
Abstract
Introduction:
Telemonitoring technologies enable medical teams to remotely manage outpatients with heart failure (HF) and reduce their risk of HF-related hospitalizations. However, noncompliance threatens the effectiveness of these approaches. This review aims to identify whether patients who are less likely or unable to comply with telemonitoring and their instructions for use are represented by interventional telemonitoring studies, and if their exclusion from studies is resulting in study findings not representative of clinical reality.
Methods:
A narrative literature review was conducted to identify interventional telemonitoring studies reporting compliance rates for HF patients. A search of PubMed and Medline databases identified eligible studies published between January 2000 and June 2021.
Results
: Twenty-five (n = 25) eligible studies with an interventional study design were identified. Reported compliance with telemonitoring ranged between 37% and 98.5%; however, 72% of studies reported good or medium compliance. A majority (76%) of studies had exclusion/inclusion criteria favoring the enrollment of patients who may be more likely to comply with telemonitoring and their instructions for use. Forty percent of studies had a sample with a mean or median age of <65 years. Participants were more likely to be male (majority in 92% of studies) and white (majority in 78% of studies that reported ethnicity).
Conclusion:
Compliance rates reported by current studies are unlikely to be generalizable to the wider HF population, particularly patients who are less likely or unable to comply with telemonitoring. Studies are therefore likely overestimating compliance rates. Future innovation should focus on designing “low compliance” solutions that require minimal engagement from users and future studies should aim to recruit a more generalizable cohort of patients. To achieve a more standardized metric of compliance, studies should report compliance (however defined) achieved by the 25th, 50th, and 75th percentile of all patients enrolled.
Introduction
Heart Failure, Telemonitoring, and Compliance
The prevalence of heart failure (HF) is increasing worldwide partly because of better treatment for conditions that predispose to HF development, for instance, hypertension, diabetes, and myocardial infarction, and partly because of the availability of many therapies that prolong survival in those who develop HF. 1 –3 An estimated 6.2 million American adults ≥20 years of age had a diagnosis of HF between 2013 and 2016, up nearly 9% compared with prevalence between 2009 and 2012. 2 HF is therefore a significant public health problem, affecting an estimated 64.3 million people worldwide. 4 The rate of HF hospitalizations also remains substantial. 1,5 In the United States and Europe, hospitalized HF represents 1–2% of all hospital admissions. 1 Reducing preventable hospital admissions has therefore become a priority in the treatment and management of HF. 5
Technological advancements and the development of telehealth has facilitated and enabled the remote monitoring and management of patients with HF. 6 HF patients are advised to manage their condition as a way of controlling their symptoms for as long as possible 7 by focusing on adherence to a range of self-care behaviors, including symptom monitoring, taking medications, and lifestyle modification. 8,9 A recent meta-analysis found that noninvasive telemonitoring significantly reduces the risk of all-cause mortality and HF hospitalization in HF patients. 10
These technologies are not seeking to replace current care for HF patients, but rather provide an option that is as good as current care but potentially more convenient for patients and more cost effective for the health care system. In addition, patients living in small and isolated rural areas travel further and longer to see a medical specialist compared with their urban counterparts. 11 Remote monitoring of patients therefore has the potential to increase access to services for patients living in rural areas, reducing travel costs and practical inconveniences. 12
However, a drawback of telemonitoring technologies is that they usually require patients to comply with instructions to initiate data collection. Despite wearables and Bluetooth technology offering a means to facilitate their use, they do not eliminate the requirement for compliance with the technology itself. Even invasive telemonitoring technologies such as implantable continuous hemodynamic monitors (ICHMs) require a level of compliance from patients. For example, the Chronicle™ ICHM requires patients to transmit the stored information using a home monitor, 13 and the CardioMEMS™ system requires patients to lay on a pillow-like electronic system to initiate the transmission of sensor readings. 14
Some of the factors that are known to be related to compliance with HF self-care regimes include age, gender, existing comorbidities, memory impairment, educational level, and depressive symptoms. 15,16 The available evidence supporting the relationship of each of these factors directly with telemonitoring is varied; however, these factors and others, such as technical ability, may also be important in compliance with telemonitoring and their instructions for use. Indeed, some patients are less likely to comply with telemonitoring and their instructions for use, while others may be unable to comply altogether (e.g., in the case of dementia, including Alzheimer's disease).
