
Abstract
Purpose:
To determine the magnitude, determinants, and public health issues related to diabetic retinopathy (DR) in India using 2019 data from a for-profit telescreening program.
Methods:
Digital retinal images were captured using a nonmydriatic fundus camera and transferred via the telescreening program to a reading center. Ophthalmologists trained in DR image reading created the DR status reports. Age/sex-adjusted rates of DR, sight-threatening DR (STDR), and diabetic macular edema (DME) were calculated and correlated with known risk factors.
Results:
Images of 51,760 Indian diabetic patients (103,520 eyes) were reviewed. The prevalence of DR, STDR, and DME was 19.1% (95% confidence interval [CI]: 18.9–19.5), 5.1% (95% CI: 4.9–5.3), and 3.9% (95% CI: 3.7–4.1), respectively. Based on these data, we projected 14.7 million cases of DR, 3.9 million with STDR, and 3.0 million DME cases in India. Statistically significant risk factors for DR were male gender (odds ratio [OR] = 1.19, p < 0.001), older age (χ2 = 270, df = 3, p < 0.001), history of cataract surgery (OR = 2.0, p < 0.001), longer duration of diabetes (χ2 = 1084, p < 0.001), and type 1 diabetes (OR = 3.9, p = 0.01). There was a statistically significant variation of DR by geographic zones (χ2 = 310, p < 0.001). Laser treatment coverage for STDR was 22%. Duration of diabetes (p < 0.001), cataract surgery in the past (p = 0.02), and females (p = 0.001) were predictors of STDR.
Conclusion:
This model of telescreening for DR provides an additional pathway for screening and preventing diabetes-related visual morbidity in India. The data from this study can be used for epidemiologic and ophthalmic health policies related to diabetes.
Introduction
The global rates of diabetic retinopathy (DR) and diabetic macular edema (DME) are 34.6% and 6.8%, respectively. 1 Vision-related functional defects are significantly greater among those with severe nonproliferative DR (NPDR) with DME and proliferative DR (PDR) than those without DR. 2
The prevalence of DR in India ranges from 15% to 20% 3 and is considered low compared with the global rate. However, the low prevalence can be attributed to the lack of a systematic approach for screening and management of diabetes mellitus (DM). There are several barriers to timely detection of DR, including the lack of trained retina specialists, a poorly educated diabetic population, and poor referral mechanisms to ophthalmologists. 4 In addition, the significant backlog of diabetic patients requiring retinal examinations is unlikely to be mitigated using conventional ophthalmic clinic/office visits. 5 –7
Visual morbidity in the Indian subcontinent can be significantly alleviated with early detection of DR and timely intervention through telescreening programs for DR. Studies of telescreening for DR in other countries have reported favorable outcomes. 8 –10 Detection of DR, progression, and the impact of treatment may be monitored using noninvasive retinal imaging techniques. 11,12 Nonmydriatic retinal photography and optical coherence tomography (OCT) are widely used, and, in conjunction with teleconsultation, these instruments have increased the ability to screen diabetic populations in remote areas. 7,13,14 In southern and western India, telescreening for DR has been implemented in local communities, government entities, and private hospital systems. 15 –17 However, public health programs that focus on national-level telescreening and managing DR remain in the early stages.
A novel initiative for DR screening is a fee-for-service teleophthalmology-based DR screening model that was initiated in 2014 by the Welcare Health System. 18 This service was provided to a large volume of patients in 20 Indian states and Union Territories. With a large diabetic population and limited retina specialists and screening resources in all parts of India, tele-DR screening initiative will be useful for early detection and timely management.
In this article, we review the characteristics of DR in a diabetic cohort that was screened with the Welcare Health System telescreening program for DR in 2019. Based on data analysis from this program, we present the magnitude of DR, risk factors of DR, and the effectiveness of managing sight-threatening DR (STDR) in India.
Methods
The Institutional Review Board of the King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia, approved this collaborative retrospective review in 2019 (1960-R). This study adhered to the guidelines of the Declaration of Helsinki. Two authors are related to Welcare Ltd. They provided the raw data from their database and facilitated data collection but had no influence on data analysis or interpretation. These two authors reviewed the final article and provided critical feedback for the Methods section as needed.
