
Abstract
Background:
Case management (CM) is an intervention adapted to the needs of patients with chronic conditions or complex needs. Factors associated with effectiveness of CM, such as high intervention intensity, can represent challenges to its implementation. Telehealth has the potential to help overcome these challenges, but little work has been done to synthesize available evidence on telehealth CM. The purpose of this scoping review was thus to fill this gap and document which telehealth modalities have been used, summarize perspectives of key users, and discuss evidence on effectiveness of telehealth-delivered CM.
Methods:
A search in MEDLINE, Scopus, and CINAHL for articles published between January 2005 and January 2021 was done. Studies in which telehealth was used for patient-case manager interaction and conducted in a population with complex health needs and/or chronic conditions were included. Articles selected for full-text review were independently screened by two reviewers. Data extraction was conducted once and validated by a second reviewer.
Results:
Of 3,108 articles, 22 were retained for data extraction. A narrative synthesis was conducted. Most studies evaluated CM interventions delivered over telephone, yet, literature suggests that face-to-face contact is essential to CM success. Results also indicate that telehealth CM is acceptable and effective, associated with better utilization of health services and favorable clinical outcomes.
Conclusions:
Lack of research evaluating telehealth CM delivered using modalities other than telephone. Further research should evaluate CM interventions that integrate platforms enabling visual information exchange.
Introduction
With a progressively aging global population and the associated increase in the incidence of chronic diseases, health care systems around the world have to cope with the challenge of properly addressing the complex needs of these patients while still containing costs. 1 –3 Care models characterized by the integration and collaboration of multidisciplinary services, such as case management (CM), represent a strategy for improving the health of individuals with chronic conditions and/or complex needs. CM can be broadly defined as a complex intervention led by qualified case managers who identify patients with high needs or at risk for frequent health care use and comprehensively assess their needs to develop individualized care plans, and coordinate care across diverse health and social domains. 4
CM is recognized as an effective intervention for patients with chronic conditions and complex needs, having been associated with reduced health care use and costs, 5 –7 greater patient 8 and provider satisfaction, 9 and improved clinical 10 and functional outcomes. 11 –13 Factors such as continuity of care, intervention intensity, and effective communication have been identified as important elements of CM success. 14,15 However, achieving the latter represents a challenge to the implementation of CM programs, 16 and the enhanced intensity and communication must not offset the benefits of CM on reduced health care demand.
Telehealth may not only have the potential to absorb some of the increased demands on health care but also to specifically address some of the unique challenges of CM. Telehealth, the use of information and communications technology (ICT) to support health care delivery, has received substantial attention in recent years, in part, due to the booming field of technology, and also due to its potential to improve health care access. 17,18 The significance of telehealth was also highlighted recently when many institutions moved toward remote delivery of care in the context of the SARS-CoV-2 pandemic to prevent adverse effects of ruptures in care. Generally, evidence shows that telehealth may be equally effective compared to usual care in supporting the management of chronic conditions. 19,20 For CM practices specifically, telehealth may also favor the very factors that support its effectiveness (i.e., intensity and continuity) by enabling prompt information exchange between case managers and patients, or other providers. 21 –23
Given the theoretical complementarity of telehealth with CM, and its potential to improve the efficiency of health care delivery for individuals with chronic conditions or complex needs, developing CM interventions that use ICTs is primordial. Moreover, the field of health is increasingly moving toward the remote delivery of care, indicating a broader need for the development of care models that are adapted to telehealth technologies. 24 Although studies have evaluated the efficacy of telehealth-delivered CM programs, to our knowledge, no comprehensive literature review has been conducted on the subject. To fill this gap, this scoping review was conducted with the objective of describing existing knowledge on telehealth CM interventions delivered to patients with frequent chronic conditions or complex needs. 15
Methods
To conduct this scoping review, we used the five-step method described by Arksey and O'Malley 25 and updated by Levac et al. 26 The procedure undertaken is reported in the sections below using PRISMA Extension for Scoping Reviews (PRISMA-ScR) standards as guideline. 27
The main research question addressed by this scoping review is the following: What is known about the delivery of CM interventions using telehealth for patients living with frequent chronic conditions and/or with complex needs? More specifically, we sought to (i) identify which telehealth modalities have been used; (ii) explore the perspectives of patients and providers with regard to the use of telehealth, including any challenges regarding its implementation; and (iii) describe evidence on the effectiveness of telehealth-delivered CM.
