
Abstract
Introduction:
Telemedicine for neurological care has been researched and practiced in various ways over the past three decades, but the recent COVID-19 pandemic has rapidly expanded its use and highlighted the need for a synthesis of the existing literature. We aimed to review the methodology and outcomes of previous studies that have evaluated the use of telemedicine in movement disorders.
Methods:
This scoping review was performed by searching PubMed, Ovid MEDLINE, and CINAHL databases from 1946 to November 2020. Studies that assessed the application of telemedicine for delivering care to patients with a movement disorder were included. We reported the aims and employed methodologies and categorized the outcomes from each study.
Results:
The search retrieved 228 articles, and 41 studies met the criteria for inclusion in the review. The majority of telemedicine studies were case series or randomized controlled pilot trials, investigating feasibility and acceptability in Parkinson's disease. Even with heterogeneity among outcome measures, they can be categorized into themes, such as feasibility, satisfaction, and efficacy.
Conclusions:
Telemedicine use has grown rapidly, due to the demands of providing care during a global pandemic. This application of telemedicine has been considered a promising way to expand care in Neurology, although research evaluating the dissemination of its use is dilatory. This review highlights the number of studies that have found telemedicine to be an acceptable and feasible way to deliver care for movement disorders. Further research is needed to expand on harmonization of outcomes, reach, adoption, and long-term use of telemedicine.
Introduction
Rationale
Telemedicine, defined here as the use of real-time, synchronous audiovisual technology to examine, monitor, and treat patients while the clinician is in a different physical location, is a promising method of providing neurological care and potentially leads to better patient outcomes. 1 –4 Telemedicine in neurology initially gained popularity for its use in stroke care, referred to as “telestroke” in an early editorial published in Stroke in 1999. 5 Since its inception, telestroke has become a critical component of stroke systems of care, promoting hub-and-spoke models that facilitate physician collaboration between a stroke center and area hospitals, expediting evaluation, and improving quality of care for patients who may require time-sensitive thrombolytic treatment. 6 While telestroke has become widely accepted in advanced stroke care, other subspecialties have not adopted telemedicine into their practice, perhaps due to inconclusive data from patients and providers on feasibility and acceptability, as well as lack of reimbursement, and lower patient acuity. 7
Telemedicine could be especially important in movement disorders, where a large proportion of patients experience limited mobility caused by disease progression, rely on visual assessments by movement disorder specialists, and may require multidisciplinary care. 4,8,9 The vast majority of published studies evaluating telemedicine use in movement disorders focus on its application in Parkinson's disease (PD) care. In the PD population, telemedicine has been shown as a useful tool to provide speech therapy, exercise programs, and follow-up care. 10 –16 In contrast, few studies have reported on telemedicine for other movement disorders, such as Huntington's disease (HD), essential tremor, drug-induced movement disorders, or Tics. 17
For individuals with a movement disorder, there are a number of barriers impacting access to health care, including travel distance, physical or cognitive impairment, an unequal distribution of neurologists, and a paucity of specialists relative to the population prevalence. 18,19 In the last year, health care providers and patients faced an additional unprecedented barrier, the COVID-19 pandemic. In a matter of weeks, neurologists were forced to transition from in-person visits with their patients to telemedicine. This abrupt shift in practice has highlighted the benefits and frustrations of using telemedicine, while also increasing users' experience with the technology. 20
With this hasty adoption of telemedicine, it is an important time to review and identify the aspects of telemedicine that have been deemed acceptable or feasible. Previous studies across neurology subspecialties indicate that visits conducted through telemedicine are noninferior to in-person visits, when comparing patient and clinician satisfaction, diagnostic accuracy, and improved outcomes. 7 However, limitations, such as study size, methodology, and heterogeneity of measuring outcomes, leave gaps in our understanding of telemedicine's full potential. The objective of this scoping review was to summarize the existing literature for real-time telemedicine contact between clinicians and patients with movement disorders, with a focus on the various study methodologies and reported outcomes.
