
Abstract
Introduction:
The Pacific Asynchronous TeleHealth (PATH) system is an asynchronous provider-to-provider teleconsultation platform utilized by military medical facilities throughout the Western Pacific Region. This study focused on PATH utilization for pediatric cases and its impact on patient transfers and cost avoidance.
Methods:
This retrospective analysis reviewed PATH cases from March 2017 to February 2020 for patients aged 0–17 years. We reviewed the referring users' responses to survey questions related to the impact of PATH consultation on patient travel for in-person subspecialty care and the need for local referral. Data for cost avoidance were estimated using per diem rates and airline flight costs for Fiscal Year 2020.
Results:
A total of 2,448 pediatric consultations were submitted from 29 military medical facilities. Pediatric Pulmonology (n = 557, 24.5%), Pediatric Cardiology (n = 446, 19.6%), and Pediatric Neurology (n = 236, 10.37%) had the highest percentage of pediatric teleconsults. Approximately 42% of referring users completed the survey questions. Among survey respondents, 710 (69.4%) indicated that unnecessary patient transfers were prevented, equating to a cost savings of ∼$3.3 million.
Conclusions:
We observed robust utilization of the PATH system by pediatric providers in the Military Health System that ultimately resulted in substantial cost avoidance. This asynchronous telemedicine platform is a vital asset in locations with limited access or travel restriction to medical specialists, such as during pandemics.
Introduction
Asynchronous (store-and-forward) telemedicine supports remote consultation, evaluation, diagnosis, and treatment recommendations using secure technology that complies with the Health Insurance Portability and Accountability Act (HIPAA). Additionally, published data demonstrate the substantial economic benefits of telemedicine. 1,2 U.S. military medical providers have capitalized on telemedicine to conduct interprofessional consults for more than 30 years. Given the global area of operation of the U.S. military, access to highly reliable clinical guidance for patient care is essential to the mission capability and supporting military families.
Tripler Army Medical Center (TAMC), located on the island of Oahu (Hawaii), serves as the U.S. military's tertiary medical referral center for the Pacific Region, which includes Japan, South Korea, and Guam (Fig. 1). In 2004, TAMC developed a teleconsultation platform to provide pediatric subspecialty provider-to-provider advice using a locally developed program called the Pacific Asynchronous TeleHealth (PATH) system. 2 This platform was initially created to support primary care providers overseas who have limited access to pediatric subspecialty advice for routine clinical cases. Over time, it was expanded to cover subspecialty consultation to adults. PATH has demonstrated that it can improve access to subspecialty care while decreasing cost burden to the Department of Defense (DOD) for routine medical evaluations. 2,3 Such a system allows for HIPAA-compliant, routine provider-to-provider communication that removes the burden of real-time synchronous communication across numerous time zones; it is currently utilized by more than 30 military treatment facilities. 2,3
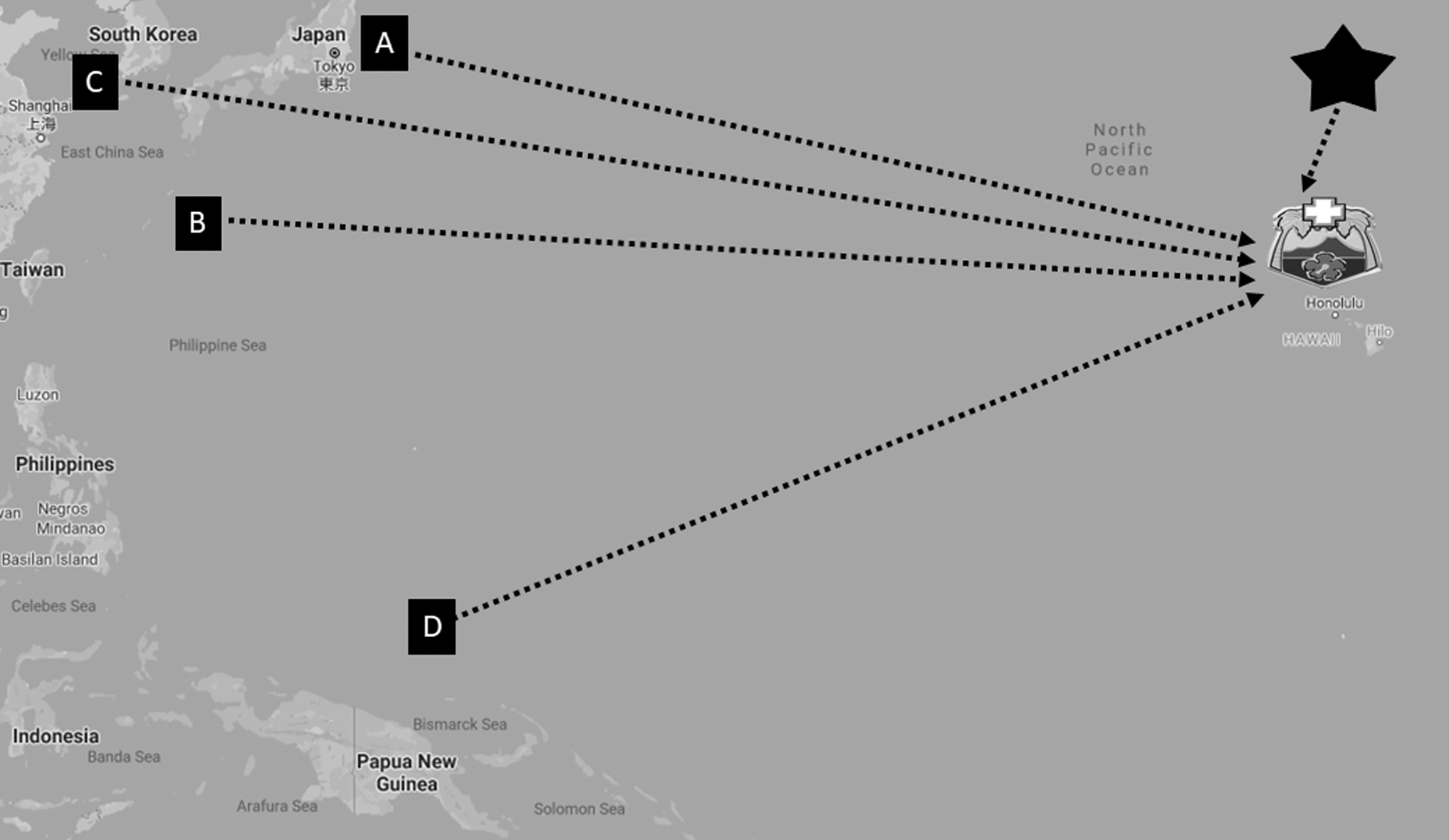
Military treatment facilities in the Pacific, which send PATH teleconsultations to Tripler Army Medical Center.
FUNCTIONALITY OF THE PATH SYSTEM