The study was conducted using data from Welcare Health Systems, India, in collaboration with the research group at King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia. Welcare Health Systems was started in 2014 in partnership with diabetes centers, general hospitals, government primary health centers, and family practice clinics throughout India. The company provides DR screening services through a different business model. In 2019, 250 medical centers were part of this network; however, none was an ophthalmic care center. The medical centers were staffed by a diabetologist/endocrinologist, internist, or family physician.
Diabetic patients included in this study were randomly selected from a database to represent six geographic zones in India. The study sample comprised 51,710 people with diabetes from a total of 300,000 screened in 2019. This random selection was done using random function of Microsoft XL® To maintain patient confidentiality and anonymity, personal and identifying data were delinked during data collection and analysis.
Physicians, diabetologists, and endocrinologists diagnosed diabetes based on HbA1C and a patient history of medications for glycemic control. 19 Systemic hypertension was defined as systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg recorded in the screening center or a patient's history of oral antihypertensive medications. 20
Each center was provided a nonmydriatic fundus camera (Trinetra classic fundus camera, Forus, Bengaluru, India) and Teleopia Customized Software for Teleophthalmology from Welcare Health Systems. The image capturing centers were located in urban and semiurban areas mainly attached to care centers affiliated to the Indian Diabetes Association or private hospitals. Diabetic patients undergoing annual assessment in these centers were residents of urban, semiurban, and, less often, from rural catchment areas. At each center, staff were trained on the use of the camera and software to upload demographic information, diabetes-related information, and posterior segment images. A single digital retinal image was obtained that included the macula centered and optic nerve head on one side with a total 40° field of view. Previous literature has reported acceptable sensitivity and specificity for automated DR screening. 21
The images were uploaded to the Welcare Cloud Based Software and forwarded to the teleophthalmology platform along with the medical history. The transfer was secure and encrypted. Images were permanently archived and accessible. The platform supports the most commonly used image formats, including Digital Imaging and Communications in Medicine. The images were reviewed and when needed filters were used for red free viewing.
Data were collected on patient demographics, the type and duration of diabetes (based on medical records, if not available then as reported by the patient), and ophthalmic history. Demographic information was collected on, age, gender, and the state in India where diabetes screening was performed. History taking specifically included whether the patient had undergone cataract surgery in the eye with more advanced DR and previous laser treatment for DR. The type of laser treatment was not documented for this study.
Ten ophthalmologists trained in telescreening and supervised by a senior fellowship-trained retina specialist interpreted the images for each eye and graded the stage of DR based on the International Classification of DR. 22 The graders (ophthalmologists) then generated reports that were transmitted to the referring center within 2–3 h after receiving the images. For quality control, the retina specialist randomly reviewed 10% of the reports. In cases with STDR, a medical retina specialist confirmed the diagnosis before a report was generated.
NPDR was graded as mild, moderate, and severe according to the Preferred Practice Pattern recommended by the American Academy of Ophthalmology and the guidelines for DR management in India. 23,24 The stage of DR was based on the eye with the more advanced disease. The status of macula was evaluated and the presence or absence of DME was noted. STDR was considered the presence of severe NPDR, PDR with or without DME. The patient was diagnosed with STDR if DME involved the central macula, with decreased vision in the eye with clear media and mild or moderate NPDR. DME was diagnosed based on nonstereoscopic images using cues such as the presence of hard exudates and microaneurysms in the macular area that were associated with visual impairment in the affected eye. 25 The image reader could make notes on the ophthalmic findings in a comments box in the software (Fig. 1).
