
Abstract
Background:
There are disparities in access to specialty care for chronic diseases in rural and minority populations. Telemedicine has been proposed to improve access.
Introduction:
The objective of this study was to identify predictors of telemedicine use for chronic disease specialty care in the Alaska Tribal Health System (ATHS) in the setting of usual care.
Materials and Methods:
We utilized data from the electronic health record (EHR) of patients from four regions in the ATHS. We queried the EHR to identify cases (ever users of telemedicine) and controls (never users), both of whom had chronic diseases requiring specialty care. Data were collected from 2015 through mid-2019.
Results:
We included 3,075 patients (799 ever users and 2,276 never users). In univariate analysis, ever users were older, more likely to be male, had more chronic conditions and higher encounter rates. There were differences by region, community, and type of specialty clinic. In our simple multivariate model, factors associated with telemedicine use included age, male gender, region, and outpatient visit rate per year. Having at least one cardiology clinic visit was also associated with telemedicine use, with the highest estimated odds ratio (5.27, p < 0.01).
Discussion:
This study describes factors associated with telemedicine use in the ATHS before the COVID-19 pandemic. We anticipate monitoring changes in these predictors over time, as we expect them to evolve.
Conclusions:
We found among factors associated with telemedicine use were age, gender, region, outpatient visit rate, and visits to a specific specialty clinic.
Introduction
The prevalence of chronic disease is high in rural and minority populations in the United States, including Alaska Native and American Indian (AN/AI) populations. 1 Many chronic conditions are associated with lifestyle factors and respond well to primary care and public health interventions. For patients with certain chronic conditions, access to specialty care also improves outcomes. 2 –4 Access to specialists is limited for rural and minority populations, given existing shortages of many specialists and maldistribution in urban academic settings. Telemedicine has been proposed by many specialist organizations to improve access to specialty care. 5 –7 Before the COVID-19 pandemic, uptake of telemedicine by physicians and health care systems was limited, 8 but its use has rapidly expanded recently during the pandemic and it is expected to continue to evolve. 9
The Alaska Tribal Health System (ATHS) is a statewide network of tribal health organizations providing primary and specialty care to Alaska Native people. Telemedicine has been available in some form in the ATHS for >20 years. Early in its course, store-and-forward (asynchronous) telemedicine was the primary modality used. With improvements in connectivity, the ATHS expanded the use of synchronous video telemedicine beginning in 2012, with greatly expanded uptake by multiple clinics occurring in 2015.
The most common method of delivering video telemedicine has been from clinic to clinic, often with the patient at a rural clinic in their home community, and the provider at a larger regional facility or the statewide tertiary care hospital. Direct-to-patient synchronous telemedicine was rare during the time of data collection but has increased during the COVID-19 pandemic where adequate connectivity is available. The Alaska Native Tribal Health Consortium (ANTHC) provides statewide specialty care services, which led us to design this study to understand the predictors of telemedicine specialty care among patients with chronic diseases receiving care in the ATHS.
Few studies have described patient and community characteristics associated with telemedicine use. Provider factors also influence uptake of telemedicine, and have been important determinants of telemedicine use in some studies. 10 In addition to patient and provider characteristics, aspects of specific health care needs for different chronic conditions, as well as health system factors, are likely associated with telemedicine use.
We previously published a qualitative study using semistructured in-depth interviews with patients and providers. 11 Building on the results of that study, we designed a mixed methods study with an initial aim of evaluating the predictors of telemedicine use for chronic disease specialty care in the ATHS. Future study aims will evaluate the outcomes and costs of telemedicine. The analysis presented in this article uses quantitative data from the electronic health record (EHR) to address our first study aim of identifying predictors of telemedicine use. Data presented herein were collected before the onset of the COVID-19 pandemic. Changes in telemedicine use during and after the pandemic will be examined in future phases of this study.
Materials and Methods
The Alaska Area IRB (AAIRB) approved this observational study as expedited research with a waiver of consent for this component of the study. In addition to receiving AAIRB approval, the study was approved by all four regional tribal health organizations participating in this component of the study, as well as the statewide tribal health organization, ANTHC.
