
Abstract
Introduction:
Despite widespread investigation into the incidence of acute myocardial infarction during the coronavirus disease 2019 (COVID-19) pandemic and associated lockdown, no study has examined the situation's impact on blood pressure (BP) levels.
Methods:
Measurements of BP and heart rate (HR) were obtained from persons living in the Paris urban area using connected home BP monitors (accessible to patients and health providers through a secured server). Three time periods of e-health recordings were compared: during the pandemic before the lockdown, during the lockdown, and the same time period in 2019.
Results:
A total of 297,089 BP recordings from 2,273 participants (age 56.3 ± 12.8 years, 81.1% male) were made. During confinement, systolic BP gradually decreased by 3 mmHg (−2.4 to −3.9), and diastolic BP by 1.5 mmHg (−1.4 to −2.2) (all p < 0.001); this decrease was greater for participants with higher BP (p < 0.0001 each). No significant variation in HR was noted.
Conclusion:
Among a very large cohort, we observed a significant decrease in home BP measured with e-health devices during the first lockdown period. This study emphasizes the research potential of e-health during the COVID-19 crisis.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic that emerged in China in late 2019 rapidly spread around the world, affecting >70,000,000 patients globally. 1 To reduce the risk of person-to-person transmission and to combat the disease's wide dissemination, many countries have imposed one or more lockdown periods. Several reports highlighted a 20–30% decrease in the incidence of acute cardiovascular diseases, mainly non-ST segment elevation acute myocardial infarction (AMI) during—and a possible rebound after—the lockdown period. 2 –4 In contrast of this large body of evidence, very little is known about blood pressure (BP) and other chronic cardiovascular diseases and/or risk factors.
The application of big data analysis in medicine has opened up new frontiers, such as the development of predictive models and personalized medicine, and population-level health analyses. 5 Given the promotion of home BP monitoring over the past several years, many people are now equipped with wireless monitors, enabling the generation of very large databases.
To address the issue of BP trends during the pandemic and associated lockdown period, we analyzed big data registries from users of connected home BP monitors, and compared BP and heart rate (HR) measurements obtained during the lockdown period with data obtained immediately before the lockdown, as well as with data obtained from the same period in 2019.
Methods
All adults living in the Paris region with an ambulatory “Withings” BP monitor, having at least one available BP measurement recorded in the three studied time periods—namely, during the COVID-19 lockdown period (from March 17 to May 11, 2020), before the lockdown, and in 2019—were included in the analysis. Measurements were obtained and automatically transmitted after a complete deanonymization process and with participants' consent on a secured server.
To assess changes over time in systolic BP (SBP), diastolic BP (DBP), and HR, repeated measures linear mixed effect models were constructed, with time as fixed effect and patient as random effect. Models were also assessed by adjusting for age and gender as fixed effects. The adjusted means were calculated for each period, and the pairwise differences of adjusted means were compared using Tukey's post hoc t-test from the model.
According to French law, as we only had access to anonymized data, no formal institutional review board (IRB) approval was needed.
Results
From January 1, 2019, to May 5, 2020, 297,089 BP recordings were available from 2,273 participants. Most participants were <60 years old (58.5%, mean age was 56.3 ± 12.8, range 19 to 95), with the majority being male (81.1%). The number of BP measurements performed before and after the lockdown was 1.5 per week (0.7–3.9) and 1.6 per week (0.7–4.3), respectively.
SBP and DBP both significantly declined during the lockdown period. SBP gradually decreased during the first 4 weeks of confinement, reaching a 3-mmHg decrease plateau (range = −2.4 to -3.9 mmHg decreased from weeks 4 to 7, all p < 0.001; Fig. 1 and Table 1). A similar pattern was also observed for DBP, with a gradual decrease up to week 4 of lockdown, and a plateau of decrease of ∼1.5 mmHg (range = −1.35 to −2.22 mmHg decrease from weeks 4 to 7, all p < 0.001; Fig. 1). Similar results were observed when considering age and gender. In contrast, changes in HR were limited to a < 1 bpm, nonsignificant decrease (Fig. 1).