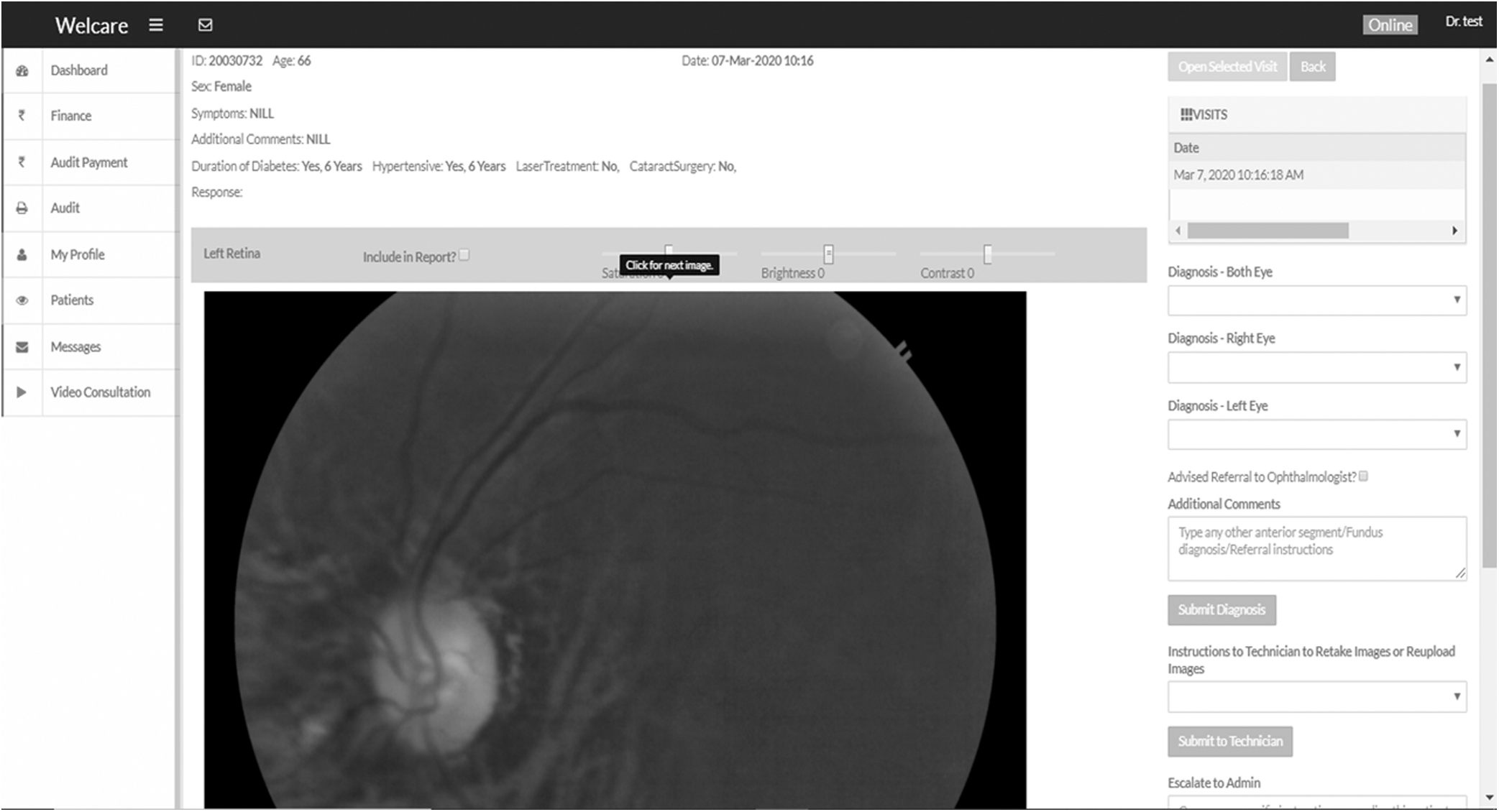
Picture of the reading center of Welcare System in India showing feedback information provided to the referring center.
The location of the clinic and the Indian state from which the images were uploaded were further divided into north, east, west, central, northeast, and south zones of India (Fig. 2).

Map of India showing states included in the six zones and the prevalence of DR and STDR. The map was drawn by an artist and provided by Welcare System. The prevalence and projected number of DR were added by the authors. DR, diabetic retinopathy; STDR, sight-threatening diabetic retinopathy.
For validation of DR image review carried out by our staff, all diabetic patients screened in Chennai were also examined by retina specialists and their findings were compared. The screening of 2,465 diabetic patients by a retina specialist revealed that the image reading with a sensitivity for detecting DR was 90.3% and specificity was 99.7%. For detecting STDR, the sensitivity was 95.7% and specificity was 98.8%. In 20 patients for whom images could not be interpreted, only 6 had media opacity not allowing retinal examination after dilation of pupil.