Methods
Search Strategy
This extensive review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 21 Original research articles were identified by searching the PubMed (1946–November 2020), Ovid MEDLINE (1946–November 2020), and CINAHL (1976–November 2020) databases. The search strategy was developed with the assistance of a medical librarian (D.O.) and included terms for movement disorders and telemedicine. The complete search in PubMed was a combination of movement disorder-related Medical Subject Headings (MeSH), such as “essential tremor,” “Parkinson disease,” “Huntington disease,” and “drug induced movement disorder” along with the MeSH “Telemedicine” and other “tele-terms.” Tele-terms is a phrase used by our librarian to refer to the multiple synonyms found throughout the literature to describe remote health care technologies. After submitting the search terms into PubMed, the filters for Clinical Trial and Randomized Controlled Trial (RCT) were selected. A similar approach was used in the CINAHL database. The complete list of terms included in our PubMed and CINAHL search can be found in Appendix A1.
In Ovid MEDLINE, a four-step search was created by first entering the term “movement disorders” and selecting the subcategories, as well as “Parkinson disease” and “Huntington disease” on the mapping page. The next search for “telehealth” resulted in an output of “telemedicine” and subheadings “telepathology,” “teleradiology,” and “telerehabilitation,” all of which were selected. Both groups of search terms were combined with AND, and the results were limited to the English language and in-human studies (see screenshot of search in Appendix A1).
Study Selection
Studies were screened manually within each database and selected if there was an indication of real-time telemedicine associated with the delivery of care or therapy for patients with a movement disorder in the title or abstract. A data charting form was created in Microsoft Excel, and duplicates were removed by searching for keywords within each title using the Excel search tool and highlighting the articles to delete. Articles were excluded from the review if they were assessing internet-delivered therapies or remote symptom tracking but did not involve a telemedicine component. Also, articles that recommended telemedicine or that proposed a telemedicine program but did not evaluate telemedicine use in a population with a movement disorder were excluded. Table 1 provides the inclusion and exclusion criteria for studies in this review.
Inclusion and Exclusion Criteria
Data Extraction and Synthesis
Specific data were extracted independently by one of the authors (E.H.) from the eligible full-text articles and organized for evaluation within the data charting form by disorder. Extracted information included title, authors, publication year, journal, purpose, methods, sample size, target disease, reported outcomes, conclusions, and limitations. Due to the heterogeneity of the study methods, outcomes, and samples, a meta-analysis was not appropriate for this review. Rather, the outcomes for each article were determined through the title, objectives posed in the abstract, and the findings that were presented in the results. The main outcomes were then categorized into themes: feasibility, acceptability/satisfaction, validity/reliability, efficacy, and clinical outcomes. The frequencies of each category are presented below.