Previous reviews have described compliance rates across studies 17 or have explored the reasons for refusal to participate or withdraw from using telemonitoring technologies. 18 However, no other review has sought to explore whether these patients who are less likely or unable to comply with telemonitoring are represented in the current telemonitoring literature. This is important because the mean number of hospitalizations is significantly higher for low adherence telemonitoring patients compared with high adherence patients. 19 The cost of hospitalization for poorly compliant HF patients with home telemonitoring is also reportedly $66,530 compared with $23,689 for highly compliant patients among Medicare outpatients in the United States. 19 If these patients are not being represented by the current literature, then it may suggest that an important patient group is being overlooked.
Objective
This review has two key objectives: (1) to summarize compliance results reported by telemonitoring studies and (2) identify whether patients who are less likely or who are unable to comply with telemonitoring and their instructions for use are represented by telemonitoring studies and if their exclusion from studies is resulting in study findings that fail to match real-world experience.
Methods
A literature search was conducted to identify studies that reported compliance outcomes with telemonitoring in HF patients. A search of PubMed and Medline databases was performed by the author (R.B.) in June 2021 to identify eligible studies published between January 2000 and June 2021. Other limits included studies published in English. Studies were eligible if they reported compliance or adherence outcomes with telemonitoring in HF patients, and with full-text available through open-access or institutional access online. Eligible studies were those with an interventional study design and therefore were not limited to randomized controlled trials alone. Single-arm studies were eligible since the focus of the review is on compliance with the telemonitoring intervention. The search strategy incorporated the search terms and relevant MeSH terms: “compliance,” “adherence,” “telemonitoring,” “remote monitoring,” “home monitoring,” and “heart failure.” The references of eligible studies and published systematic reviews were also searched to identify any additional studies.
For the purpose of this review and ease of interpretation, studies were categorized into low (dark gray), medium (medium gray), or high (light gray) according to the compliance results they reported. This was performed by the primary author (R.B.). There are no available guidelines outlining compliance thresholds with telemonitoring; however, a threshold of 80% is used to define adherence with exercise and medication taking among HF patients. 20 Therefore, studies were categorized as high compliance if reported compliance was ≥80%. A subjective threshold of 60–79% was decided by the authors to signify medium compliance and <60% to signify low compliance. Where studies provided multiple compliance results based on different definitions for example, 4 days versus 6 days or one measure versus two, the lower compliance estimate was always extracted. If studies also provided two results for example, one for blood pressure and one for weight, then the lower estimate was also chosen. By taking the lowest reported compliance estimate it ensured that the poorest compliance measure was always considered.
This information, along with a description of the telemonitoring intervention, study type, duration, and sample size, was extracted and organized in a table to provide a summary of telemonitoring studies and their reported compliance. Compliance rates were then reviewed across the categorized studies to gain an overview of compliance with current telemonitoring technologies to respond to the first objective of this review.
To respond to the second objective of this review, the inclusion and exclusion criteria of studies and their study sample were critically evaluated to assess the generalizability of their study findings. Therefore, information regarding notable inclusion/exclusion criteria and potential predictors of compliance, which included the mean age of participants, % of female participants, ethnicity of participants, and ejection fraction (EF) of participants, were extracted and organized in a table. Analysis of the extracted data included identifying any observational biases between either study inclusion/exclusion criteria or potential predictors of compliance and whether the study reported high, medium, or low compliance. This analysis was performed by the authors and was displayed in a table format.
Results
A search of PubMed and Medline databases, with an additional search of reference lists and other systematic reviews, identified 25 eligible studies to include in the narrative literature review (Fig. 1). A summary of study characteristics and reported compliance rates reported by studies are summarized in Table 1.