The data were provided on an Excel® spreadsheet (Microsoft Corp., Redmond, WA) from the telescreening program. Data were analyzed using Statistical Package for Social Sciences (SPSS 26; IBM Corp., Armonk, NY). The eye with the worse stage of DR was labeled and only this eye was included in the analysis. Univariate analysis was performed using parametric methods. The population projection for males and females in each Indian state and age groups for 2019–2020 were obtained from a population pyramid of India and by using data on the prevalence of diabetes from previous studies. The number of individuals with diabetes was estimated and matched with projections from the International Federation for Diabetes. 24,26 An Excel® spreadsheet was created for each of the six geographic zones (Supplementary Appendix SA1). People with diabetes were grouped according to age as follows: <20 years, 20 to 39 years, 40 to 59 years, and 60 years and older. The number of males and females was also calculated. The duration of diabetes was grouped as follows: <5 years, 5 to 10 years, 10 to 15 years, and more than 15 years. The referring physician or patient provided data on the duration of diabetes. Rates of DR, STDR, and DME were calculated as summarized in the next paragraph. 27
To calculate crude rates of DR, DME, and STDR by age and gender, data were stratified by age groups and gender (Supplementary Appendix SA1). We then used previously published population and DM prevalence data 24 to compute a projected estimate of different stages of DR, DME, and STDR among diabetic patients in India; that also allowed us to calculate the projected age/sex-adjusted prevalence rate and the 95% confidence interval (CI). 28
Odds ratio (OR), the 95% CI, and two-sided p values were calculated to assess the association between DR and risk factors. For variables with more than two subgroups (e.g., age groups), the chi-square value, degrees of freedom, and two-sided p values were calculated. For quantitative variables with skewed deviation, we estimated the median and interquartile range (IQR; 25%; 75%). A p-value <0.05 was considered statistically significant. The factors significantly associated with univariate analysis were put in binominal regression models and associated/correlated to the presence of DR and STDR. The adjusted OR (adj OR) and two-sided p values were estimated.
The proportion of patients with different stages of DR was also calculated and plotted. We also calculated the proportion of eyes that had STDR or DME and the proportion that received laser treatment (pan retinal photocoagulation or focal laser) in this study group. Patients who provided a history of laser treatment and/or had evidence of laser burns visible on retinal images were considered to have received laser therapy. We used these data to estimate the scope of laser treatment services available for STDR cases by the existing DR management services. We used the following formula to calculate this metric: number of persons with laser treatment in the past in either eye/persons with STDR × 100. 29
The need for resources such as lasers, intravitreal injections, and vitreoretinal surgeries for managing STDR cases was also calculated.
Results
The study sample comprised retinal images from 103,520 eyes of 51,760 Indian patients with diabetes. The mean age of study sample was 51.7 ± 11.9 years. There were 52 individuals with type 1 DM (T1DM), 25 with confirmed gestational diabetes, and the rest had type 2 DM (T2DM). The median duration of diabetes was 6 years (IQR 3; 10). Hypertension was present in 15,324 individuals (29.6%).
Table 1 presents the distribution of people with diabetes in different age groups, gender, and compares the distribution of people with diabetes participating in this study with that reported in the population with diabetes projected for India. The tele-DR screening group had a slightly greater number of people with diabetes in the “under 20-year age group” for both genders and in the “20- to 39-year age-group” of females. The number of people with diabetes from both genders in the “40- to 59-year age-group” was lower in the present study compared with the reported projections. Among individuals with T1DM, the median age was 35 years (IQR 22.3; 50) and the median duration of DM was 7 years (IQR 1.7; 14). The median age of those with T2DM was 50 years (IQR 42; 58) and the duration of diabetes was 5 years (IQR 2; 10). The age was significantly higher in individuals with T2DM than those with T1DM (Mann/Whitney [MW] p < 0.01), but the duration of diabetes was not significantly different for those with T1DM or T2DM (Mann/Whitney U p = 0.2).