DATA SOURCES AND SEARCHES
The search strategy was developed in collaboration with a librarian. Key words related to the two concepts of this review, telehealth, and CM were identified by reviewing relevant articles, their references, and related key words. Details on the electronic search strategy can be found in Appendix A1.
MEDLINE, Scopus, and CINAHL were searched for articles written in English or French, limiting the search to the last 15 years (January 1, 2005 to January 24, 2021), given that technology is a rapidly evolving field. Moreover, the early 2000s correspond to the advent of smartphones and increased accessibility to mobile technologies, which have reshaped the way the general population uses and understands technology. 28 References of articles identified in the database search were reviewed to identify other potentially relevant articles (hand searching). Moreover, if a record consisted of a conference article or abstract only, authors were contacted to identify related full-text articles.
STUDY SELECTION
Eligibility criteria
Articles were included if they fulfilled the following inclusion criteria: (i) evaluated empirically a CM intervention that includes the following three components 4,29 : assessment, planning, and coordination of care; (ii) used telehealth to facilitate a synchronous interaction between the patient and provider of the CM intervention; and (iii) included a population of adult patients (older than 18 years of age) with complex needs, including those with multimorbidity or frequent health care use, or with at least one frequent chronic condition (hypertension; osteoarthritis; mood and/or anxiety disorders; osteoporosis; diabetes; asthma; chronic obstructive pulmonary disease; ischemic heart disease; and cancer). 30
For the purpose of this review, telehealth was defined as the use of any informations and communications technology (e.g., telephone, web-application, video call), which allows a direct, synchronous interaction between patient and provider. 31 Studies were excluded if telehealth was solely used for (i) physiological monitoring, (ii) medical records, (iii) interaction between health professionals, (iv) for diagnostic purposes, or (v) as a store forward communication medium. Studies conducted exclusively within a pediatric population were excluded, as well as studies in which the CM intervention was delivered in the context of acute or postdischarge care, because this type of CM may differ significantly from the one delivered in a more longitudinal manner.
Selection process
First, one member of the team reviewed the titles and abstracts of the identified articles to exclude records that were clearly ineligible. Full texts of remaining records were reviewed and evaluated independently by two team members (S.B. and C.H.). In case of disagreement, the decision to retain or exclude the article was made by collectively reviewing each eligibility criterion, and by clarifying information, as needed, in supplementary materials provided.
DATA EXTRACTION
Before evaluating full texts, relevant data categories were identified and agreed upon by members of the team, and a standardized data extraction form was created. The data extraction process was nevertheless iterative, such that after using this extraction form for a first set of articles, the latter was modified to refine the choice of categories. Ultimately, data from the following general categories were extracted by a first reviewer (S.B.) and validated by a second team member (O.D.-S.): source information; study design and objective; sample description; intervention(s) studied; telehealth modality; CM activities conducted using telehealth; telehealth use frequency; main study outcomes; and stated challenges/facilitators to intervention implementation. A complete list of data categories and their definitions can be found in Appendix A2.
DATA SYNTHESIS
Synthesis of the extracted data was conducted using a narrative synthesis approach as described by Popay et al. 32 The synthesis process was conducted by grouping the extracted data into key themes including factors related to (i) experiences of users, barriers and facilitators, and (ii) main indicators of intervention effectiveness.