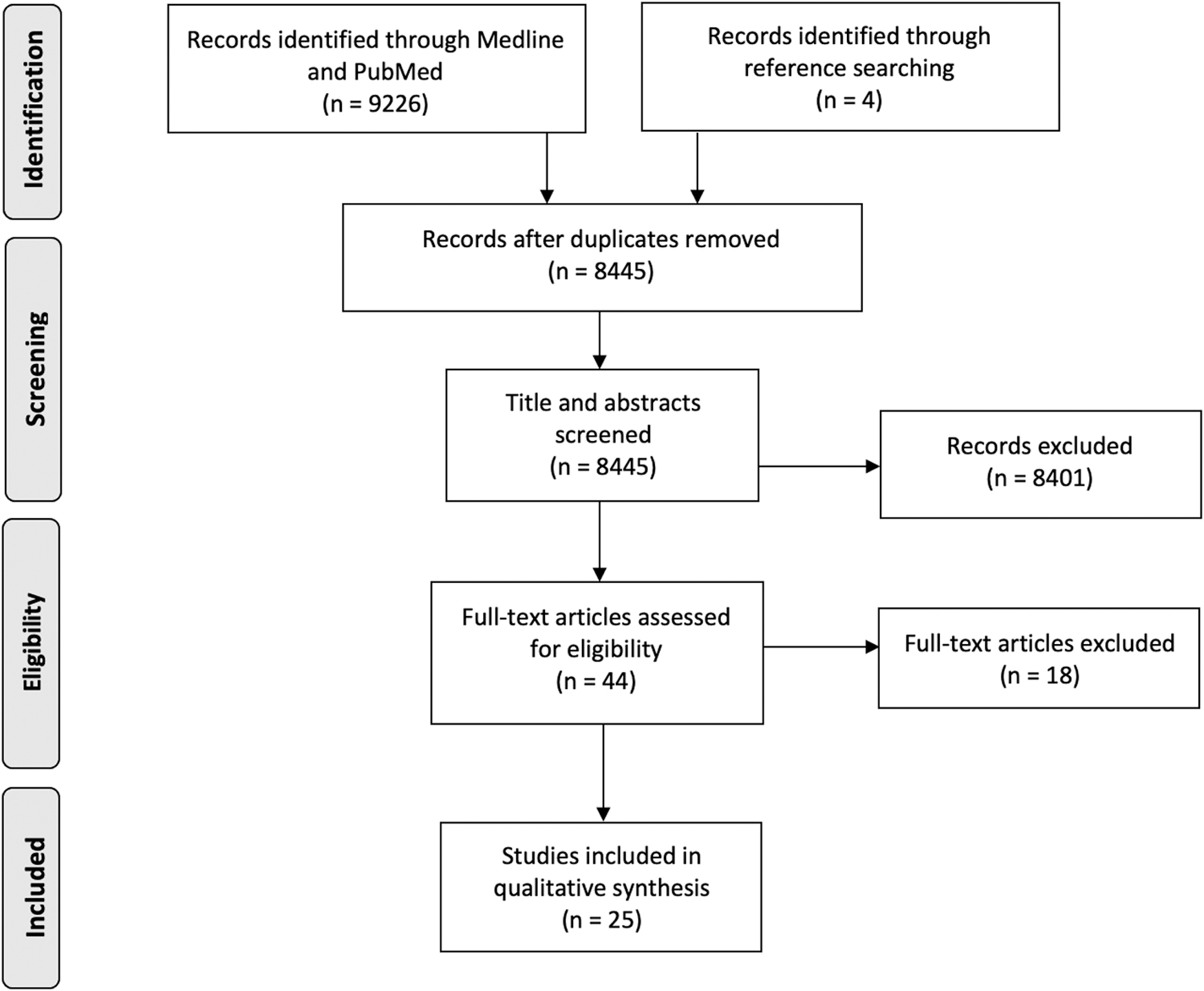
Flowchart adapted from Moher et al. 72 summarizing the results of the literature search.