Proportionate Representation of the Diabetic Population and Those Participating in Tele-Diabetic Retinopathy Screening
The distribution of diabetic population is based on the census population of India 20 and rate of DM in subgroups noted by Gadkari et al. 6
DM, diabetes mellitus.
The crude prevalence of DR was 9.6% among individuals with T1DM and 2.4% among those with T2DM. The prevalence of DR was statistically significantly higher in T1DM (OR = 3.9, p < 0.001). For patients with more than 5 years of diabetes, the prevalence of DR was 11.1% among individuals with T1DM and 26% among individuals with T2DM (p = 0.06).
The age/sex-adjusted prevalence of all stages of DR was 19.1% (N = 9,886) (95% CI: 18.9–19.5). Table 2 presents the prevalence of DR in subgroups according to gender, age groups, and zones in India. A greater number of patients were screened in the southern and western zones than in the other zones. The lowest numbers of patients were screened in the northeast zone. The prevalence of DR was statistically significantly higher in males compared with females (OR = 1.19, p < 0.001). There was a statistically significant increase in the risk of DR with increased age (χ 2 = 270, p < 0.001). The age/sex-adjusted prevalence of DR was significantly greater in the northern (19.4%), eastern (20.0%), and central (22.1%) zones compared with the northeast (15.7%), western (17.1%), and southern (18.7%) zones (χ 2 = 310, p < 0.001). A longer duration of diabetes was positively correlated with a higher prevalence of DR (χ 2 = 1,084, p < 0.001). The risk of DR was significantly higher in people with associated hypertension compared with those without hypertension (OR = 1.15, p < 0.001). Based on these data, it is projected that there could be 14.7 million people with DR among 77 million individuals with DM in India.
Prevalence of Diabetic Retinopathy (All Grades) Among Persons Who Underwent Telescreening for Diabetic Retinopathy in India
p < 0.05 is statistically significant.
χ 2 , chi-square value; CI, confidence interval; DF, degrees of freedom; DR, diabetic retinopathy; OR, odds ratio.
A history of cataract surgery in the eye with more advanced DR was noted in 4,353 (8.4%) participants. People with diabetes who had undergone cataract surgery had a higher rate of DR compared with diabetic patients who had not undergone cataract surgery (OR = 2.0, p < 0.001).
The binominal regression analysis suggested that age (adj OR = 1.003, p = 0.02), duration of diabetes (adj OR = 1.05, p < 0.001), gender (adj OR = 1.07, p = 0008), and no cataract surgery (adj OR = 0.84, p < 0.001) were associated with the presence of DR.
Figure 3 presents the proportion of the different stages of DR in these patients. STDR was noted in 243 (5.8%) of 4,353 patients with DR.

Proportion of different stages of DR in a population with diabetes based on the stage of DR in the worse eye.
Table 3 presents the prevalence of STDR among subgroups. There were 4,080 STDR cases among 51,760 individuals with diabetes. The prevalence of STDR was 5.1% (95% CI: 4.9–5.3). Based on these numbers, we project that there could be 4 million individuals with STDR among 77 million individuals with diabetes in India. The STDR rate was significantly higher in females compared with males (OR = 1.14, p < 0.001). The variation in STDR rate was not significantly different among age groups (χ 2 = 1, p = 0.8). The rate of STDR increased statistically significantly with a longer of duration of DM (χ 2 = 1,084, p < 0.001). The age/sex-adjusted prevalence of STDR was 7.7% in the northern zone, 11.6% in the eastern zone, and 3% in the western zone. A history of hypertension (OR = 2.2) and cataract surgeries (OR = 1.5) were both inversely associated with STDR rates. The prevalence of STDR was 4.5% in those with a history of laser treatment and 9.4% in those who had not undergone laser treatment (OR = 2.2, p < 0.01). The binominal regression analysis suggested that the duration of diabetes (p < 0.001), cataract surgery in the past (p = 0.02), and females (p = 0.001) were predictors of STDR.
Prevalence of Sight-Threatening Diabetic Retinopathy Among Persons Who Underwent Telescreening for Diabetic Retinopathy in India
p < 0.05 is statistically significant.