STUDY POPULATION
Data collection for this study included patients in four regions of the ATHS. Because telemedicine was already widely used throughout the ATHS, we were unable to randomize patients to receive care by telemedicine or not. As such, we utilized data available in the EHR and an observational study design to explore factors associated with telemedicine use in the setting of usual care.
To be included in the study, patients were required to be age 18 or over, to have a chronic condition (as defined by the chronic condition indicator developed as part of AHRQ's Healthcare Cost and Utilization Project [HCUP] to categorize International Classification of Diseases [ICD]-9 and ICD-10 codes as chronic or nonchronic), 12 and to have had a visit in a specialty clinic in the ATHS, either through telemedicine, or in-person, or both, between January 1, 2012 and June 30, 2019. Furthermore, to be eligible for the study patients were required to reside within communities in the four regional tribal health organizations participating in this study. We did not require patients to be of AN/AI race to be included in the study, but almost all patients eligible for care in the ATHS are AN/AI.
DATA COLLECTION AND DEFINITIONS
We queried the ATHS shared EHR system (Cerner) to identify cases (telemedicine ever users) and controls (never users) who met the inclusion criteria for chronic conditions as specified earlier and had any visit between 2012 and mid-2019. We defined cases (telemedicine users) as the subset of patients who had ever used telemedicine between 2015 through mid-2019. Patients who never used telemedicine during the full-time period (2012 to mid-2019) were designated as controls (never users). Because telemedicine was not used widely from 2012 to 2014, patients who had a telemedicine visit between 2012 and 2014, but no telemedicine visits in 2015 or later were excluded from the study. Characteristics and encounters of the filtered set of eligible study participants that were potentially associated with telemedicine use were included in the final data set for analysis.
Variables included in the final data set included demographic features, community and region information, chronic conditions, and health care utilization. Demographic features identified included age, gender, race, and marital status. If participants were deceased after the beginning of the study period, date of death was recorded. Community of residence was identified as the listed community in the EHR and was used to assess community level factors, including level of access (geographical proximity to health care services, ranging from 1 (most remote) to 4 (least remote)) and socioeconomic status (defined based on proportion of community receiving Supplemental Nutrition Assistance Program), as well as region of service.
Details of the number and types of chronic conditions for each patient were determined using the HCUP chronic category of ICD-9/ICD-10 codes for patient encounters during the study period. Health care utilization data we considered included total number of encounters during the follow-up period, type of encounters (inpatient, outpatient, and emergency), and type and number of specialty clinic encounters.
STATISTICAL ANALYSIS
We examined the association of patient and visit characteristics with telemedicine use. We calculated summary statistics using univariate analyses, and tested differences between telemedicine users and nonusers through chi-square tests, Fisher's exact tests, and t-tests as appropriate. Visit rates (both inpatient, outpatient, and emergency) were calculated based upon the duration a patient was followed. Both patient deaths and persons reaching age 18 during the study period affected individual follow-up times. In addition, because entry into the shared EHR system varied by region, the time frame (and thus follow-up length) of patient data available varied by region. An exception were patient encounters at specialty clinics, as these encounters are recorded in the Alaska Native Medical Center EHR (regardless of patient region), and are available for the entire study period for all patients. We defined consecutive outpatient encounters as a single encounter when the gap between encounters by a patient was 1 day or less; similarly, distinct inpatient encounters required a gap between inpatient encounters of >30 days.
To examine the influence of multiple covariates (both patient characteristics and encounter characteristics) simultaneously on telemedicine use, we used multiple logistic regression. We selected initial candidate covariates to include in our models based upon the results of our univariate analyses, as well as their clinical meaningfulness. The final model we selected resulted from a balance of understandable covariate representation (indicator, categorical, linear, or polynomial) and model fit in combination with the number of degrees of freedom required (specifically, using Akaike information criterion). Although we considered interaction terms, we found only minor evidence of effect modification, and more frequently observed indications of indirect effects through multiple covariates on telemedicine use.