Results
Study Selection
The systematic searches of the three databases initially identified 228 studies. After duplicate articles were removed, as well as those that did not meet the eligibility criteria, 41 articles remained for the final review. The PRISMA flowchart summarizes this process (Fig. 1).
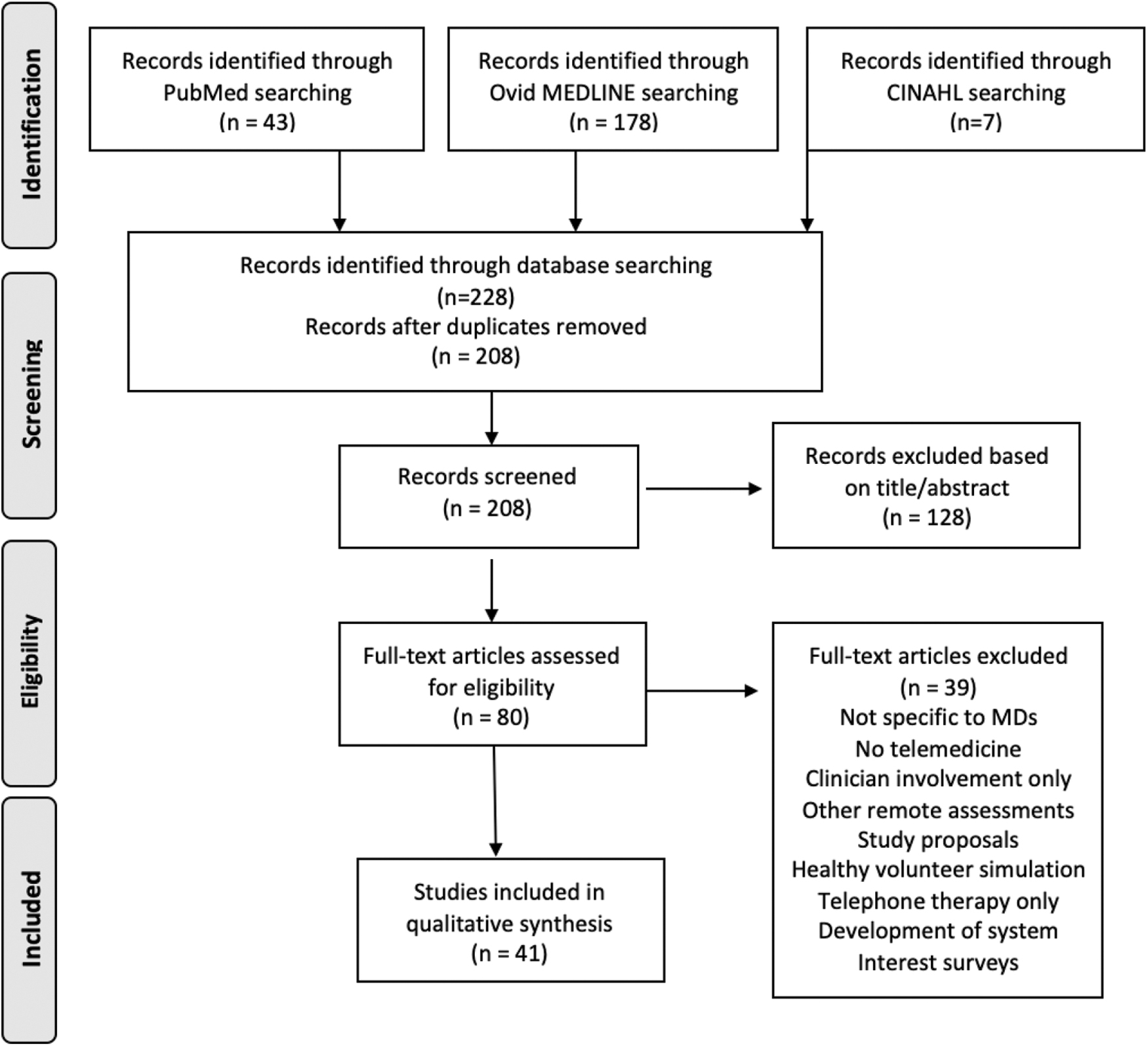
PRISMA flow diagram of study identification. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
The majority of studies involving a telemedicine application for movement disorders focus on its use within the PD population. Of the articles selected for this review, 35 articles involved evaluation of telemedicine for PD alone (85%). 3,10 –12,16,22 –48 Two of the articles focus solely on telemedicine use in HD (5%), 49,50 and one study evaluated both PD and HD (2.5%). 51 The remaining articles examine telemedicine application in a pediatric population that experiences tics (7.5%) 52,53 as well as participants who are at risk for developing a drug-induced movement disorder, based on duration of antipsychotic use (2.5%). 54 A summary of study characteristics is presented in Table 2.
Characteristics of Eligible Studies
ABC, Activities-specific Balance Confidence; ADL, activities of daily living; AEs, adverse events; AIMS, Abnormal Involuntary Movement Scale; ASQ, IBM After-Scenario Questionnaire; BBS, Berg Balance Scale; CBIT, Comprehensive Behavioral Intervention for Tics; CSQ, Client Satisfaction Questionnaire; CTD, chronic tic disorder; DBS, deep brain stimulation; DGI, Dynamic Gait Index; DIP, Dysarthria Impact Profile; F2F, face-to-face; FIM, functional independence measure; HD, Huntington's disease; ICC, intraclass correlation coefficient; LSVT, Lee Silverman Voice Treatment; MDS, movement disorder specialist; MGHAA-CSS, Modified Group Health Association of America's Consumer Satisfaction Survey; MHC, mental health clinician; MoCA, Montreal Cognitive Assessment; NJ, nasojejunal; NPTQ, Nurse Post-Telehealth Questionnaire; PD, Parkinson's disease; PDQ-39, Parkinson Disease Questionnaire–39 items; PDQ-8, Parkinson's Disease Questionnaire–8 items; PEG/J, percutaneous endoscopy gastrostomy with a duodenal/jejunal expansion tube; PPTQ, Patient Post-Telehealth Questionnaire; PT, predictive testing; PTQ, Parent Tic Questionnaire; PwP, people with PD; QOL, quality of life; RCT, randomized controlled trial; RD-tDCS, remotely supervised-transcranial direct current stimulation; SAE, serious adverse event; SLP, speech language pathologist; SPL, speech pressure level; SRE, self-regulated exercise; TAE, telecoach-assisted exercise; TAQ, Treatment Acceptability Questionnaire; TM, telemedicine; TR, telerehabilitation; UHDRS, Unified Huntington Disease Rating Scale; UPDRS, Unified Parkinson's Disease Rating Scale; VoIP, voice over internet protocol; VR, virtual reality; YGTSS, Yale Global Tic Severity Scale.