DME, diabetic macular edema; NPDR, nonproliferative DR; PDR, proliferative DR; STDR, sight-threatening diabetic retinopathy.
The prevalence of DME (N = 3,889) was 3.9% (95% CI: 3.7–4.1). Based on this computation, it is projected that there could be 3 million cases with DME among the diabetic population in India.
There were 448 (0.9%) (132 with STDR +316 with NPDR at the time of examination) people with diabetes who had undergone laser treatment for DR. Of the 4,080 STDR cases, 682 (4.5%) cases had undergone previous laser treatment for DR. Thus, the coverage of laser treatment for STDR by the existing ophthalmic services in the study area was 682/4,080 × 100 = 16.7%.
Among 10 ophthalmologists who were the image readers (each had screened images from more than 500 patients), the reported STDR rate ranged from 1.9% to 5.9%. This variation in the STDR rate was marginally statistically significant (χ 2 = 9.7, DF = 9, p = 0.01). However, there was significant variation in the detection of DR by ophthalmologists (χ 2 = 113, DF = 9, p < 0.001).
In 3,767 (7.3%) diabetic patients, undilated posterior segment evaluation was not possible because of poor image quality likely resulting from media opacity, poor pupil dilation, or poor patient cooperation. Up to 578 (1.1%) individuals who screened for DR had hazy media bilaterally, limiting retinal examination.
Discussion
This unique data set of a large population screened through a private fee-for-service system provides an understanding of the magnitude of DR in India, and the association of DR with known risk factors. In addition, the data allow estimation of the burden of DR in India, which can be used for planning appropriate interventional services for the diabetic population.
Our analysis of a biased sample suggests that one in five diabetic patients who underwent telescreening had DR and two out of five DR patients had STDR. These rates are much higher than projections from the International Federation of Diabetes. 30 For example, the International Federation of Diabetes 30 reported one in six cases of DR among adult diabetic patients and one in three cases of STDR among those with DR. Based on these data, there could be 14.7 million cases of DR, 3.9 million cases of STDR, and 3 million DME cases in India. The national diabetes and national eye health care program in India could use these projections for allocation of health care resources. The present study confirmed previously described risk factors for DR such as male gender, older age, longer duration of diabetes, and a history of cataract surgery. 1,26 Regional variation in a large country such as India has been previously reported. 1,26 Several studies have documented the benefits of telescreening for DR. 31 –33 However, there are also some pitfalls in the telescreening initiative. In the current study, the prevalence of STDR and the low rate of intervention through existing eye care services are a public health concern. Screening efforts should include treatment planning once STDR is detected. 34,35 During DR telescreening, the referral source should be noted (e.g., local diabetes society, endocrinologist, and family physician). We recommend that for-profit DR screening initiatives should ensure a strong liaison with referring centers to support intervention of cases identified with STDR. Arguably, the rate of STDR in the entire diabetic population could be lower than that reported in this study.
In the present study, there was a 19.1% prevalence of DR among those older than 20 years. This rate is well within the range of 9.6% to 33.9% reported by a systematic review of DR in the adult T2DM population in the Indian subcontinent. 36 Studies of a T2DM population 40 years and older in an urban slum in Mumbai and of adult diabetic patients in an urban area reported DR prevalences of 15.4% and 21.7%, respectively. 37,38 The difference in the prevalence of DR between our study and previous studies could be due to the variation in sample size, age-related inclusion criteria, data from specific zones only, or the ratio of urban/rural populations. The prevalence of DR reported in our study was based on a large sample from 20/28 states in India. In this study, individuals were from diabetes care centers and thus could represent a population more aware of its health than diabetic patients who were not receiving care or were managed at general medical practices.
Of the 77 million projected patients with diabetes in India, we estimate that at least 15 million with DR would require annual DR screening, primary prevention of diabetes, and control risk factors for the progression of DR. Endocrinologists, family physicians, counselors, and patients with diabetes could use these projections as targets for primary prevention initiatives for DM and DR.
In any DR screening initiative, STDR cases indirectly reflect the reach of the existing eye care services for managing DR. The 5.1% prevalence of STDR in the current study is within the range of 3.8% 38 to 6.6% 37 reported by similar studies on an Indian cohort. The projections of 3.9 million STDR cases and 3 million DME cases in our study could enable to plan the resources for addressing the current backlog and meeting the future demand.
We found that the prevalence of diabetes and DR was significantly higher in males compared with females. T2DM and DR are more prevalent in males and occur at an earlier age. 39 In addition, we noted that 14% more males had STDR compared with females. However, this was less than the 50% higher risk in males than females noted in south India. 40 In contrast, Joseph et al. 41 noted that females with STDR faced barriers in seeking hospital-based services. Although not a novel finding, the higher rates of STDR in males noted in the present study warrant further investigation.
DR was more prevalent in the central, eastern, northern, and southern zones and less prevalent in the northeast and western zones of India. Geographic variation has also been reported in underprivileged areas in the United Kingdom. 42 Ethnicity may be an alternate explanation for the variation in the prevalence and severity of DR. 43 Perhaps variation in lifestyle, food habits, and access to health care services in some zones in India could further explain the regional differences in the prevalence of DM and DR.
The prevalence of DR in this study increased with age. This observation concurs with Solomon et al. 44 and Wang et al. 45 who have reported that older diabetic patients are at a higher risk of developing advanced DR. The duration of diabetes is a risk for DR and the progression of DR. We noted a strong association between DR and the duration of DM. This observation concurs with findings of previous studies where DM of more than a 15-year duration had a significantly higher risk compared with DM less than 5 years of duration. 1,46
In the current study, DR was more prevalent among T1DM patients than those with T2DM. However, the small sample of T1DM in our study precludes a definitive conclusion. Wang et al. 45 noted that eight years after detection of DM, DR developed in 10.3% of T1DM patients and 31.2% of T2DM patients who were between 10 to 20 years old. Thus, screening for DR in the Indian population should be performed within 5 years after onset in T1DM cases and annually for T2DM after detection. 23,47
In the current study, we found a statistically significant positive association between DR and a history of cataract surgery. However this association did not exist between STDR and previous cataract surgery. A higher risk of DR was documented in the era of intracapsular cataract surgeries. 48 However, the modern techniques of cataract extraction and intraocular lens implantation have reduced the risk of DR and its progression. 49 Peterson et al. 50 noted that cataract surgery poses a 50% additional risk of developing NPDR and progression of DR to STDR. There could be an alternate explanation of a positive association of DR with cataract surgery. After cataract surgery, the posterior segment visibility will be better, and hence, signs of mild-to-moderate non-PDR-like microaneurysms can be better seen after cataract surgeries, resulting in a high rate of DR in aphakic/peudophakic eyes.
In this study, less than 1 in 15 cases of STDR had a history of laser treatment (pan retinal photocoagulation and/or focal laser application). This was much higher than 2.7% reported in a study from Pune, India, and 5% reported in Fiji. 51,52 The relatively higher coverage of laser treatment in the present study may be be due to a larger proportion of affording patients in our for-profit payment model. However, several other factors might have contributed to the differences in laser coverage between studies, including the limited availability of laser treatment and extensive usage of low-cost intravitreal bevacizumab. 53 The screening/treatment discrepancy highlights the importance of public health planning for the management of STDR as a component of DR screening programs. 54
Detecting DR through tele-DR screening and suggesting a protocol for referral to a retina specialist to prevent sight-threatening complications of diabetes are also a focus of this research article. All diabetic patients with STDR in one eye must be referred to a retina specialist for urgent intervention. The feedback to the referring centers about the status of DR was then shared with the attending family physician and endocrinologist. This helped in stressing their role in patients' good glycemic control as well as in addressing the known risk factors of progression of DR. Their role in annual or more frequent DR screening was also a crucial part of protocol for tele-DR screening.
In the current study, labeling of STDR was relatively uniform among the image readers. Piyasena et al. 55 have reported on the variation in detection rates of DR among image graders. Hence, all the DR readers in this teleophthalmology DR screening system were periodically retrained and supervised. Since telescreening is the first level of screening for DR, efforts should be directed at improving the validity parameters of the screening test. 56
In 7% of our study population, the presence of bilateral media opacities (mainly cataracts) limited the use of telescreening for DR. A Greek study reported that 18.7% of images could not be interpreted due to poor image quality. 57 A study from south India reported that 32% of images could not be interpreted. 58 The low percentage of media opacities in our study compared with rates of cataract-related blindness 59 and telecreening 60 could be attributed to a population with better access to ophthalmic consultations for cataract and other media opacities. In countries with a high backlog of unoperated cataract, DR telescreening programs could face a high rate of image failure, reducing the efficacy of the initiative.
There are some inherent limitations to the analysis of data from DR telescreening programs. Information of the known risk factors such as glycemic control, obesity, nephropathy, and hyperlipidemia was not collected by the imaging centers in the present study. The validity of a health screening program is enhanced if more information on the independent risk factors is available to the screener. 61 In the current study, the diagnosis of DME was based on the interpretation of macular images and visual impairment but without confirmation by OCT. OCT is expensive and less feasible in the field and could be added as a second-level screening to enhance the validity of telescreening for DR. In the current study, information was missing for some patients on ocular comorbidities, DR-related surgeries, and intravitreal injections. The missing data could limit the usefulness of monitoring indicators of a screening program. As all the images were based on only one visit, the conversion rate of NPDR to STDR through sequential imaging of the same patient could not be studied.
Although the prevalence of DR in this study is low, the proportion of STDR is similar. A higher proportion of STDR in a population with lower prevalence of DR suggests late detection and insufficient management services. Introduction of imaging techniques is crucial as it can bypass general ophthalmologists in rural areas and allow patients with severe DR timely and direct access to a retina service. The cost of tele-DR screening was less than U.S. $ 2 to the diabetic patient. Most of the patients were either enrolled at the local diabetes associations or visiting large hospital for their annual diabetes checkup. If this screening is held by ophthalmologists in eye clincis, it will cost similar or more and expert retina specialist opinion would not have been available to all with similar consultation charges.
Although the prevalence of DR in this study is low, the proportion of STDR is similar. A higher proportion of STDR in a population with lower prevalence of DR suggests late detection and insufficient management services. Introduction of imaging techniques is crucial as it can bypass general ophthalmologists in rural areas and allow patients with severe DR timely and direct access to a retina service.
In summary, this study presents data from a large-scale model of a fee-for-service telescreening program for DR. In a country such as India with a population of 1.4 billion and with limited eye care services that are concentrated mainly in the urban areas, telescreening for DR by private companies involving ophthalmologists could be an effective, sustainable, and expandable strategy to provide screening services to people with diabetes both in urban and rural areas, and effectively detect early-stage DR. Such initiatives also provide epidemiological and public health information on this chronic noncommunicable disease. Scaling up of DR screening through payment could be useful in countries where insurance and nongovernmental agencies could cover the expenses. This initiative must be complemented by upgrading the resources to address treatment of the cases identified with STDR and increasing the awareness among all stakeholders to continue primary prevention, and regular follow-up of those at risk.
Key Messages
In a large country such as India, early detection of DR is a challenge and the nationwide tele-DR screening is in its early stages.
We share the review of tele-DR screening data-based prevalence, risk factors of DR, and sight-threatening stages of DR among persons with diabetes screened through a network of public/private partnership.
Such DR screening model could complement a national initiative of improving eye care of the diabetes population.
Footnotes
Authors' Contributions
R.K.: planning, data analysis, and article writing. T.S.: planning, data owner, and drafting article. M.N.: data manager, image reading, in-charge of article. D.P.E.: planning and finalization of article.
Acknowledgments
We thank the staff at the Research Department of King Khaled Eye Specialist Hospital and the ophthalmologists at Welcare System for supporting data assimilation. Dr. J. Fernando Arevalo and Dr. Taraprasad Das provided important inputs to improve the article.
Ethical Statement
Disclosure Statement
Dr. Senthil is the founder of Welcare Ltd that provides physician screening services. Dr. Nainappan was affiliated to the company as advisor and trainer. Drs. Senthil and Dr. Nainappan provided the raw data but had no influence on data analysis or data interpretation. Dr. Senthil reviewed the article and provided critical feedback.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.