In addition to our final model, we also generated a simpler model (trading optimal fit for improved understanding) of the most salient covariates, to facilitate our understanding of the basic characteristics of patients and encounters that influence who utilizes telemedicine. Results of both model fits are provided through odds ratios and their confidence intervals, as well as p-values of the model fitted coefficients. All analyses were performed using R Statistical Package, version 4.0.3.
Results
The total population included 3,075 patients, of whom 799 had ever used telemedicine and 2,276 had not. In Table 1, patient characteristics (including demographics, community characteristics, chronic conditions, and health service utilization) and clinic factors are shown, with comparisons between those who had not used telemedicine versus those who had. Notable differences in univariate comparisons between these groups included older age in those ever seen by telemedicine and an increased proportion of males.
Characteristics of Patients Never Versus Ever Using Telemedicine
Distinct visits are defined as visits that do not occur on the same day or consecutive days for outpatient visits, and hospitalizations that do not occur within 30 days of each other.
HCUP, Healthcare Cost and Utilization project; SNAP, Supplemental Nutrition Assistance Program.
The use of telemedicine varied by region of residence. Both community factors (level of access and average community level socioeconomic status) and region of residence were associated with telemedicine use. Ever users of telemedicine had a higher mean number of chronic conditions and higher outpatient and inpatient encounter rates during the follow-up period, but did not have a higher rate of emergency department visits. The specialty clinic most associated with telemedicine use was cardiology. We found that the cardiology visit rate was higher in telemedicine users, and that 67% of telemedicine users had at least one visit to cardiology clinic, compared with just 23% of nonusers (p < 0.01).
We investigated specific categories of chronic conditions and specialty clinic visits in more detail, as presented in Table 2, Figures 1 and 2. As shown in Table 2, a high proportion of telemedicine users had disorders of the circulatory system diagnosed (85%), whereas behavioral health conditions were the most common category of chronic condition in nonusers (67%). Table 2 also shows the most common clinics visited at least once by patients with or without a history of telemedicine use, led by cardiology clinic among telemedicine users and orthopedics clinic among never users.
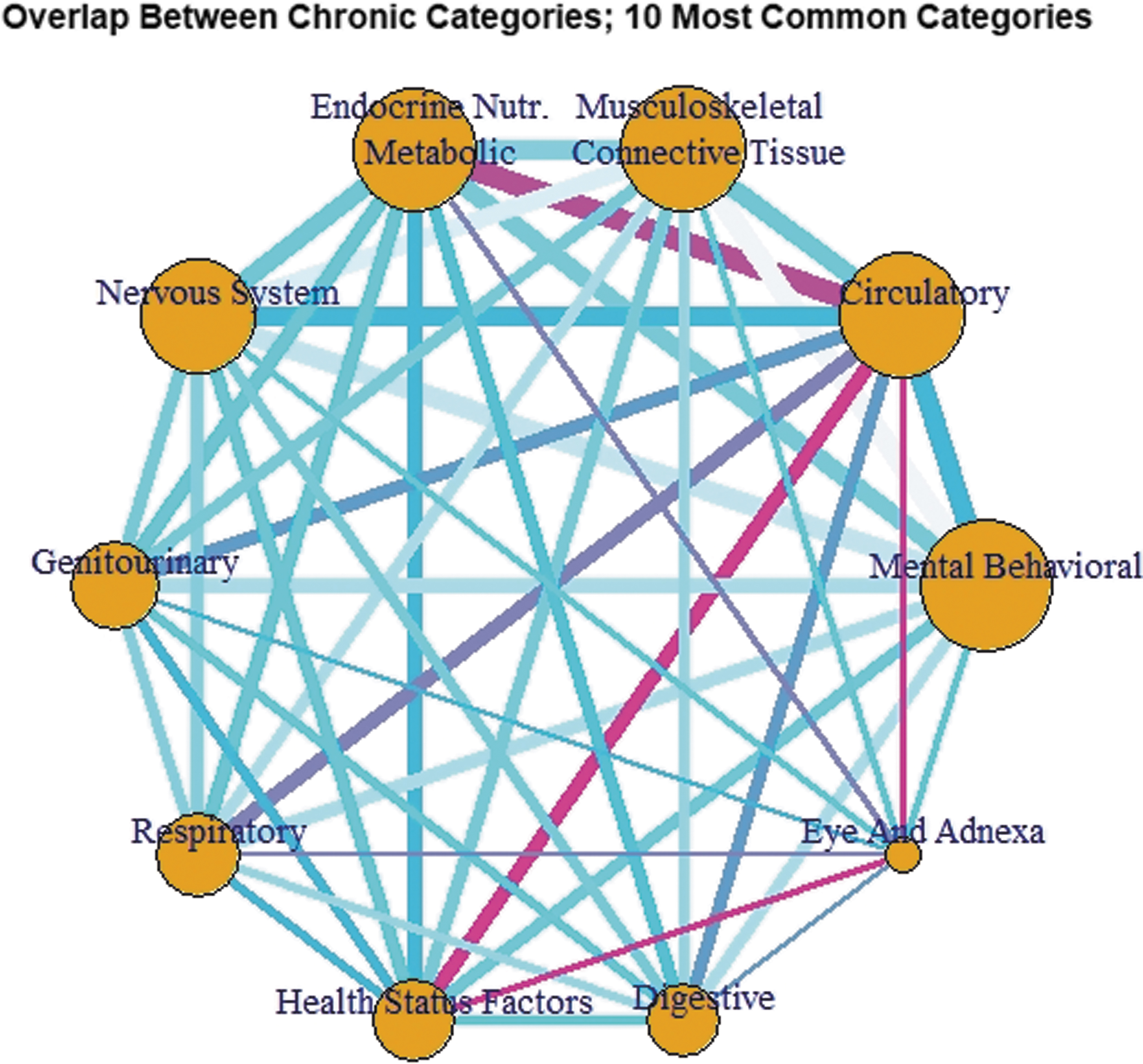