Nearly one third of the studies included in this review employ a RCT design (34%); nine studies in PD, 3,11,15,26,30,31,33,37,44 one HD trial, 48 and two of the chronic tic disorder (CTD) studies. 49,50 This includes two PD studies that expand on the primary data analyzed as a result of a large RCT published by Beck and colleagues. 28,29 The remainder (66%) are reported as case reports, case series, or cohort studies. Among the articles reviewed, most (71%) enrolled 50 participants or less, identify as pilot studies, or focus their objectives on feasibility. There are 12 articles (29%) with a sample size larger than 50; 4 of those studies enrolled more than 100 participants with a movement disorder (PD), and each article was published in the last 5 years. 11,27,36,37
Categorization of Reported Outcomes
Only a few of the articles included in this review explicitly stated their primary and secondary outcomes. 3,11,15,26,31,32,40,44,46,52,53 Other articles state their planned outcomes in the abstract, as well as report them in the results section. As indicated below, there are studies with multiple outcomes, which have been categorized into five themes: feasibility, acceptability/satisfaction, efficacy, validity/reliability, and clinical outcomes.
Feasibility
The feasibility of completing telemedicine visits and conducting the videoconferencing sessions using the necessary technology was evaluated in 21 studies. In an early study published in 2006, the authors reported that telemedicine was effective for conducting follow-up visits for people with PD (PwP) who lived at facilities, which had an established telemedicine network with the Seattle Veterans Administration Medical Center. 42 In a 3-year period, the facilities used existing equipment to complete 100 follow-up visits for 34 patients, with an internet connection speed of only 384 Kbps (kilobits per second). Following this study, an effort has been made to assess the feasibility of completing real-time video calls in the patients' homes, eliminating the need to travel.
A large RCT assessing telemedicine use in PD defined the primary outcome of feasibility by the percentage of participants who completed at least one visit (98%) and visits that were completed as scheduled (91%). 11 The authors reported that 96% of the study participants were familiar with the internet and email and that 54% had previously participated in a video call. Similarly, in 2013, Dorsey et al. examined the feasibility of providing care to PwP in a rural community and found no significant difference in proportion of completed visits between the in-person group and the telemedicine group (p = 0.99). 26 In an effort to report on the feasibility of a telemedicine visit with a Movement Disorder Specialist (MDS) in a large, multicenter cohort study, 277 participants were enrolled and the number of participants who completed a visit was provided (258), as well as the percentage of visits that occurred as scheduled (91%). 36 Two articles assessed the feasibility of performing the Montreal Cognitive Assessment (MoCA) through telemedicine, with one measuring the outcome as the number of MoCA items completed remotely (all of them) 43 and the other study determining feasibility by the rate and description of technological complications. 47 In 2015, Chen et al. published an initial examination of the demands for remote deep brain stimulation (DBS) evaluation and determined that there was an urgent need for DBS postoperative follow-up. 25 The results from four clinical cases indicated that telemedicine is a feasible method of conducting these visits for patients with DBS. Overall, telemedicine has been shown as a feasible and efficient means of connecting health care clinicians with patients of varying needs. 55
Acceptability/satisfaction
The other most commonly reported outcome was acceptability or satisfaction, terms that appeared to be used interchangeably and were found in 20 of the reviewed articles. In British Columbia, the application of telemedicine to predictive testing for HD was examined, and the authors reported that there was no significant difference in participant satisfaction between the in-person and telemedicine groups. 51 The surveys contained questions related to participants' experience with the predictive testing process, reflecting how acceptable they found it, as well as questions directly asking about levels of satisfaction. Examples were: “Overall I was given enough support from the genetics team during the period following my genetic results” and “Overall I was satisfied with the support provided during the entire process by the health care professionals.” In one of the many PD studies that looked at both feasibility and patient satisfaction, six aspects of the telemedicine visit were highlighted to determine levels of satisfaction. 