
Abstract
Background:
Telemedicine usage in orthopedic surgery has seen a dramatic increase as a result of the severe acute respiratory syndrome coronavirus 2 pandemic. The purpose of this study was to examine patient perceptions with telemedicine at a large orthopedic practice.
Materials and Methods:
An anonymous online survey was distributed to all patients who received a telemedicine health visit at our institution for musculoskeletal complaints from March 17 to June 1, 2020. Responses were scored on a 5-point Likert scale (strongly disagree, disagree, neutral, agree, and strongly agree, 1–5) and analyzed by average score and percent reaching top box.
Results:
A majority of patients (76.5%) were satisfied with their visit, and only 19.2% did not want telemedicine as a future option. Patients who presented for follow-up visits (4.11 vs. 3.94, p = 0.0053; 48% vs. 41%, p = 0.02) and utilized video (4.21 vs. 3.88, p < 0.001; 51% vs. 39%, p < 0.001) were more satisfied. Average satisfaction between older (>65 years) and younger patients was similar (4.06 vs. 4.06, p = 0.97), however, younger patients were more likely to reach top box (42% vs. 51%, p < 0.001). Confidence that the physician came to the correct diagnosis (r = 0.78, p < 0.001) and receiving the same information and care as an in-office visit (r = 0.60, p < 0.001) demonstrated the strongest correlation with satisfaction and desire for future telemedicine visits, respectively. Interestingly, 31.1% of patients would have sought treatment elsewhere had telemedicine not been an option.
Conclusions:
Overall, satisfaction rates are high for orthopedic patients undergoing telemedicine visits. Patients are more confident in telemedicine when presenting for a follow-up visit and with the use of video.
Introduction
Telemedicine, a subset of telehealth, allows delivery of clinical care between two distinct geographic sites, typically through phone or videoconferencing. 1 Classically reserved for patients in remote locations without access to local clinics, telemedicine has garnered a substantial increase in usage in orthopedic surgery as a result of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. 2 Stay-at-home orders and fear of contagion resulted in the temporary cessation of nonurgent in-office visits, forcing health care providers to provide alternative methods of evaluation. Consequently, telemedicine, which abides by all social distancing guidelines, temporarily became the standard of care. However, most orthopedic physicians and patients were experiencing telemedicine for the first time.
Although telemedicine has demonstrated benefits, including increasing access to care and decreasing cost, 3,4 acceptance of this new standard of care was fueled by relaxation of governing rules and the Telehealth 1,135 waiver, allowing Medicare to cover the cost of visits furnished by telemedicine. 5 Before the SARS-CoV-2 pandemic, telemedicine in orthopedic surgery had been used sparingly, although use in outpatient care, postoperative evaluations, and rehabilitation showed promising results and high satisfaction rates. 6 –10
Telemedicine is, however, not without challenges. Makhni et al. described many of the barriers facing widespread implementation of telemedicine in orthopedic surgery. 11 These include implementation and maintenance costs, inefficiencies, decreased ability to perform physical examinations, lack of perceived benefit, negative financial implications for providers, possible increased medicolegal exposure, regulatory barriers, as well as lack of awareness, access, and technology literacy. Although efforts have been made to standardize aspects of the telemedicine visit, including the physical examination, 12 there is still no universal consensus. There is also skepticism or reluctance on the physicians' behalf. A 2017 study by Wongworawat et al. found that only 20% of surgeons see telemedicine as a way to provide postoperative care, 10% see telemedicine being used for supervised therapy, and 42% feel that their fellow colleagues would be disinterested altogether. 13
In the current digital age, telemedicine usage is predicted to increase even further with the rise of interconnected health devices and high-speed connectivity. 14 The purpose of this study was to examine patient satisfaction and comfort with telemedicine during the COVID-19 pandemic at a large orthopedic practice. We hypothesized that patients would be satisfied and comfortable with telemedicine and a large percentage would prefer to have telemedicine as an option in the future.
Methods
After obtaining Intuitional Review Board approval, an anonymous online 23-question survey was distributed via electronic-mail to all patients who received a telemedicine health visit at our institution for musculoskeletal complaints from March 17 to June 1, 2020. When scheduling their visit, patients were given the choice to complete either a phone or video visit. The survey included questions regarding demographic information and patient perceptions of their telemedicine visit. Follow-up e-mails were sent 1 week later to nonresponders. Responses were scored on a 5-point Likert scale (strongly disagree, disagree, neutral, agree, and strongly agree, 1–5).