After securely logging in to the PATH home page, a clinical provider at the originating site submits a patient query for specialist consultation including all pertinent patient information and any associated media, including photographs in JPEG format, scanned documents such as electrocardiograms, pulmonary function tests (PFTs), external laboratory results in PDF format, and short video clips in MP4 format. 2,4,5 The system also allows integrated alerts on the case for radiology and cardiology technicians located at both the originating and distant sites, allowing for coordination of radiographic studies through the Picture Archiving and Communications System (PACS) to be sent to the distant site for additional review or interpretation. The teleconsultation is routed to a consult manager who directs the teleconsultation to one or more appropriate subspecialty consultants and also monitors to make sure that the consultant provides a response within 24 to 72 h. The subspecialist reviews the teleconsultation and may ask for further information and/or render advice to the remote care provider. The responses of all participating providers are logged chronologically. The PATH system operates on a secure platform using encrypted passwords for provider authentication in accordance with HIPAA requirements. TAMC informatics department maintains the PATH system on its existing servers. 2
Asynchronous telemedicine has been shown to be an exceptional technological tool to improve access to subspecialty pediatric care around the world in the literature. 6 A retrospective review of 1,000 pediatric teleconsultations from 2006 to 2009 revealed PATHs positive impact and effectiveness with regard to access, quality, and cost. It demonstrated the benefits of incorporating asynchronous provider-to-provider teleconsultation into routine pediatric practice. 2,4 Of note, this study relied on review panels to assess the outcomes and impact of each case rather than the involved clinicians. In June 2014, Navy Medicine East and the U.S. Navy Bureau of Medicine and Surgery (BUMED) launched the Health Experts onLine at Portsmouth (HELP) teleconsultation system as a module created within the PATH platform and programmatic infrastructure. The HELP platform incorporated the same operational structure with consult managers reviewing each new case submission and initially focused on providing asynchronous teleconsultations to the Atlantic Fleet, but has evolved to cover a broader footprint to now include Europe and the Middle East. In the initial 1-year review of the HELP program, it was shown to provide improved access to care and to reduce network referrals and/or medevacs to a tertiary care center with subspecialty providers. 7 In 2017, a review of HELPs return on investment showed considerable savings (both tangible and intangible) to the Military Healthcare System given the low cost of the information technology (IT) system. 8 The evaluations during the first 3 years of implementation of the HELP module highlighted not only the continued value of this platform but also the potential value of adding a simple way to assess end user experience with the system through the use of a short survey when closing a clinical case.
At the time of this study, TAMC had the highest usage and productivity as a distant site with asynchronous teleconsultation in the DOD; however, an updated assessment of the PATH system has not been published in relation to pediatric subspecialty care in over a decade. 2,9 The results of reviews performed by the HELP module managers led to the system-wide addition of two survey questions in March 2017 for the originating site provider to reply upon closing the case. The survey asked the following: (1) “Did this consult prevent patient movement (prevent unnecessary transfer to TAMC)?” (2) “Did this consult recapture care (prevent referral to facilities outside military network)?” 7,8 In this retrospective review, we provide an update regarding the utilization of PATH for pediatric cases and an analysis of the survey questions in relation to travel cost avoidance.