The circles represent categories of chronic conditions, with larger circles indicating more patients with those conditions. The width of the connecting lines is thicker when more patients have that pair of conditions. The color gradient of the lines (light blue to deep pink) represents the proportion of all patients with that pair of conditions who are telemedicine users, with pink representing a higher proportion, light blue the lowest, and purple intermediate.

The circles represent clinics, with the size of the circle representing the relative number of patient visits to the clinic. The width of the connecting lines indicates the number of patients having visits to both clinics in the pair. The color gradient (light blue to deep pink) of the lines represents the proportion of patients with visits to a pair of clinics who were telemedicine users, with pink representing a higher proportion, light blue the lowest, and purple intermediate.
Top Five Categories of Chronic Conditions and Clinics Visited for Never Users Versus Ever Users of Telemedicine
ICD, International Classification of Diseases.
Figures 1 and 2 are network diagrams depicting the relationship between pairs of chronic condition categories (Fig. 1), and between pairs of specialty clinics (Fig. 2). As noted in the figure legends, the color of the connecting lines represents the proportion of visits in that particular combination of conditions or clinics that were made by telemedicine users, the size of the node indicates the total number of patients, and the thickness of the connecting edges represents the frequency of occurrence of that pair.
Multivariate models of the factors associated with telemedicine use are presented in Tables 3 and 4. The model presented in Table 3 represents the best fit model, whereas the simple model in Table 4 was selected to be more readily applicable in clinical care. Factors associated with telemedicine use in these models include age (older), gender (male), region (all regions had higher rates than the reference region), the number of outpatient visits per year, and visits to cardiology clinic. Although the number of chronic conditions is included in the best fit model, this variable was excluded from the simple model given its limited predictive value.
Best Fit Multivariate Model of Factors Associated with Telemedicine Use
Specialty clinic visits per year of follow-up, excluding cardiology clinic. Categorized as zero to less than one visit per year (0,1), one to less than three visits per year (1,3), three to less than 5 visits per year (3,5) or 5 or more visits per year.
CI, confidence interval; OR, odds ratio.