Results
SELECTION OF SOURCES OF EVIDENCE
The database search yielded 3,108 records. Five additional records were identified through hand searching, of which two were identified by contacting two authors of the seven conference abstracts identified in our database search. After removing duplicates, a total of 2,504 articles were screened for eligibility. Screening of titles and abstracts yielded a list of 131 full texts, from which 22 articles were selected to include in this review. Figure 1 details the study selection process. 27 Descriptions of each included study and main findings are presented in Table 1.
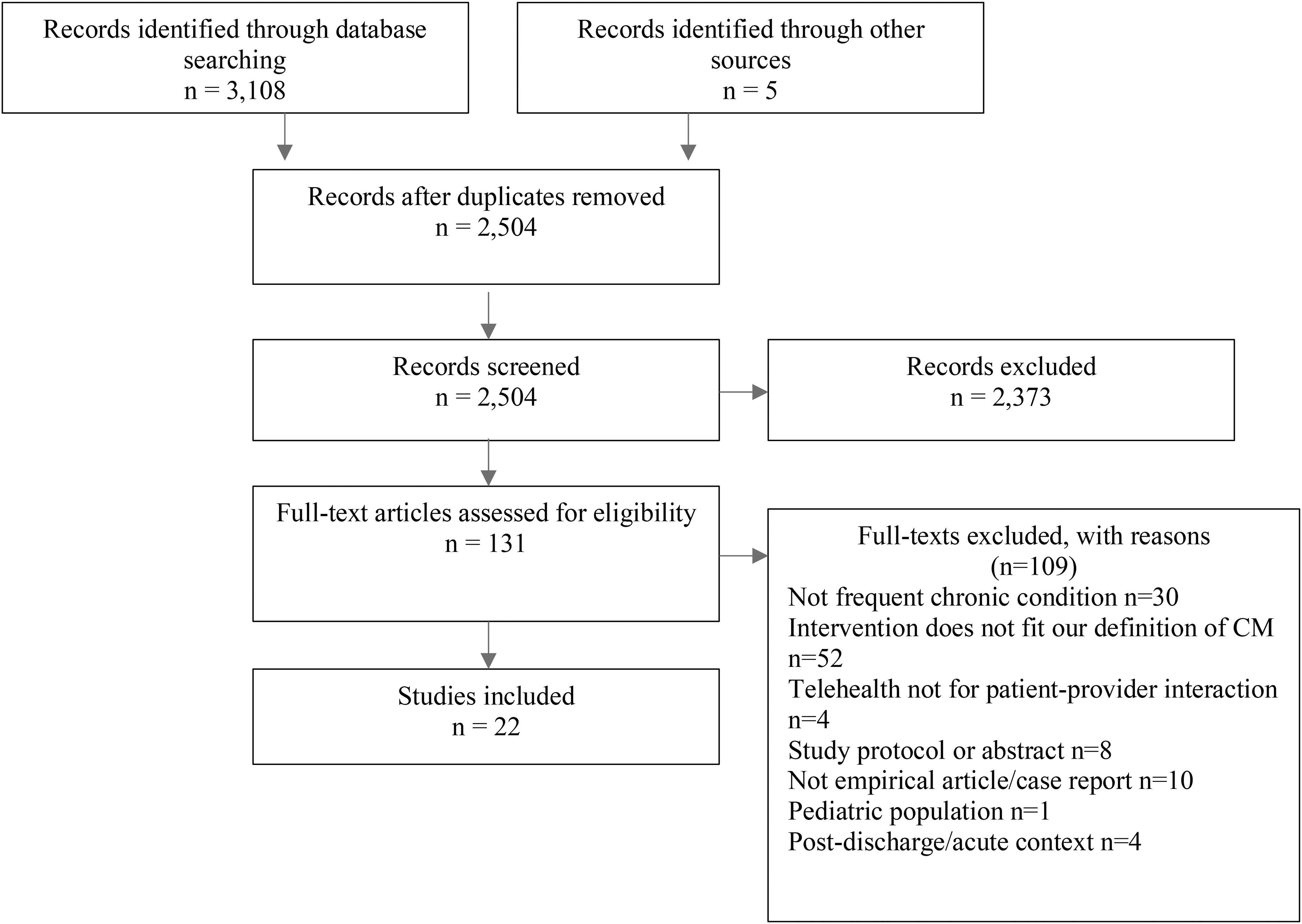
Flowchart of search results for the scoping review.