Summary of Studies and Reported Compliance Results
Gray coded according to high compliance (light gray), medium compliance (medium gray), and low compliance (dark gray).
BP, blood pressure; HF, heart failure; IVR, interactive voice response; RCT, randomized controlled trial; SBP, systolic blood pressure.
Reported Compliance with Telemonitoring
Reported compliance results with telemonitoring were heterogeneous, ranging between 37% 21 and 98.5% 22 (Table 1). Six 9,23 –27 of the included studies measured compliance as a proportion of time patients were compliant over the study period, whereas 12 19,22,28 –37 measured it as the proportion of participants who were compliant by a particular definition of the study. Four studies used a measure of compliance based on the proportion of planned responses or submissions fulfilled by participants 38 –41 and three provided no detail about their measure of compliance. 42 –44 The average study length was around 9 months, with the shortest being just 30 days 23 and the longest being 4 years. 26
To provide an overview of reported compliance in this review, 10 studies were categorized as reporting “high compliance” (≥80%), 8 studies “medium compliance” (60–79%), and 7 studies “low compliance” (<60%) (Table 1). However, studies were heterogeneous in their definition of what was considered “compliant” and “noncompliant.” For example, Seto et al. 30 considered the submission of at least 80% of telemonitoring measurements as “compliant” while Nanevicz et al. 23 considered at least 20 uploads over 6 months to be “compliant.”
A notable finding by Cleland et al. 31 was an observed decline in compliance from 81% to 55% with the addition of one daily measurement (weight or blood pressure) from patients. As a result, this study was categorized as reporting “low compliance” due to the joint measurement of weight and blood pressure. Other studies also reported lower compliance with an increasing number 9,31 or frequency 33 of measurements required from patients. The TELE-HF trial found that by the last week of their study, only 55% of patients were still using the telemonitoring system at least three times a week. 32 Ware et al. also reported that compliance declined to 63.1% after 12 months in their single-arm study and that time was a significant predictor of adherence, with each month since study enrollment accounting for a 1.4% decrease in adherence. 9
In addition, seven studies reported findings of patients refusing to comply, withdrawing, or never utilizing the telemonitoring technology. Blum and Gottlieb reported that one participant declined to accept the telemonitoring technology 26 and Cleland et al. reported that 7.1% declined to comply with regular telemonitoring altogether. 31 One study also reported 12 never-beginners out of 54 participants 41 and in another, 3 participants had no recorded weights. 43 Eighteen percent of participants were considered dropouts in Capomolla et al. 38 and 17% did not use the telemonitoring equipment in the BEAT-HF trial. 27 The TELE-HF study that included 826 participants also reported that 14% never used the system. 32
Inclusion and Exclusion Criteria
Notable exclusion/inclusion criteria of studies and the characteristics of included participants are summarized in Table 2. These include the exclusion of patients living with Alzheimer's or dementia, cognitively impaired patients and patients with poor technical ability. Four studies excluded patients living with dementia or Alzheimer's 24 –26,43 and five excluded patients who were cognitively impaired or cognitively impractical (Table 2). 27,28,33,34,39 Of the four studies that excluded specifically patients living with Alzheimer's or dementia, not one study reported low levels of compliance with telemonitoring (Table 3). However, studies that excluded cognitively impaired/impractical patients reported both high and low levels of compliance (Table 3).
Notable Exclusion/Inclusion Criteria and Key Characteristics of Participants Per Study
AA, African American; AC, African Canadian; EF, ejection fraction; SEA, South East Asian.
Compliance Categories of Studies That Have Excluded Participants or That Have a Biased Sample of Participants Based on Potential Predictors of Reduced Compliance with Telemonitoring
Six studies selected participants based on their technical ability to be able to comply with telemonitoring (Table 2). 9,19,40 –42,44 This included assessing patient's technical skills, 40 testing patient's ability to perform a variety of telemonitoring competency tasks, 19 a digital aptitude test 44 and excluding patients unable to use a weighing scale, 43 understand text prompts, 9 or read a phone display. 41 All six of these studies reported high or medium compliance rates with telemonitoring (Table 3).
Three studies also excluded patients who were considered physically impractical or physically impaired to carry out telemonitoring. 27,34,39 The TELE-HF trial also used “enthusiasm” as a criterion in the selection of medical practices used to recruit HF patients (Table 2). 32 Two studies also excluded patients deemed unable to comply 31 or who were judged to be “inappropriate,” 29 but did not provide any further detail as to which groups of people this specifically applied to (Table 2). Overall, 76% of studies had an exclusion/inclusion criteria that favored the selection of more compliant patients.
Study Sample
Twenty-three (92%) of the included studies included mostly male participants, and in some of these studies, the male majority was overwhelming (Table 2). Of those studies that reported sex, the average proportion of males per study was 66%. For example, in Capomolla et al. 38 and Vuorinen et al., 40 only 7.4% and 17% of participants, respectively, were female, and only 2 studies had a larger female representation than male. 36,42 The majority (74%) of the studies that included a male majority in this review also reported high and medium levels of compliance (Table 4).
Compliance Categories of Studies According to Whether They Recruited a Male or Female Majority
Ten of the included studies had a sample of HF patients with a mean or median age of <65, ranging from 46.344 years to 63.434 years (Table 2). Studies with younger (<65 years) and older (≥65 years) participants both appeared to report a similar distribution of compliance results (Table 5). However, of the nine studies with a mean age of ≥70 years (Table 6), eight reported good or medium compliance results but seven of these eight had excluded patients with Alzheimer's, cognitive impairment, or those not technically competent (Table 6). Studies also appeared to be biased toward the recruitment of white participants (Table 2), with only one study focusing solely on the black and Hispanic HF population. 35 Of the nine studies that reported the ethnicity of their participants (Table 2), seven studies contained a white majority. 9,22,26,27,30,32,42
Compliance Categories of Studies According to Whether They Recruited Younger or Older Participants
Compliance Categories of Studies with a Mean or Median Participant Age ≥70 Years According to Their Exclusion Criteria
Discussion
Of the 25 studies included in this review, compliance rates ranged between 37% and 98.5%. These findings are mostly in line with a previous review on compliance with home-based telehealth projects for multiple chronic conditions where compliance rates ranged between 40% and 90%. 17 However, it must be noted that varying measures of compliance were utilized by studies depending on the type of telemonitoring procedure and what level of interaction and engagement was expected from patients. Without a standardized measure of compliance, drawing comparisons between studies and summarizing overall compliance with telemonitoring is challenging.
Nevertheless, several studies reported a decline in compliance with an increasing number or frequency of measurements required from patients. This suggests that the more patients are expected to engage and interact with telemonitoring, the less compliant they may be. Interestingly, these findings are aligned with those for medication adherence in HF patients, where the risk of poor medication adherence is significantly greater with a higher number of total daily medications. 45 Like medication taking, telemonitoring requires compliance over a long time from HF patients. However, telemonitoring may often require the recording and submission of multiple vital parameters, which may be more time consuming for patients than taking medication. This review therefore highlights that noncompliance is likely to be an even greater issue with telemonitoring technologies.
Both Chaudhry et al. and Ware et al. also reported a decline in compliance over time. As noted by Chaudhry et al., these findings are of significant importance given that considerable resources are utilized by these studies to optimize patient engagement with telemonitoring. 32 In a real-world setting, where these resources are not available, and patients are not monitored in a controlled study setting, noncompliance is likely to be a more prominent issue than implied by these studies.
On average, compliance is being measured by the studies in this review for a short time relative to the average lifespan of HF patients and therefore may not be reflective of compliance with longer-term use of telemonitoring technologies. The average lifespan of HF patients from the point of hospital discharge is reported to be five and a half years 46 ; however, the longest study in this review was 4 years 26 with a median of 6 months in length. Assuming the 2% per month drop in compliance observed by Ware et al., 9 over 5.5 years, even perfect initially observed compliance would be expected to drop to 26%. Chronic long-term noncompliance is therefore to be expected, rather than uncommon.
The finding that 14% of participants never used the telemonitoring technology in the TELE-HF trial is also alarming. 32 TELE-HF is the largest study included in this review by a substantial margin, thus we may assume that noncompliance with telemonitoring is a problem that exists but is not being widely reported by studies. A systematic review looking at studies that have reported rates of refusal/withdrawal from telehealth also found that almost one-third of patients offered telehealth refused, and 20% of participants who did accept later abandoned telehealth. 18
Interestingly, the studies in this review that excluded patients living with Alzheimer's or dementia did not report low levels of compliance with telemonitoring. Dementia is a common symptom of Alzheimer's disease 47 and memory loss is a symptom of both dementia and Alzheimer's disease. Memory impairment is significantly associated with poorer adherence to HF self-care behaviors. 48 Considering that these studies excluded a patient group likely to be noncompliant with telemonitoring, it is unsurprising that low compliance was not reported by any of these studies.
It must be noted however that many studies may have excluded patients living with dementia, including those living with Alzheimer's disease, due to the ethical challenges of including them in a trial. As outlined by the Declaration of Helsinki, researchers have a clear obligation to obtain consent from individuals participating in research. 49 Providing informed consent requires cognitive skills, which gradually deteriorate in patients living with dementia or Alzheimer's. Obtaining informed consent from this patient group is therefore challenging, and in some cases may be impossible to obtain. 49 In the United States, Institutional Review Boards have strict requirements for obtaining informed consent and this process is heightened when including patients living with dementia or Alzheimer's. 50
Both high and low compliance was reported by studies that excluded cognitively impaired/impractical patients. Research has demonstrated that HF causes cognitive impairment through a variety of direct and indirect mechanisms, and the prevalence of cognitive impairment in HF patients is significant, reported to range from 25% to 75%. 48,51 Among HF patients with no history of dementia, poorer cognitive function is a predictor of reduced medication adherence in these patients. 52 Based on these findings, compliance with telemonitoring is likely to be a challenge for cognitively impaired HF patients who may be unable to actively engage with these technologies and follow instructions.
A distinction must be made between these patients who cannot follow instructions and are thus inevitably noncompliant, with those who can follow instructions but are still noncompliant. Patients living with Alzheimer's, dementia, or cognitive impairment who cannot follow instructions present a particular challenge for telemonitoring technologies. For some of these patients, carers or family members may help overcome any issues with following instructions. However, in the United States, estimates indicate that one in three patients living with dementia and at least one in seven patients living with Alzheimer's live alone. 53 Suggested strategies to improve compliance such as empowerment and education 54 will therefore likely not work on this patient group.
Several studies also selected participants based on technical ability, thus knowingly excluded patients who are highly likely to be noncompliant with telemonitoring. Unsurprisingly these studies reported high to medium levels of compliance. For example, Nouryan et al. selected participants who had previous experience using telehealth technology, therefore, only testing the intervention on those familiar with telehealth and thus technically able. 19
The TELE-HF trial also used “enthusiasm” as a selection criteria and Koehler et al. excluded patients with severe depression. Around one in five HF patients have depression and these patients are 2.3 times more likely to report medication nonadherence compared with nondepressed patients. 55,56 Koehler et al. reported excellent compliance levels of 97% having excluded these patients. 37 Based on these findings, it is also unlikely that depressed HF patients would have been selected for the TELE-HF trial, despite depression being prevalent among HF patients. Depressed patients may also not enroll or choose to participate in these studies due to their condition.
The bias toward including mostly male participants in studies is also concerning. While this may be a normal occurrence in trial design, the more a clinical trial population diverges from the real-world population, the less we can rely on the results to inform real-world care. A 2018 study on a range of chronic conditions, including HF, reported that male patients maintained a higher level of adherence with telemonitoring than females over time. 57 A majority (74%) of studies that included a male majority in this review also reported high and medium levels of compliance. These findings are also in line with reported hospital admission rates in the United States; between 2004 and 2001, more females were hospitalized with a primary or secondary diagnosis of HF than men (53.5% of hospitalizations were in women). 58 The suggestion that males may be more compliant than females is perhaps, surprising; however, a study by Kerby et al. on blood pressure telemonitoring also reported higher male adherence. 59
The gender bias could be explained by another bias in the literature. There are notable gender differences in the etiology of HF, with men more likely to develop HF with reduced ejection fraction (HF-REF) than women. 60 Of the 22 studies that reported the EF of participants, 45% included only HF patients with an EF ≤40%, which is a diagnosis of HF-REF, and another 23% reported a majority of participants with an EF of ≤40% (Table 2). With the majority of studies biased toward recruiting HF-REF patients, this may explain the overall bias observed toward male recruitment.
The underinclusion of women in clinical trials is recognized as a barrier to understanding sex-related differences in HF outcomes. Many pharmacological therapies for the treatment of HF, such as beta-blockers, have mostly been performed on male HF patients. 61 As a result, there is consistently insufficient reporting of sex-specific HF and cardiovascular outcomes. 61,62 This has implications for the effective translation of research into clinical practice and may result in ineffective treatments and interventions being delivered to women. 62
Another concern is the mean age of participants included in these studies. HF is a disorder of the elderly, mainly affecting individuals ≥65 years, 63 yet ten studies had a sample with a mean or median age below 65. Older age is reportedly a negative predictor of follow-up appointment keeping, medication taking, lifestyle changes, and overall compliance of HF patients with treatment. 64 However, contrary to these findings, Ware et al. reported that adherence with telemonitoring was higher with each increasing age category such that older patients maintained higher adherence over time. 9 These findings are surprising given that a common reason for lower compliance among the elderly is forgetfulness and cognitive impairment. 64 It is important to keep in mind that Ware et al. excluded patients based on technical abilities, so these very same patients may well have been excluded.
Nevertheless, there appeared to be no clear bias in the literature between the compliance results of studies and whether their mean age was above or below 65 years.
It has also been acknowledged that older HF patients over the age of 70 are underrepresented in HF studies. 65 A systematic review by Inglis et al. identified a notable bias toward the recruitment of younger HF patients, with only 33% of telemonitoring studies in their review using a sample with a mean age over 70 years. 66 The studies included in this review corroborate these findings, with 36% of studies including patients with a mean age of 70 years or above. However, of the studies with a mean sample age of 70 years or above, the majority reported good or medium compliance. However, most of these studies had excluded potentially noncompliant patients. The bias toward recruiting mostly white participants is also concerning given that black patients have the highest risk of HF-related death, yet these patients are barely represented by the majority of telemonitoring studies. 67
Strengths and Limitations of Studies and Review
A strength of the studies included in this review was that they reported compliance results that could be extracted. In addition, studies originated from a range of countries, including the United States (8 studies), Europe (10 studies), Canada (2 studies), Asia (3 studies), and Australia (2 studies). A major limitation, however, is the heterogeneous measures of compliance and a lack of consistent reporting of compliance by studies.
Since most patients are compliant, trial results do reflect the majority of HF patients thus it is unsurprising that researchers and trial sponsors focus on these patients. Due to the nature of clinical trials and those with an interventional study design and the behavioral limitations of noncompliant patients, it is also challenging to include potentially noncompliant patients in trials when evaluating telemonitoring technologies. However, those who are hospitalized repetitively at the cost of the health care system are frequently those who do not do as their doctors say. The findings from these studies and their generalizability to the HF population should therefore be treated with caution, given that an important portion of the HF population was not represented.
A strength of this review is that a substantial number of studies reporting compliance with telemonitoring in HF patients were identified and included in the narrative synthesis. Findings were, therefore, summarized narratively without doing a meta-analysis. A limitation is that the categorization of the studies in this review by compliance was subjective, and it is acknowledged that this categorization would likely differ depending on the author. It is also acknowledged that this categorization is limited by the results that were disclosed by studies and the definition of compliance that they used. This review also only searched two databases and is therefore not a systematic review. Additional searches of other databases could have revealed additional eligible studies.