45 On a scale from “very satisfied” to “very unsatisfied,” participants were asked to rate items such as quality of the connection, the specialist's ability to gather relevant information, and their ability to convey feelings, symptoms, and information to the specialist. For all items, at least 90% of participants were satisfied or very satisfied. 45 Two studies of long-term follow-up care for PD reported high satisfaction with telemedicine among patients, families, neurologists, and the nursing staff, regardless of one of the studies being published early on in 2006 and noting less-than-optimal video quality in 82 of 100 visits. 10,42 In general, studies that have assessed satisfaction with telemedicine found the majority of participants to be satisfied, likewise for clinicians who are involved. 3,12,13,15,16,24,25,27,35,36,40,45,47,48,50
Efficacy
Efficacy is an outcome that not only overlapped with feasibility and satisfaction in a number of studies but also became the primary outcome in most of the articles involving a therapeutic intervention. Among the PD studies, we identified seven studies involving the delivery of the Lee Silverman Voice Treatment (LSVT) 13 –15,32,34,41,46 and five implementing a physical therapy or activity program. 31,33,37,41,44 In six of the articles, changes in speech from baseline to the end of a 4-week intensive program indicated the efficacy of the program. Constantinescu et al. reported in 2011 that online delivery of LSVT is noninferior to in-person based on the mean change in sound pressure level on a monologue task. 15 This was following two preliminary studies that determined delivery of LSVT through telemedicine was effective in achieving comparable gains in speech. 13,34 Four of the physical therapy articles reported on efficacy measures, such as the Berg Balance Scale, 10M walking test, and Time Up and Go Test, following the use of a virtual reality balance training program or a coaching program called Engage-PD. 31,37,41,44 Gandolfi et al. 31 reported a significant improvement in physical performance after 7 weeks of therapy. Quinn et al. reported that in the context of the COVID-19 pandemic, PwP who participated in their study and received individualized exercise programs remotely had improvements in their physical activity. 41 In children with a CTD, two studies have examined the use of telemedicine to deliver Comprehensive Behavioral Intervention for Tics (CBIT), measuring the pre- to post-treatment change with the Yale Global Tic Severity Scale (YGTSS). 52,53 Similar to physical and speech therapy in PD, the CTD studies showed that CBIT administered through telemedicine was effective for reducing tics, without a significant difference between the in-person and remote groups.
Validity/reliability
In this review, 11 articles report assessing for validity, reliability, or both. Inter-rater reliability was evaluated in five of the studies by comparing in-person with telemedicine findings, typically done in tandem. 14,33,35,49,54 In 2011, Amarendran et al. 54 described their methods for determining if the Abnormal Involuntary Movement Scale (AIMS) could be reliably measured through telemedicine. In their study, participants in an examination room were observed by two psychiatrists face-to-face, and two psychiatrists in a nearby room, who completed the assessments through video and audio equipment. Calculating for the intraclass correlation coefficient (ICC), they determined consensus of the raters and found concordance with their AIMS scores. An example of measuring validity can be seen in a study that leveraged the online registry for PwP, Fox Trial Finder, to recruit participants and connect them with an MDS for one visit. 27 The researchers accessed the participants' self-reported data in Fox Trial Finder, including their diagnosis, which they compared with their own impressions following the telemedicine visit. They determined the validity of self-diagnosis of PD in 97% of cases.
The pilot RCT published by Dorsey et al. in 2010 assessed both the test–retest reliability and validity of the Unified Parkinson's Disease Rating Scale (UPDRS) motor subscale, which was completed at multiple time points via telemedicine. 3 The UPDRS Part III was initially completed at the baseline visit and again at the month 1 visit, following no changes to participants' medications. There was fair or better agreement for all motor items between the in-person and telemedicine assessments (Cohen's kappa = 0.20), except for rigidity and leg agility (Cohen's kappa = −0.09 and −0.30, respectively). These values improved when three motor fluctuators were excluded from the analysis. The final two sets of UPDRS motor assessments were performed 2 weeks apart at month 6 and 6.1 and used to calculate test–retest reliability. The reported ICC was 0.82, signaling an excellent test–retest reliability for the UPDRS Part III performed through telemedicine.