Description and Summary of the Main Findings of Included Studies Relating to the Use of Telehealth for Case Management
Older adults refers to participants over 65 years old.
Telephone-based CM refers to an intervention delivered entirely by phone as interpreted from article.
The use of the terms “decreases” or “increases” in a particular outcome refers to the group receiving the telehealth CM intervention, unless otherwise specified.
CM with telephone follow-up refers to an intervention which includes mostly telephone follow-up, with some in-person visits.
C, control; CM, case management; ED, emergency department; I, intervention; ICT, information and communications technology; ICU, intensive care unit; RCT, randomized controlled trial; ZD, zelen design.
CHARACTERISTICS OF SOURCES OF EVIDENCE
A majority of studies were published after 2010 (n = 17) and most were conducted in the United States (n = 15). Other countries include Sweden (n = 3), Spain (n = 2), United Kingdom (n = 1), and Germany (n = 1). Half of the studies (n = 11) were randomized controlled trials (RCTs), eight had a pre–post design with or without comparison groups, and three were qualitative studies. Ten studies compared a telephonic CM intervention to usual care or a passive control.
Most studies (n = 14) reported data for participants with a mean age or age range >60 years old. Eight studies included samples with an average age range of no <38. Most studies (n = 15) included samples representing individuals with complex needs, such as patients with multimorbidity, 39,48 frail older adults, 21,33,36 or identified as “high-risk” or “frequent users” based on predetermined criteria of health care use or health status. 8,35,37,38,42,45,47,49,50,52 Five studies included a sample with specific chronic conditions, including cancer, 51 diabetes, 34,40 and anxious and/or affective disorders. 44,46 One study focused on a sample of individuals with sickness-related long-term work absence. 41 Finally, one study included injured and newly in-processing Army Veterans, with some experiencing behavioral health problems and/or traumatic brain injury. 43
INTERVENTIONS
Thirteen studies included interventions that were provided entirely remotely using telehealth, 8,34,35,37,40 –44,46,47,49,51 while nine studies investigated a CM intervention, which included predominantly remote follow-up using telehealth, but where in-person visits were also mentioned. 21,33,36,38,39,45,48,50,52
Telehealth modalities used included mainly the telephone (n = 17), followed by tablet computers (n = 3), specially designed telehealth units (n = 3), and one mobile application (n = 1). In 18 studies, only 1 modality was investigated, while 4 studies used a combination of 2 of the latter telehealth modalities. 34,37,43,49
Only six studies specifically measured and reported the frequency of contact using telehealth. 8,37,44 –46,50 Nine studies described the planned frequency of contact, but did not report it as a measured outcome. 21,38,41 –43,47 –49,52 Seven studies did not mention contact frequency. 33 –36,39,40,51 From the available data, frequency of contact ranged between at least once a day 43 to minimally once every 3 months. 42 By contrast, the duration of the intervention was reported by all authors and ranged between 2 months 52 and 3 years. 36
Finally, CM interventions were either provided by United States health maintenance organizations (n = 8), 38 –40,42,45,47,50,52 United States Army Veteran programs (n = 3), 34,37,43 by the research team itself in a primary care setting (n = 2), 44,46 by a primary care team or in a community-based setting (n = 7), 8,21,33,35,36,48,49 or as part of an employer-based, occupational health program (n = 1) 41 or cancer support program (n = 1). 51
USER EXPERIENCE, CHALLENGES, AND FACILITATORS