The survey was distributed, and the results collected by Research Electronic Data Capture (REDCap) electronic data capture tools hosted at our institution. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. 15,16
Statistics
Significance testing of nonparametric variables was conducted using the Mann–Whitney U test and reported using medians with interquartile ranges. Normally distributed variables were analyzed using two-sided t tests and reported as means with standard deviations. Categorical variables were reported as counts with proportions and analyzed with the chi-square and Fisher's exact test where appropriate. Multiple linear regression was used to identify survey questions associated with overall satisfaction and preference for telemedicine in the future. We used Pearson correlation coefficients to identify any correlation between satisfaction and preference for telemedicine in the future with each survey question. p-Values <0.05 were considered to be statistically significant. Statistical analysis was conducted using Python software (version 3.7).
Results
In total, 1,558 patients (6.8%) with an average age of 63.3 years (median = 65, range 18–98) completed the survey. The average age of patients who sent the survey, 55.0 years (median = 57, range 18–103), was significantly lower (p < 0.001) than those completing the survey. A total of 30.3% of responders presented with a new injury, while 69.7% presented for a follow-up visit. Overall, 76.5% (1,192/1,558) of patients were either satisfied or very satisfied with the care they received during their telemedicine visit, and only 19.2% (299/1,558) of patients did not want telemedicine as an option in the future. Interestingly, 31.1% (484/1,558) of patients would have sought treatment elsewhere had telemedicine not been an option at our practice at the time of their visit (Table 1).
Overall Results for Patient Perceptions of Telemedicine
SD, standard deviation.
When comparing follow-up visits with new patient visits (Table 2; Fig. 1), analysis of average Likert score and percent reaching the top box score (strongly agree) revealed that patients presenting for follow-up were more confident that the physician reached the correct diagnosis (4.20 vs. 3.97, p < 0.001; 47% vs. 38%, p = 0.002), more strongly agreed that the care received was the same as an in-person visit (3.66 vs. 3.39, p < 0.001; 27% vs. 22%, p = 0.046), and had higher overall satisfaction (4.11 vs. 3.94, p = 0.0053; 48% vs. 41% p = 0.02). There was no difference between patients who were comfortable scheduling surgery (77.9% vs. 86.1%, p = 0.221).
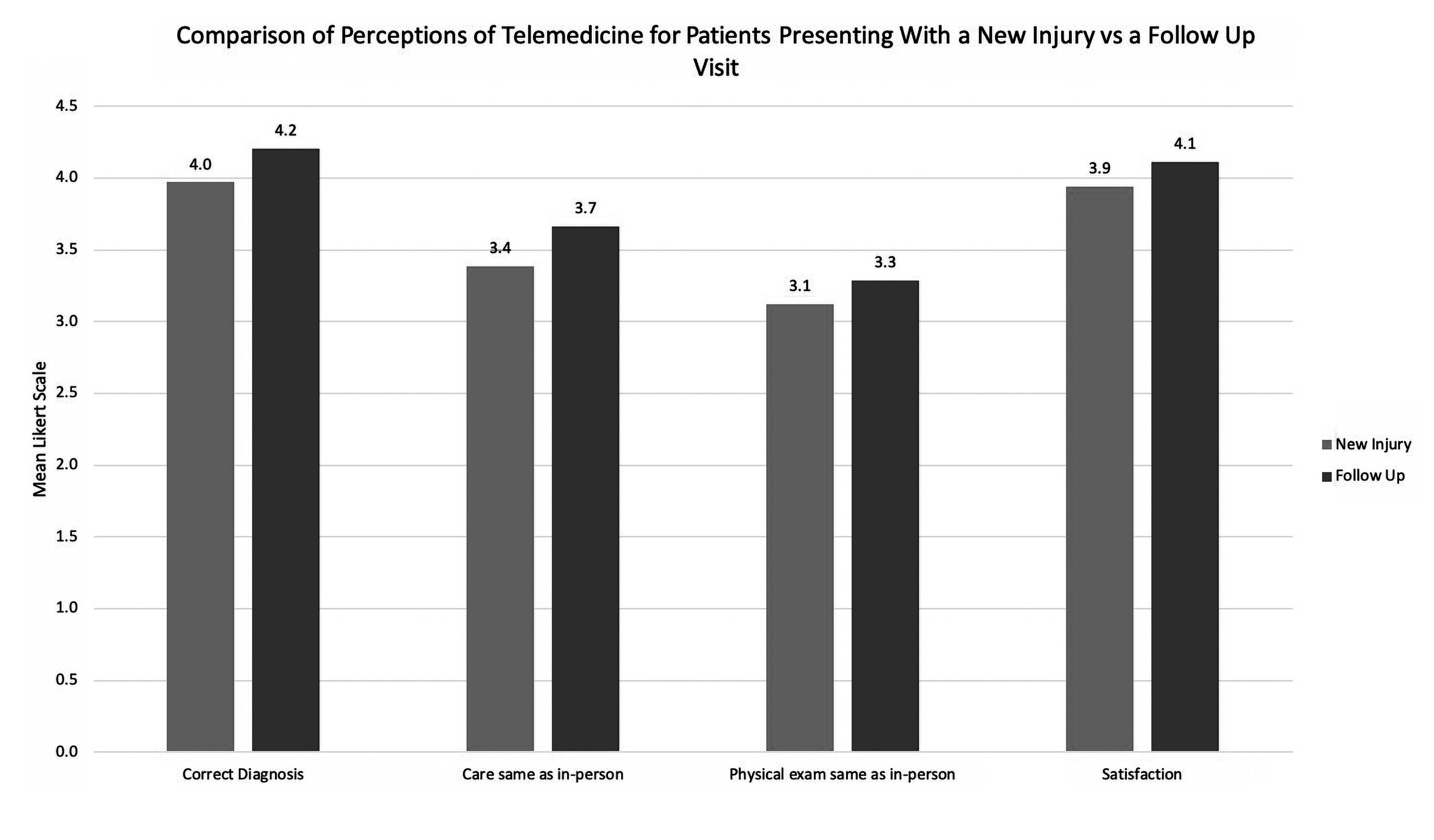
Comparison of perceptions of telemedicine for patients presenting with a new injury versus a follow-up visit.
Comparison of Perceptions of Telemedicine for Patients Presenting with a New Injury Versus a Follow-Up Visit
When comparing video telemedicine visits to phone-only visits (Table 3; Fig. 2), patients utilizing video demonstrated a higher overall satisfaction (4.21 vs. 3.88, p < 0.001; 51% vs. 39%, p < 0.001), were more comfortable scheduling surgery (87.9% vs. 72.4%, p = 0.011), more strongly agreed that the physician was able to simulate a physical examination similar to an in-person visit (3.45 vs. 2.96, p < 0.001; 24% vs. 14%, p < 0.001), were more confident that the correct diagnosis was reached (4.23 vs. 4.02 p < 0.001; 48% vs. 39%, p < 0.001), and that care received was the same as an in-person visit (3.70 vs. 3.43, p < 0.001; 29% vs. 22%, p < 0.001).
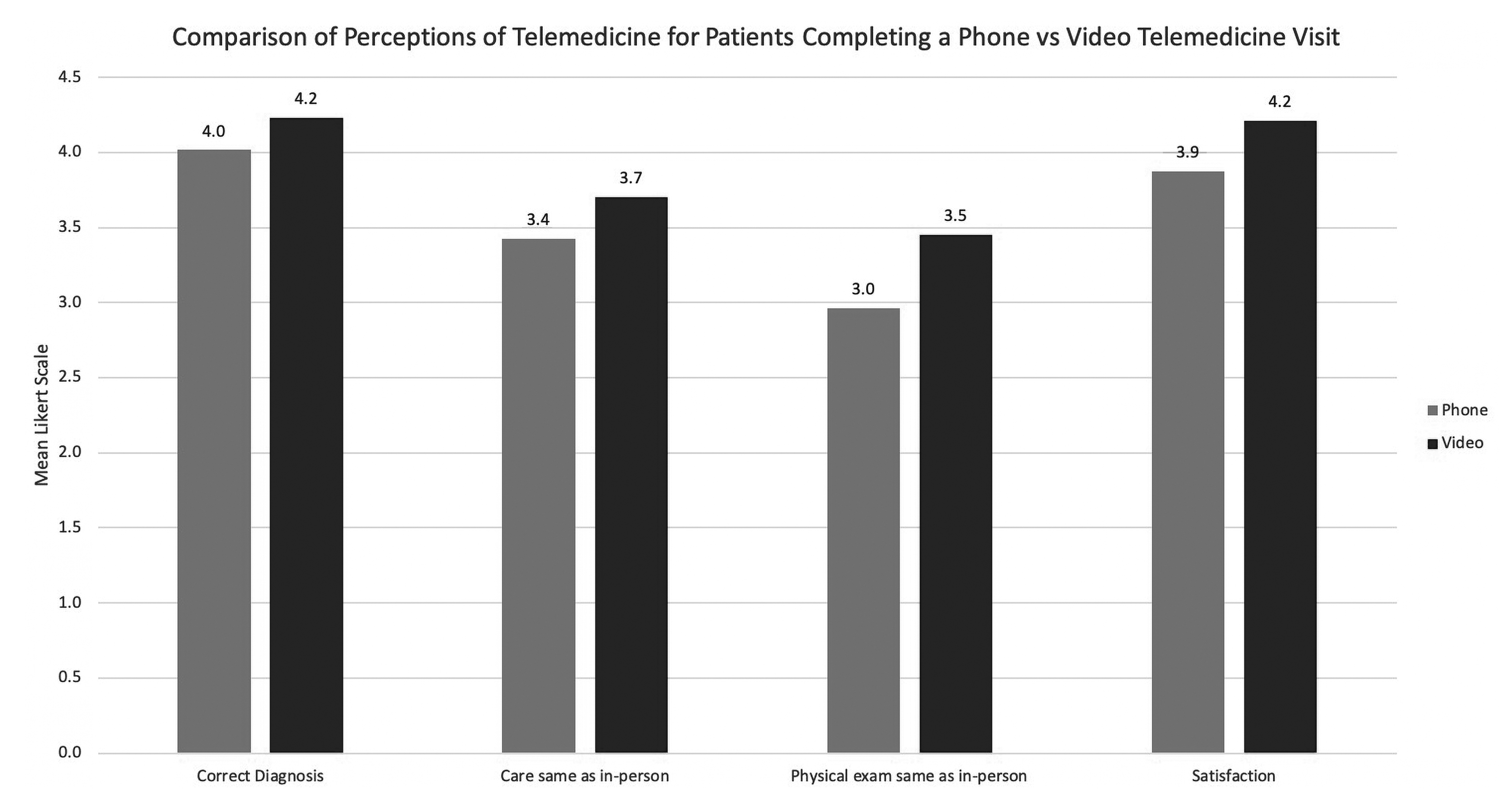
Comparison of perceptions of telemedicine for patients completing a phone versus video telemedicine visit.
Comparison of Perceptions of Telemedicine for Patients Completing a Phone Versus Video Telemedicine Visit
When comparing older patients (older than 65 years) with younger patients (Table 4), older patients were more likely to schedule a phone visit (51.0% vs. 36.9%, p < 0.001); however, there was no difference between comfort in scheduling surgery (79.0% vs. 83.1%, p = 0.59). Analysis of average Likert score revealed no difference in overall satisfaction (4.06 vs. 4.06, p = 0.97). In contrast, analysis of top box score demonstrated that patients younger than 65 years were more satisfied with telemedicine than patients older than 65 years (51% vs. 42%, p < 0.001).
Comparison of Perceptions of Telemedicine for Patients Younger Versus Older than 65
Using multiple linear regression (Table 5), how quickly was the visit scheduled (p = 0.044), providing guidance or reassurance regarding the injury (p < 0.001), receiving the same information and care as in-office visit (p < 0.001), listening to and understanding the history of the injury/pain (p < 0.001), the ability to simulate physical examination tests (p < 0.001), and confidence that the doctor came to the correct diagnosis (p < 0.001) all revealed significance in determining patient satisfaction. The regression (R 2 = 0.76) suggests a strong predictor of patient satisfaction. Again, using multiple linear regression (Table 6), providing guidance or reassurance regarding the injury (p < 0.001), receiving the same information and care as in-office visit (p < 0.001), the ability to simulate physical examination tests (p < 0.001), and confidence that the doctor came to the correct diagnosis (p = 0.036) all revealed significance in determining whether the patient desired telemedicine for future visits. The regression (R 2 = 0.406) suggests a weak predictor of patient desires for future telemedicine visits.
Multiple Linear Regression to Overall Satisfaction
Multiple Linear Regression to Desire for Future Telemedicine Visits
Correlation analysis revealed that confidence that the doctor came to the correct diagnosis (r = 0.78, p < 0.001) showed the strongest correlation with overall satisfaction, while how quickly was the visit scheduled (r = −0.17, p < 0.001) showed negligible correlation. For patients desiring telemedicine as an option in the future, receiving the same information and care as in-office visit (r = 0.60, p < 0.001) demonstrated the strongest correlation, while again how quickly was the visit scheduled (r = −0.11, p < 0.001) demonstrated negligible correlation.
Discussion
Telemedicine facilitates delivery of clinical care between two distinct geographic locations. Alongside the benefit of adhering to social distancing guidelines, telemedicine enables physicians to reach patient populations in remote locations thereby expanding the number of patients that can access health care services. Telemedicine also reduces cost by eliminating the need for transportation to and from appointments, limiting time off from work or school, and decreasing the amount of resources used. 3,7 Although there had been increased usage of telemedicine more recently, out of necessity, the SARS-CoV-2 pandemic dramatically increased the availability and adoption of telemedicine. As a result, we sought to identify and quantify patient satisfaction and comfort with telemedicine at a large orthopedic practice.
Overall, the majority of patients were either satisfied or very satisfied with the care they received during their telemedicine visit. Although we demonstrate high satisfaction rates, our data are lower than previous studies in orthopedic surgery, 80–99%. 8,17 –20 Similarly, we found that 53.1% would opt for a telemedicine in the future, which is again lower than previous studies, 86–92%. 7,17,21 Lower satisfaction rates may be explained by the lack of a trained individual to guide the encounter, our vast sample size, and that a large number of patients only received a phone visit. In addition, these visits were out of necessity during a pandemic for patients who are accustomed to relatively easy access to in-person visits. Studies by Buvik et al., 17 Chaudhry et al., 18 and Haukipuro et al. 20 included patients in remote locations thereby alleviating their extensive commute, which may have improved satisfaction rates. The addition of a video connection may have increased satisfaction rates for these patients, as the visit may have more closely simulated an in-person visit. Finally, the average age of patients who completed the survey was significantly higher than the average age of patients who received the survey, which again may have influenced satisfaction rates. Recent trends have demonstrated a decrease in overall response rates for surveys, especially for younger men. 22
With regard to physical examination, 27.4% of patients did not think that telemedicine could simulate a physical examination similar to that of an in-person visit. Multiple studies have looked at the validity of using telemedicine to simulate a physical examination and noted excellent results. 23 –28 When looking at adolescent postoperative knee arthroscopy follow-up, Abel et al. found that evaluation of range of motion, incision color, and effusion size was similar between telemedicine and in-office visits. 24 Bradley et al. demonstrated no significant difference between the overall diagnostic effectiveness of telemedicine versus in-office visits for rotator cuff tears. 27 Furthermore, Owusu-Akyaw et al. determined that a (patient) self-administered examination was actually more accurate than a traditional standardized clinical examination for femoroacetabular impingement syndrome. 28 This highlights a potential education gap. Patient satisfaction rates with and the eagerness to use telemedicine may be increased if patients knew that telemedicine is able to closely simulate an in-person physical examination. Standardized physical examinations will continue to be developed and validated, which may improve patient confidence. 29 As mentioned previously, a large proportion of our patients only received a phone visit, which may have negatively affected their response.
When comparing follow-up visits to new patient visits, patients presenting for follow-up were more confident that the physician reached the correct diagnosis, more strongly agreed that the care received was the same as an in-person visit, and had higher overall satisfaction. This correlates with a study by Hurley et al. who noted that more physicians preferred to use telemedicine for postoperative visits compared with new patient visits, citing a lack of a meaningful physical examination as the main reason. 30 Patients with follow-up visits will typically have an established diagnosis, have rapport with the physician, and may not need an extensive physical examination.
When comparing video telemedicine visits with phone-only visits, patients utilizing video demonstrated a higher overall satisfaction, were more comfortable scheduling surgery, more strongly agreed that the physician was able to simulate a physical examination similar to an in-person visit, were more confident that the correct diagnosis was reached, and that care received was the same as an in-person visit. A systematic review by Rush et al. noted that video offers improved provider diagnostic accuracy and reduced readmission rates compared with phone visits. 31 Although video telemedicine does not replace an in-person encounter, it can be assumed to more closely simulate an in-office visit.
Older patients were more likely to schedule a phone visit; however, there was no difference in comfort scheduling surgery compared with younger patients. Statistical analysis demonstrated a discrepancy between average satisfaction score, which revealed no difference, and percent reaching top box score, which showed that younger patients were more satisfied with telemedicine. The video component of our telemedicine system requires either a smartphone or computer/laptop with video capabilities, and anecdotally some of our older patients were not comfortable with the process. However, this did not lower their average overall satisfaction, possibly due to the convenience of not needing to travel or be exposed to others. Older patients may be more amenable to telemedicine on average, while younger patients were more polarized to the lack of an in-person visit.
The authors acknowledge that since the COVID-19 pandemic there have been other additional studies examining patients' perceptions of telemedicine during this unprecedented time. 32 –34 However, our study presents results from a large diverse cohort, much larger than most comparable studies. Furthermore, this study can only help to reinforce and add to the literature regarding such a unique period. There is no guarantee that a similar pandemic will not occur in the future. With the return to mainly in-person visits for the majority of the orthopedic world, limited additional studies regarding COVID-19 and telemedicine can be carried out.
Rapid adoption of telemedicine in orthopedic surgery as a result of the SARS-CoV-2 pandemic was born out of necessity. Lockdown forced the cancellation of in-person office visits, accelerating the implementation of virtual visits. Although the majority of visits at our institution have returned to in-person, this brief transition may have shown us the value and capabilities of telemedicine within orthopedics. A significant percentage of our patients would have sought treatment elsewhere had we not offered telemedicine visits, which demonstrates the importance of having telemedicine as an option in the future. The extent to which telemedicine will be incorporated into orthopedics is yet to be determined, however, with more studies and guidelines implemented regarding its use, telemedicine may play a significant role in the future of orthopedic surgery.
Limitations
This study has several limitations. First, as with any survey-based study it is subject to inherent responder bias. It is possible that patients who were either very satisfied or unhappy with the experience may have been more likely to respond. Second, we distributed the survey to a large number of patients to increase feedback at the cost of response rate. The survey was distributed through electronic mail and the response is thereby limited by junk mail filters and noncompliance. Although our response rate is generally low, we had a large number of diverse respondents. In addition, the survey was distributed in July, which may have been several months after a patient had his or her actual telemedicine visit leading to recall bias. Finally, the survey was conducted during a pandemic. The results may not translate to future perceptions about telemedicine once travel restrictions and social distancing recommendations change. However, the data were gathered during an unprecedented time, which may be valuable should in-office visits be limited in the future for any reason.
Conclusions
Overall, satisfaction rates are high for orthopedic patients undergoing telemedicine visits, with high confidence in coming to the correct diagnosis, as well as comfort level in scheduling surgery. Patients are more confident in telemedicine when presenting for a follow-up visit rather than a new injury. If possible, video telemedicine should be utilized over phone visits.
Footnotes
Authors' Contributions
A.M.O.: Conception, data acquisition and analysis, drafting of the article, and final approval of the article. C.L.A., J.Z., A.J., and J.C.: Data interpretation and analysis, drafting of the article, and final approval of the article. G.R.K. and F.G.A.: Data interpretation and analysis, critical revision of the article, and final approval of the article. J.D.K.: Conception, data interpretation and analysis, drafting and critical revision of the article, and final approval of the article.
Disclosure Statement
A.M.O., C.L.A., J.Z., A.J., and J.C.: None. G.R.K.: American Academy of Orthopedic Surgery—Committee Member, New Jersey Orthopaedic Society: Board or committee member, paid consultant Zimmer Biomet, Royalties Zimmer Biomet, paid consultant Corentec USA. F.G.A.: American Orthopaedic Society for Sports Medicine: Board or committee member; American Shoulder and Elbow Surgeons: Board or committee member; Integra Life Sciences: Paid presenter or speaker; Integra Life Sciences: Paid consultant; New England Shoulder and Elbow Society: Board or committee member; New Jersey Orthopaedic Society: Board or committee member; NewClip USA: IP royalties. J.D.K.: Clinical Spine Surgery: Editorial board, CreOsso: OP royalties; Jaypee Publishing: Royalties; Medtronic: Research support.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.