Simple Multivariate Model of Factors Associated with Telemedicine Use
Discussion
In this observational study conducted before the COVID-19 pandemic comparing patients receiving chronic disease specialty care who had ever used telemedicine to those who had not, we found that older age, male gender, region of residence, higher outpatient visit rates, and any visits to cardiology clinic were associated with higher odds of telemedicine use in the multivariate models. In addition, patients who ever used telemedicine had more chronic conditions present. There was overlap between chronic conditions and specialty clinics, but overall the strongest predictor was visiting a clinic that had a higher rate of telemedicine use. In this study, telemedicine use was most significantly associated with having any visit to cardiology clinic.
Few studies of telemedicine have addressed the factors associated with its use in clinics or hospitals providing care for multiple chronic conditions, including care by different specialty clinics. Cardiology clinic was the earliest adopter of telemedicine in the ATHS and it appears that clinic and provider buy-in are driving many of these findings. A qualitative interview study in Australia proposed that clinician acceptance explains most of the variation in use of telemedicine. 10 In other health care settings, it is likely that other specialty clinics might use telemedicine more often, and the finding of increased use by cardiology may not be generalizable. Although other studies have described the use of telemedicine in cardiology, most focus on modalities other than live video visits with a provider, such as remote patient monitoring, device monitoring, nurse management for heart failure, and remote echocardiograms. 13 –15 The findings that older patients and men were more likely to have used telemedicine in our study may be partially explained by their increased likelihood of visiting cardiology. However, even when controlling for clinic type visited, age and gender remain significantly associated with telemedicine use.
We anticipate that the acceptance of telemedicine and factors associated with its use will change over time, initially with increased adoption by other clinics, as well as changes in modalities offered in the future, such as direct-to-patient visits. Since the onset of the COVID-19 pandemic, there have been more dramatic changes, with rapid increase in uptake of telemedicine throughout the world and an increase in direct-to-patient telemedicine. The findings of this study are prepandemic and the importance of the specific conditions and specialties identified in this study in determining telemedicine use are likely changing. However, although we have seen widespread increase in telemedicine uptake globally during the pandemic, the levels and acceptance of telemedicine use that will persist is unclear.
Several findings of this study are useful for clinical practice. First, some clinicians might believe that cardiology is a specialty less amenable to live video telemedicine, but our findings demonstrate its feasibility and widespread acceptance in the ATHS. Second, it is clear that there are patient, community, and clinic factors associated with telemedicine use. Although some studies 16 suggest that older patients may be less willing to try telemedicine or seek health information online, 17 the average patient seen by telemedicine in our study was in their 60s, about 10 years older than those never seen by telemedicine, suggesting that older patients can be good candidates for telemedicine use. Other studies have found that overall health, rather than demographics such as age, can be the primary driver of the choice to use telemedicine. 18
This study has some limitations. Because it relies exclusively on data drawn from the EHRs, we are limited in our ability to explore all factors driving telemedicine use by certain types of patients or clinics. As such, we are conducting patient and provider surveys and patient focus groups as a component of our research and will use those findings to complement the findings described herein, which are derived from EHR data. Second, this study is observational and was conducted in the setting of usual care in the ATHS before the COVID-19 pandemic. The predictors of telemedicine use in the study population may not be generalizable to other settings. As mentioned, these predictors may also change in the future, particularly in response to the pandemic. Finally, because of differences among regions in their adoption and implementation of the shared EHR, the duration of follow-up varied by region although we accounted for these differences as appropriate in our statistical methods.
Conclusions
In summary, we found that among patients with chronic diseases seeing specialists in the ATHS, the factors associated with telemedicine use were older age, male gender, region of residence, outpatient visit rate, and visits to a specific specialty clinic (cardiology in particular). In future research, we plan to examine how these predictors are changing in a postpandemic world, as well as evaluate the outcomes and costs of telemedicine use.
Footnotes
Acknowledgments
We thank Sarah Freeman, PharmD, for her assistance with initial study design. We also thank the patients and tribal health organizations in the ATHS who contributed valuable data to this research study.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported by grant number R01HS026208 from the Agency for Healthcare Research and Quality.