Only seven studies reported outcomes related to the experiences of intervention participants. 8,21,33,37,40,41,43 In terms of advantages, aspects of practicality and accessibility were often addressed, 33,36,46 such as the ability to reach a larger number of patients, including those with mobility issues or that are geographically dispersed. 21,44,46 Several studies also noted that providing CM through remote technologies could promote a more “seamless” and continuous relationship with the case manager, 21,38,40 including the ability to keep in touch even during holidays or hospital stays. 21 Older adults noted that having videocalls with their CM could help reduce social isolation. 33 Moreover, the same participants felt a “sense of security” knowing that they could easily contact their case manager. Several researchers and research participants alike also noted the efficiency of telehealth, emphasizing the ability to quickly fix or address minor issues without the need for a clinic visit. 34,36,37,40,48 Other highlighted advantages of telehealth were modality specific. In relationship to tablet computers, older adults receiving CM through videocalls appreciated the possibility of having face-to-face contacts, which the authors concluded could facilitate the creation of a bond with case managers. 21,33,37
Nevertheless, some common challenges were noted. The most commonly cited one pertained to technical issues when using a telehealth device, 33,36,37,43 which was an issue specific to telehealth modalities other than a telephone. For example, for patients receiving CM through videocalls, internet connectivity was often an issue. 21,37 Moreover, frail older adults mentioned lacking “know-how” as an obstacle for using tablets, and the need to have a support network to learn how to use it, 33 while Duke 36 reported that those with certain conditions like Alzheimer's found using a telehealth unit particularly difficult to learn. Having access to these technologies also represents a barrier, particularly for individuals experiencing homelessness or financial difficulties. 40 Finally, in patients receiving a mobile app-supported CM intervention, participants criticized the repetitiveness and amount of information received using this medium. To exemplify this, Little et al. 43 noted that participants who received a mobile-app intervention, which involved receiving daily questionnaires, were significantly less likely to complete a follow-up assessment as part of the RCT.
INTERVENTION EFFECTIVENESS
Health care cost
Seven studies, including three RCTs and four pre–post studies investigated the cost-effectiveness of telehealth CM. Six of them indicated potential savings in health care expenditure. The remaining study only found a reduction in overall health care costs with a telephone-based CM in the later years of program implementation, which the authors attributed to program improvements. 35
Health care use
Thirteen studies 8,35,36,38,42,45 –52 reported results related to health care use, including number of hospitalizations (n = 10 8,35,36,42,45,47 –50,52 ), length of inpatient/hospital stay (n = 5 8,36,48,50,52 ), hospice use (n = 151), hospital-at-home unit use (n = 148); outpatient visits (n = 5 8,35,42,47,49 ); or emergency department (ED) visits (n = 9 35,36,42,46 –50,52 ). Outcomes revealed a general trend toward reduced use of costly care and increased use of outpatient or primary care services with the use of telehealth-delivered CM. Indeed, in 8 of the 13 studies mentioned above, reductions in the use of costly care were noted, such as reduced number of hospitalizations, 35,36,45,47,48,52 shorter hospital length of stay, 8,36,48,52 and decreased number of ED visits, 36,46,48 when comparing outcomes to a passive control group 8,35,45 –47,52 or to preintervention data. 36,48 By contrast, of the five studies reporting number of outpatient visits, four reported an increased use of these services by patients receiving telephonic CM compared to a control group. 35,42,47,49
Four studies deviated from these trends. In two cases, null findings could be attributed to small sample sizes 50 or unequal baseline characteristics of study groups. 49 In another study, Kim et al. 42 replicated results of decreased hospitalization or ED use only when focusing on a “high-needs” subsample.