Clinical outcomes
Nine studies have reported outcomes that fall outside the four previous categories, yet are meaningful in how they describe participant experiences with, and implications of, telemedicine. For instance, four of these studies provide data on clinical recommendations made to participants or Primary Care Physicians, by an MDS. The percentage of encounters with a care recommendation or most common care recommendations were reported. 29,42,43,47 In addition, Mammen et al. 38 aimed to qualitatively evaluate how PwP and physicians perceive telemedicine visits, describing how the convenience and comfort of the virtual calls were beneficial, how they experienced quality care with frequent visits and thorough assessments, and how the remote sessions allowed for interpersonal engagement. Other broad clinical outcome measures include rates of serious adverse events and device complaints, 48 as well as quality-of-life scales, when they are not used as efficacy tools. 31
Discussion
Summary of Evidence
This scoping review aims to provide an overview of the existing literature evaluating telemedicine use in movement disorders. Since Hubble et al. published their accounts of using videoconferencing to interact with PD patients in 1992 and 1993, 35,56 many studies have set out to demonstrate the feasibility, validity, and reliability of visits completed remotely. Investigators have employed unique methodologies in their trials, while aiming for similar outcomes. We categorized these outcomes into five groups and highlighted key findings from each one.
In many of the applications of telemedicine described here, researchers are delivering therapies that have already been proven as effective in their target populations. For instance, the LSVT program has been well established as an effective speech therapy for PwP who experience dysarthria. 57,58 Similarly, for children with CTD, CBIT has been endorsed as a first-line treatment for reducing tic symptom severity. 59 Of note, there are data to support the importance of an in-person visit with an MDS for improving health outcomes for PwP, 60,61 but the question remains: Do patients who complete visits through real-time telemedicine experience these same benefits? Studies completed to-date seem to overwhelmingly endorse the use of telemedicine, with positive patient and clinician feedback, as well as favorable feasibility data. The novelty of many of the studies included in this review is the telemedicine component—the ability of clinicians to provide evidence-based therapies to patients who are not physically in front of them—while maintaining a high quality of care. Rapid technological advances from the early 2000s to the mid to late 2010s facilitated the evolution of evaluating telemedicine, from the development and testing of the systems 42,62,63 to advances in wearable technology, web-based applications, and improvements in internet connectivity. 64,65 A recent example is the Food and Drug Administration (FDA) approval of Abbott's NeuroSphere™ Virtual Clinic, which allows for remote programming of neuromodulation therapies and real-time communication between patients and clinicians. As we continue to explore the applications of telemedicine and the potential for remote monitoring, the opportunities to expand on delivery of care will continue to grow.
Recently, and in the context of increased telemedicine use, there is concern that remote visits will diminish the connection between patient and physician. 66 Our review found that patients were satisfied with both initial consultation visits 36,45 and follow-up visits 12,41 performed through telemedicine, and some individuals may prefer a combination of remote and in-person visits. 39 Dorsey et al. 67 emphasized the importance of patient-centered care, which should be flexible to meet the patient's needs; this includes the ability to expand access to specialist care and minimize travel for those who would be more comfortable remaining in their own home. In movement disorders, clinicians have scrutinized ways to adequately assess a patient without being able to put hands on them. For instance, in PD, there are limitations to completing the Movement Disorder Society–Unified Parkinson's Disease Rating Scale (MDS-UPDRS) 68 motor subscale, as rigidity (item 22) and postural stability (item 30) cannot be examined remotely. 26 However, modified UPDRS motor examinations have been proposed and reported as potentially reliable and valid clinical outcomes for PD patients, 69,70 further establishing outcomes that may be conducted at a distance and compared with the standard assessments, especially in the context of consistently missing values. 71
The COVID-19 pandemic has disrupted many neurological services worldwide. 72 It has also created an opportunity for evolution of our care models, with a large focus on the incorporation of telemedicine. Chen and Hemmen 73 stated that by addressing gaps in care we may “develop a feasible telehealth system for a high-quality standard of care post-pandemic.” At present, thousands of patients and health care professionals are using telemedicine to conduct clinic visits, research visits, and to participate in therapy sessions. In March to April 2020, the International Parkinson and Movement Disorder Society Telemedicine Study Group launched a survey across 40 countries to assess 4 domains of telemedicine: legal regulations, reimbursement, clinical usage and tools, and barriers within each region. 74 Their report confirmed a global increase in all forms of telemedicine, including telephone calls, messaging apps, and video visits. Even though the rise of telemedicine use was consistent across low- and high-income countries, there is a wide spectrum of regulations and infrastructure support. Reimbursement also ranged from none to partially or fully covered by insurance in some countries. Members from 12 countries reported changes in national policy related to telemedicine during the pandemic, including South Korea, where it was previously illegal to use video calls for clinical care. 74 Shalash et al. 75 recently report on varying levels of patient comfort and acceptance of telemedicine among different socioeconomic and cultural groups. There continues to be ongoing concerns with communicating sensitive information and loss of privacy, and barriers to uptake, such as limited computer literacy, and poor audio/video quality due to internet connectivity issues. 74,75
On a positive note, movement disorder specialists attest that during the COVID-19 pandemic patients and clinicians have gained experience with telemedicine, promoting equity of access to specialized interdisciplinary care. 75 To ensure continuity of care, as well as clinical research efforts, telemedicine became the safest way to complete visits for chronic diseases such as PD, which can entail frequent medical management and therapeutic adjustments. 76,77 Worldwide, clinicians and investigators have been sharing their experiences with telemedicine during the pandemic, reporting on factors that support their transition to remote care. In the first 5 weeks of the COVID-19 pandemic, 60% of previously scheduled in-person visits successfully converted to telemedicine visits at a large academic movement disorder center, with distant patients more likely to make the switch, as well as males, and more PD patients completed telemedicine visits than the patients with other movement disorder diagnoses. 55 It was also noted that patients with DBS chose to transition to telemedicine visits at a higher rate than patients without DBS. Some neurologists are skeptical that a remote examination is well suited for a new diagnosis, especially in complex cases, and prefer to conduct follow-up visits with established patients. 75,78,79 Additional researchers believe that smartphone applications and wearable sensors for remote patient monitoring can provide objective data that may be used to supplement the MDS-UPDRS or virtual examinations, as well as to complete outcome measures. 76,77,79
In summary, there has been an unexpected shift toward remote visits, and the combination of research evidence and real-life experience should continue to promote the utilization of telemedicine moving forward. Future studies can help investigators determine if there has been any change in patient and physician perceptions of telemedicine since the pandemic, as well as the preferred methods of completing visits and collecting data. These insights would enable the implementation of telemedicine, addressing barriers to accessing health care, while disseminating specialized neurological care, especially in rural areas and regions with limited connectivity.
Limitations
In this scoping review, we did not intend to assess the quality of the literature through a critical appraisal, but instead aimed to provide a comprehensive summary of the studies and key outcomes. The outcomes could not be compared, due to the different study designs, samples, and interventions. The initial article screening and data charting were performed independently by one rater, which could have biased the articles chosen or the details that were selected from the articles.
Conclusions
Telemedicine use in movement disorder populations, especially PD, is a feasible, acceptable, and effective way to provide care in many settings. Health care professionals and patients have quickly adapted to remote visits during the COVID-19 pandemic, and this may shape how we deliver care in the future. Additional research into implementation of telemedicine services will be essential in guiding decisions for patient-centered care, and researchers could harmonize the way they evaluate it through developed frameworks.
Footnotes
Authors' Contributions
Ms. Houston is responsible for the article concept and design, as well as data acquisition and interpretation. She was involved in drafting and revising the article and will be accountable for all aspects of the work. Dr. Kennedy contributed to the conception of the article, as well as interpretation of the data and provided critical revisions for intellectual content. Ms. O'Malley contributed to data acquisition and critical review of the article. Dr. Rabinowitz has been involved in interpretation of the data and revising the work critically for important intellectual content. Dr. Rose contributed to interpretation of the data and critically reviewed the drafts, providing important revisions to intellectual content. Dr. Boyd was involved in developing the article concept and design, interpreting data that were synthesized, and critically revising the article for intellectual content.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.