Conclusion
The utilization of telemedicine is increasing rapidly in the United States. According to the American Medical Association, telemedicine insurance claims increased by 53% from 2016 to 2017. 68 COVID-19 has also accelerated the shift toward virtualized health care, which is transforming the delivery of health care in the United States. 69 The remote nature of telemonitoring is thus well aligned with the future direction of health care. Moreover, telemonitoring management alongside usual care for discharged patients with HF is reportedly more cost effective than usual care alone in the United States. 70
However, understanding compliance within the context of current studies is challenging. What is apparent is that noncompliance with telemonitoring technologies is a problem. However, while some studies are reporting this, the majority are reporting high or medium compliance results. Overall, 76% of studies had an exclusion/inclusion criteria that favored the selection of more compliant patients. It is, therefore, unsurprising that overall reported compliance rates are high to medium across the majority of studies. It suggests that current studies overestimate compliance with telemonitoring and their instructions for use in the real world. This is unsurprising given that these studies are trialing telemonitoring technologies that require patients to be able to follow instructions. However, this has implications for patients as telemonitoring technologies continue to cater for the more compliant population.
Noncompliant patients appear to consist of two groups; those who can follow instructions but remain noncompliant and those who cannot follow instructions. For the latter, for example, patients living with dementia, including those living with Alzheimer's disease, telemonitoring technologies demand an unachievable level of engagement and compliance, with no reasonable expectation of improvement in engagement and compliance. Noncompliant patients, whether they can follow instructions or not, place a financial burden on the health care system.
This review has therefore demonstrated the significance of current gaps in the evidence surrounding compliance with telemonitoring technologies and is the first review to directly explore the issue of noncompliance with telemonitoring in HF patients. This review hopes to inform the future innovation of telemonitoring technologies to ensure the consideration of noncompliant patients in their design. This is important in the battle to reduce the number of preventable hospital admissions among HF patients and the associated cost of hospitalization. This review also highlights the lack of inclusion of important HF groups in current telemonitoring studies and thus further supports other studies in the literature that continue to raise the concern that there is a lack of diversity in cardiovascular studies. It is important that this issue is addressed to ensure the best delivery and practice of HF care.
Recommendations for Future Research and Innovation
Telemonitoring technologies need to work for all patients and take into consideration the behavioral and physical limitations of many, particularly the most frail and high-risk patients. Therefore, the following recommendations for future research innovation are as follows:
Technological Innovation
A shift in focus is required toward the innovation of “low compliance” technologies rather than attempting to enhance patient compliance with existing ones.
Novel developments in artificial intelligence and sensing technology could provide such solutions by reducing the need for patient engagement.
“Low compliance” technologies should take into consideration the behavioral limitations of most patients and therefore should:
○ Demand very minimal engagement from users that is, minimal time and frequency interacting with the technology.
○ Not require a high level of technical ability to use the technology successfully.
○ Should be able to fit around the patient's day-to-day life that is, minimal disruption to a patient's day-to-day routine. The success of telehealth approaches is in part dependent on the extent to which they managed to fit with patients' needs, skills, and daily life. 71
Future Studies
Studies should aim to improve the generalizability of their findings to the wider HF population. They should therefore aim to recruit a more balanced cohort of patients. This includes recruiting more female patients, older patients, patients living with comorbidities such as Alzheimer's or dementia, HF-REF patients, and ethnic minorities.
Due to the diversity of telemonitoring technologies, it is perhaps unrealistic to hope for an agreed standard metric for compliance to report against. However, reporting the fraction of patients excluded or declining enrollment, alongside the level of compliance (however defined) achieved by the 25th, 50th, and 75th percentile of all patients enrolled, would give a much clearer indication of the range of outcomes achieved for a meaningful body of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.