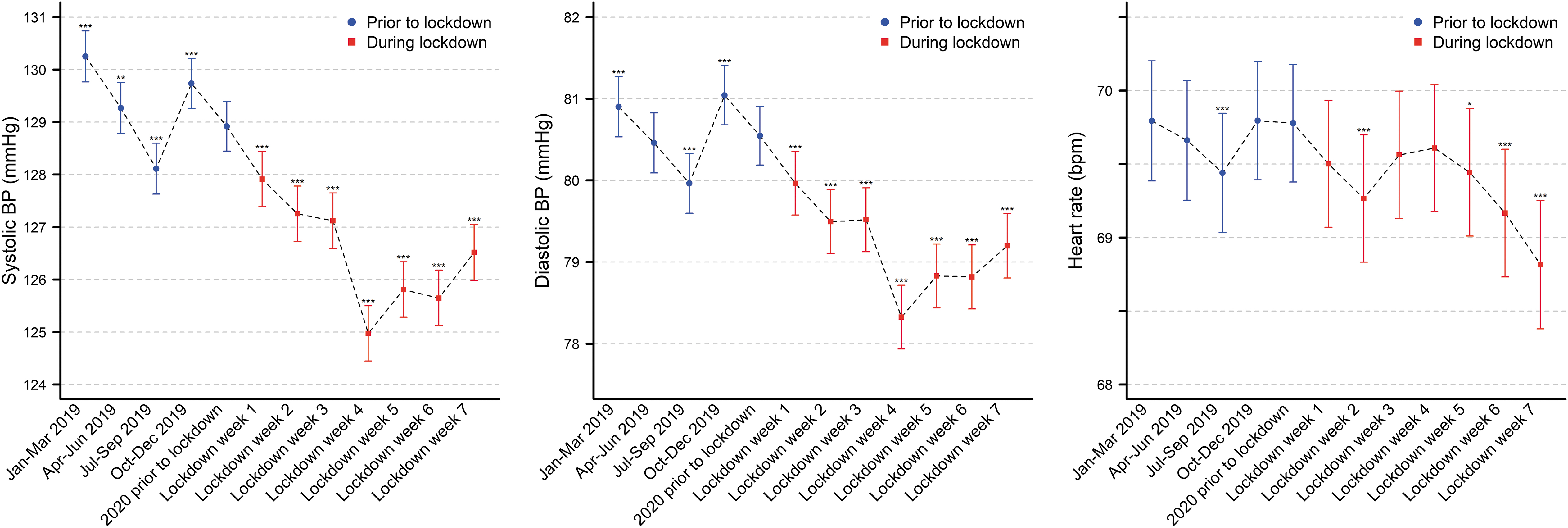
Changes in systolic and diastolic blood pressure and heart rate before and during the COVID-19 lockdown in France. COVID-19, coronavirus disease 2019.
Changes in Systolic and Diastolic Blood Pressure Prior and During the Country Lockdown
BP, blood pressure; CI, confidence interval; SE, standard error.
The main driver of BP changes during the lockdown was the BP level before the lockdown. Participants with higher SBP had higher decrease in SBP during the lockdown (beta for each 10 mmHg increase in SBP before the lockdown = −1.91 ± 0.12, p < 0.0001), whereas age and gender had no significant effect (p = 0.9 and 0.054, respectively). Similarly, participants with higher DBP had higher decreases in DBP during the lockdown (Beta for each 10 mmHg increase in DBP before lock down = -1.43 ± 0.12, p < 0.0001), whereas gender had no significant effect (p = 0.15).
Discussion
Our study shows that participants experienced a 3-mmHg SBP decrease and a 1.5-mmHg DBP decrease (which was not accompanied by an HR reduction) during the lockdown related to the COVID-19 crisis.
Several behavioral changes have been observed during the COVID-19 pandemic and associated lockdown. Most of these were expected to adversely impact BP, for example, sedentary lifestyles leading to increased food and alcohol intake, and, in turn, increased weight, and greater psychological tensions.
6
Some patients may have also stopped taking their medicine in the early phase of the pandemic due to preliminary warnings about a possible interaction between angiotensin converting enzyme inhibitors and the COVID-19 outcome.
7
A recent survey presented during the Argentine Congress of Cardiology indicated there were fewer emergency department (ED) admissions during the lockdown period compared with the period just before the isolation, but there was a greater proportion of patients having hypertension as defined by a SBP ≥160 mmHg and/or a DBP ≥100 mmHg (
In contrast, we studied a very large population, and all measurements were homemade. In addition, the BP reduction we observed occurred <1 month after the onset of the lockdown and was of a higher magnitude when compared with the minimal BP changes observed during the beginning of the pandemic, suggesting a direct link between the lockdown and BP reduction. The exact link cannot be derived from our study. Nonetheless, it is very unlikely that many therapeutic changes were performed during that period. In addition, we report a greater BP reduction among people having the most elevated BP before this time. We, therefore, hypothesize a decreased occupational stress level and increased treatment compliance during the lockdown, thereby resulting in greater BP control. 8
France was one of the countries most affected by COVID-19 in Europe. The French government decreed a period of confinement from March 17 to May 11, 2020. During this period, a decrease in hospitalizations for AMI was reported. 3 This study particularly focused on participants living in the Paris urban region, which was massively impacted by the COVID-19 epidemic and in which the lockdown was strictly enforced, resulting in a sudden and prolonged cessation of nonessential activities. Whether our results of decreased BP may account for part of the observed trends in AMI during the lockdown remains to be established.
LIMITATIONS
Some limitations deserve consideration. First, our analysis is limited by our inability to collect clinical data about medical diseases and treatments. As we studied all persons equipped with a wireless BP monitor, and because its use has been endorsed by national guidelines and advocated by physicians, our population should mostly correspond to hypertensive patients. The observed greater reduction in patients with higher BP before the lockdown may confirm our hypothesis. Second, we cannot comment on the possible clinical relevance and the possible link to the observed AMI reduction—a 3/1.5 mmHg BP reduction in our population—although a similar BP reduction was associated with reduced stroke and AMI in the valsateran antihypertensive long-term use evaluation (VALUE) trial. 9
Conclusion
This study demonstrates a progressive decrease in SBP and DBP during the lockdown. Whether this could partly explain the concomitant reduction in the incidence of acute cardiovascular diseases remains to be studied.
Footnotes
Authors' Contributions
N.G. was responsible for data analysis, writing, and revision of the article. C.M. carried out data analysis, writing, and revision of the article. K.D. performed statistics. V.V. performed data transfer. M.L.-S. carried out writing and revision of the article. J.-J.M. was responsible for conception, data analysis, writing, and revision of the article.
Disclosure Statement
V.V. is employed by Withings; however, he was neither involved in the data analysis nor in the decision to publish the results.
Funding Information
No funding was received for this article.