Clinical and functional outcomes
Three studies reported clinical outcomes that were disease specific. In a retrospective cohort study of predominantly male United States Veterans with diabetes, 34 a telephonic CM intervention led to similar improvements in glycemic control when compared to a CM intervention where the same information was provided automatically by a telehealth monitoring device. Two RCTs 44,46 similarly showed that a telephonic CM intervention was associated with improved mental health functioning and reduced anxiety and depression symptom severity in individuals with anxious or affective disorders, when compared to usual care 46 or symptom monitoring alone. 44
Six studies measured self-reported health, quality of life (QoL), or well-being. Four studies reported improvements in the latter. In the same RCT discussed above, Rollman et al. 46 showed that telephone-based CM led to greater improvements in mental health-related QoL compared to usual care in middle-aged adults with anxiety/affective disorders. Relatedly, two different RCTs 8,49 showed that in similar samples of older adults qualified as “high-risk” or frequent ED users, a telephone-based CM intervention improved self-reported QoL.
Finally, four RCTs specifically reported quantitative outcomes in relationship to patient's satisfaction with telehealth-delivered CM and in all cases, most participants (over 70% of participants) reported being satisfied with telephonic CM 8,41,43 or mobile app-facilitated CM. 43
Discussion
In line with the present reviews' objectives, overall trends were identified among studies evaluating telehealth CM. First, most of the included studies focused on telephonic CM. Furthermore, studies evaluating patient perspectives highlighted the appreciation for the face-to-face contacts of video calls, and the accessibility and continuity of care afforded by telehealth. Studies generally showed decreased health care costs and positive patient outcomes with the implementation of telehealth-delivered CM, corroborating research on standard CM outcomes. 6,53,54
One potential drawback of a telephone-only modality is the lack of face-to-face contact. Two qualitative studies evaluating the use of videocalls for CM indicated that patients especially appreciated the ability to have face-to-face interaction with their case manager, which could facilitate the creation of a bond. 21,33 This finding was corroborated in a pilot RCT, where nurse case managers noted how video interaction provided improved patient engagement and communication. 37 The building of a trusting relationship between case manager and patient is an important element of CM, 14,55 –57 and the potential to have face-to-face communication has indeed been identified as a determinant of positive clinical outcomes among patients with chronic conditions receiving CM. 58 Video interactions may also facilitate other aspects of case managers' work such as conducting remote physical assessments or evaluating a patients' living environment, thus facilitating the implementation and efficacy of CM. 36,37
One potential mechanism for the decreased cost associated with telehealth CM is the better utilization of resources. In support of this, a general trend toward decreased costly care such as hospitalizations, but increased outpatient visits, were noted. This suggests that rather than culminating in emergency care-seeking or hospitalization, telehealth CM may allow for more appropriate responses to deteriorations in health status, through closer monitoring, care coordination, and referrals by case managers. Reductions in health care costs and use may also directly correspond to an overall reduction in the needs of patients receiving telehealth CM. In support of this, results of included studies pointed toward more positive clinical and functional outcomes in patients with chronic conditions or complex needs receiving telehealth CM, such as reduced psychiatric symptom severity, better glycemic control, and improved QoL. 8,34,44,46,49
One telehealth-specific mediator of reduced health care costs and use is that it allows prompt information exchange between case managers and patients, which was noted by many authors as a benefit of telehealth CM. Telehealth may indeed allow case managers to become aware of and address changes in health status in a timelier manner, preventing deteriorations in disease states. In addition, having the opportunity to handle minor health issues over the phone or through videocalls could prevent more costly in-person visits. 34,36,40,48 Communication with patients outside of clinic visits may also facilitate the longitudinal monitoring of patient needs. 21 By facilitating continuous care, remote delivery of CM using telehealth can reduce the “rupture” in the intervention that may occur in-between scheduled office visits, which may ultimately favor patient engagement in their treatment plan.