Methods
PATH cases initiated for patients aged 0–17 years that were generated between March 2017 and February 2020 were included in this analysis, excluding Active Duty Service Members. Data elements were collected as follows: age of patient, originating site of PATH consultation, originating site provider department (provider initiating consult), and medical subspecialty of distant site provider (provider responding to consult). Additionally, the response to the survey questions was assessed. The study protocol was approved by the TAMC Scientific Review Committee (IRB protocol # 20R18).
STATISTICAL ANALYSIS
Descriptive statistics were used to characterize submitted case volume, basic patient demographics, providers' responses to survey questions, and cost avoidance. Fisher's exact tests and chi-squared tests were used to assess differences in survey response by specific characteristics. Subspecialties were divided into pediatric subspecialties, non-pediatric subspecialties, surgical specialties, and other specialties.
EVALUATING COST AVOIDANCE
Data for cost avoidance were calculated using established per diem rates for the given year group. Per diem rates and flight costs were obtained from Defense Travel System per diem rates and Scheduled Air Transportation Office (SATO) for Fiscal Year 2020. 10,11 Flight costs included both the patient and the nonmedical attendant (NMA), who usually is the parent or guardian of the patient. Cost savings were estimated as the average cost of the visit multiplied by the estimated number of in-person evaluations avoided. The estimated number of total in-person evaluations avoided was determined by a “yes” response to the first survey question: “Did this consult prevent patient movement (preventing unnecessary transfer to TAMC)?” A 95% confidence interval around the estimated rate of visits avoided was used to calculate upper and lower bounds on the cost estimate. Cost avoidance to non-military medical facilities was not included in the calculation due to multifactorial factors involved in cost from individual institutions from various countries.
Results
DEMOGRAPHICS
From March 2017 until February 2020, there were 2,448 PATH consultations initiated for pediatric patients. Table 1 describes patient demographic data. The median patient age was 7.9 years. Nearly half of the cases were generated in 2019 (n = 1,162, 47%). Okinawa, Japan, generated the largest percentage of consults (n = 1,045, 43%). The majority of consults were initiated by general pediatric providers (n = 1,670, 76%), followed by Family Medicine providers (n = 372, 17%). Physicians initiated the majority of consults (n = 1,881, 77%), followed by nurse practitioners (n = 267, 11%). Of note, utilization of the PATH system by other regions including the Marshall Islands, the continental United States, and European regions accounted for 3% of all cases submitted during the analysis window.
Demographic Data for Pacific Asynchronous Telehealth Cases from March 2017 to February 2020
Other refers to departments with less than 25 consults submitted.
IQR, interquartile range; std, standard deviation.
Note: Demographic data for submitted consults with year of submission, patient age, originating site region, the department of the originating provider, and provider title.
The number of teleconsultations made to specific pediatric specialties via PATH is depicted in Figure 2. Among subspecialties, Pediatric Pulmonology, Pediatric Cardiology, and Pediatric Neurology had the most consults (n = 557, 25%; n = 446, 20%, and n = 236, 10%, respectively). The median response time from specialists to consults was 16 h.

Pediatric teleconsultations by specialists. *Other pediatric specialty includes pediatric psychology, pediatric child abuse, adolescent medicine, and child and adolescent psychiatry. **Other non-pediatric specialties include neurology, sleep medicine, endocrinology, anesthesiology, cardiology, critical care, pathology, physical medicine and rehabilitation, infectious disease, pulmonary, rheumatology, preventive medicine, and concussion clinic. ***Other surgical specialties include urology, plastic/reconstructive, general, oral/maxillofacial, OB/GYN, pediatric ENT, cardiothoracic, and vascular. ****Other includes pharmacy, senior medical officer, vaccine health care, dentistry, neuropsychology, psychology, general medicine, nutrition, optometry, pain management, and podiatry.
SURVEY QUESTION RESPONSES
Among the 2,448 PATH consultations, 1,249 (51%) were designated as closed at the time of this analysis. Of the closed cases, there were 1,025 (82%) cases with completed responses to the survey questions. Originating site providers reported that in-person consultation (patient movement) was prevented in 69% (n = 710/1,025) of cases, and care was recaptured from outside the military medical system in 78% (n = 797/1,025) of cases. An affirmative response to the survey question related to the prevention of patient movement was higher in years 2019 and 2020 compared with 2017 and 2018 (80% vs. 48%, p < 0.001). By location, preventing patient movement and recapturing care were significantly higher for cases originating in Japan than for those originating in Guam or Korea (71% vs. 64%, p = 0.037; and 82% vs. 67%, p < 0.001, respectively).
CALCULATION OF COST AVOIDANCE
According to SATO travel, in Fiscal Year 2020, the estimated range of cost a round-trip flight from the Western Pacific Rim main regions (Japan, Guam, