth in obstetric care during the COVID-19 pandemic, as it is still a new issue.
Conclusions
This review reveals that the majority of identified protocols were guided by expert opinions, scientific societies' recommendations, the best available evidence, and previous telehealth models. However, the protocols and guidelines were developed as a rapid response to a new and ambiguous disease. Therefore, they are subject to change as new information becomes available. Hospitals may reduce in-person visits by incorporating telehealth into their routine obstetric care and allowing women to take a more active role in their care (e.g., by measuring their vital signs) according to their available resources. Based on the reviewed articles, these protocols helped reduce exposure SARS-CoV-2, which was the main reason behind their implementation. Additionally, health care organizations recognized that these protocols could be continued even beyond this pandemic, as they provided many additional benefits for patients, medical staff, and the organizations themselves. 11,23,39,40,45 Nevertheless, more research is needed to investigate these benefits and barriers.
Authorship Confirmation Statement
This review was conducted by two authors (H.M. and S.D.). H.M. contributed to the study conception, design, analysis, and discussion. S.D. contributed to the study conception, design, critical revising, and giving the final approval.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was provided for this review.
Appendix
List of Included articles by Author
| AUTHOR | COUNTRY | TYPE OF STUDY | TELEHEALTH TYPE | MEDICAL SERVICES | SOURCE OF ARTICLE | KEY OUTPUTS |
|---|---|---|---|---|---|---|
| Aziz et al. 23 | United States | Not clear. | Real time. | Obstetrics, radiology, genetics. | Columbia University Irving Medical center. | Protocol, benefits. |
| Bindra 57 | India | Commentary. | Real time. | Obstetrics, gynecology. | Apollo Hospitals. | Benefits. |
| Boelig et al. 41 | United States, Italy | Guidelines. | Real time, store-and-forward. | Obstetrics, radiology. | Thomas Jefferson University, and University if Naples Federico II. | Protocol. |
| Dosaj et al. 42 | United States | Guidelines. | Real time. | Obstetrics, gynecology. | University of Illinois at Chicago. | Protocol, benefits, barriers. |
| Dotters-Katz and Hughes 22 | United States | Review. | Real time. | Obstetrics. | Duke University Medical Center. | Protocol. |
| Faden et al. 5 | Saudi Arabia | Guidelines. | Real time. | Obstetrics. | Saudi Society of Maternal-Fetal Medicine. | Protocol. |
| Fryer et al. 11 | United States | Not clear. | Real time, store-and-forward. | Obstetrics. | University of South Florida. | Protocol, benefits. |
| Holcomb et al. 43 | United States | Descriptive, cross-sectional study. | Real time (audio only) | Obstetrics. | Parkland Health and Hospital system. | Protocol, benefits, barrier. |
| Madden et al. 44 | United States | Observational, analytical study. | Real time. | Obstetrics, genetics. | Columbia University Irving Medical center. | Benefits, barriers. |
| Marshall et al. 45 | United States | Descriptive, cross-sectional study. | Real time. | Obstetrics, mental health, sociology. | The Florida Maternal, Infant, Early Childhood Home Visiting Initiative. | Barriers. |
| Nakagawa et al. 20 | Japan | Descriptive, retrospective study. | Real time. | Obstetrics. | Hokkaido University Hospital. | Benefits. |
| Pagliazzi et al. 49 | Italy | Descriptive, cross-sectional study. | Real time, store-and-forward. | Obstetrics, genetics. | Meyer Children's University Hospital. |
Benefits. |
| Palmquist et al. 46 | United States | Not clear. | Real time. | Lactation education. | Ready, Set, BABY. | Benefits. |
| Peahl et al. 48 | United States | Viewpoint. | Real time. | Obstetrics. | University of Michigan. | Protocol. |
| PSBC 52 | Canada | Guidelines. | Real time | Obstetrics. | Perinatal Services British Colombia. | Protocol. |
| Kimble et al. 51 | Australia | Guidelines. | Real time | Obstetrics. | Queensland Health. | Protocol. |
| Quinn et al. 55 | United Kingdom | Commentary. | Real time. | Obstetrics. | University Hospital of Leicester. | Benefits, barriers. |
| Ross-Davie et al. 17 | United Kingdom | Guidelines. | Real time. | Obstetrics. | RCOG. | Protocol. |
| Shields et al. 47 | United States | Observational, cohort. | Real time | Obstetrics. | Center for Maternal and Fetal Care, San Antonio, Texas. | Benefits, barriers. |
| Turrentine et al. 38 | United States | Commentary. | Real time. | Obstetrics. | Texas Children's Hospital Pavilion for Women. | Protocol. |
| UNFPA 50 | Guidelines. | Real time. | Obstetrics. | UNFPA | Protocol. | |
| Vivanti et al. 21 | France | Guidelines. | Real time, store-and-forward. | Obstetrics, Radiology, Psychology. | The French General Health Directorate, and the French National Authority for Health. | Protocol. |
| Vora et al. 39 | United States | Research letter. | Real time. | Obstetrics, genetics. | University of North Carolina at Chapel Hill. | Benefits, barriers. |
| Wu et al. 56 | China | Viewpoint. | Real time, store-and-forward. | Obstetrics. | Jinan University. | Benefits, barriers. |
| Zork et al. 40 | United States | Not clear. | Real time. | Obstetrics. | Columbia University Irving Medical center. | Protocol, benefits, barriers. |
RCOG, Royal College of Obstetricians and Gynecologists; UNFPA, The United Nations Population Fund.