Enhanced psychosocial support could also mediate improved patient outcomes with telehealth CM. Psychosocial support has been shown to be an important element of CM success, 14 and telehealth may especially support this. Accordingly, improved feelings of support were frequently reported as a benefit of telehealth-CM in the included studies. 21,38,40 Feeling that one can easily contact their case manager through telehealth may foster a sense of security and reduce feelings of loneliness. Moreover, the improved ability to keep in touch with case managers may increase patients' proximity with them, also facilitating the development of a bond. Ultimately, enhanced feelings of psychosocial support could promote better disease self-management and treatment adherence and thereby improve clinical outcomes, a link which has been shown in previous work. 59 –62
Different populations may not equally benefit from telehealth CM. Indeed, quantitative outcomes of telehealth CM occasionally differed according to patient profile. 42,45 Patients with specific impairments like cognitive difficulties, 36,37 or frailty and disability, 33 may find it difficult to learn how to use telehealth devices or physically operate them, respectively. Indeed, in a sample of older medically complex individuals with suspected cognitive impairment receiving video-based CM, only about a third considered continuing to receive CM in this form, highlighting the need to identify, and address, barriers to the use of telehealth in these individuals. 37 Individuals with financial barriers may have difficulty accessing ICTs. Finally, individuals in situations of homelessness may be difficult to reach using means other than in-person visits. 40 These examples suggest the need to adapt the modality of CM to the preferences, resources, and abilities of individual patients.
FUTURE DIRECTIONS
Future studies evaluating telehealth modalities other than telephone to provide CM are needed. Specifically, modalities that offer the ability to communicate remotely while retaining face-to-face contacts should be further tested. In addition, further qualitative studies exploring the perspectives of health professionals and patients should be pursued, as this could further promote the evaluation of telehealth CM's feasibility.
Dosage is an important determinant of CM intervention success, 58,63 –65 but the frequency of telehealth contact was rarely reported. Moreover, the specific CM activities provided through telehealth and their proportion to those in-person activities were not always clearly defined. Future studies should thus specifically monitor and report these.
LIMITATIONS
CM is a complex intervention that is difficult to define and the CM definition used in the review's eligibility criteria may have excluded certain studies that may nonetheless reflect CM. In addition, interventions that correspond to CM are not always identified as such in the literature. Hence, it is likely that our search was not able to identify all articles that include both a CM and telehealth component. Second, although most studies were conducted in the United States, countries of origin varied in this review. It is plausible that the intricacies of the health care systems in place in specific countries may modulate outcomes. Finally, given that this is a scoping review, the articles included were not critically appraised and each included study had equal weight in guiding our interpretation of the literature. Accordingly, a systematic review design should be conducted to get a more accurate portrayal of the effectiveness of telehealth CM interventions.
Conclusions
This scoping review highlighted the dearth of research evaluating telehealth CM delivered using modalities other than telephone. The development of innovative CM interventions that integrate other ICTs, notably virtual platforms that enable exchange of visual information, represents an obvious next step, especially in the face of increased demand for and pertinence of remote delivery of care. This review also demonstrated that delivering CM interventions remotely using telehealth is generally effective and acceptable. Opportunities for improvements should be further evaluated in qualitative research that explore the perspectives of key players, including patients, case managers, and health care administrators.
Footnotes
Authors' Contributions
All authors fulfilled the criteria for authorship. S.B. wrote the original article. C.H. and O.S.-D. reviewed the article and contributed to the process of screening, review, and data extraction of included articles in this review.
Acknowledgments
The authors thank Mireille Lambert (Université de Sherbrooke) for her help in reviewing the drafted article. Moreover, S.B. thanks the Société des Médecins and Faculté de Médecine et des Sciences de la Santé of Université de Sherbrooke for their financial support.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported by the Canadian Institutes of Health Research-Operating Grant: Strategy for Patient-Oriented Research - Primary and Integrated Health Care Innovations (SPOR PIHCI) Network: Programmatic Grants (grant number 397896). This funding body was not involved in the design, conduct, and reporting of the review.
Supplementary Material
Supplementary Table S1
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.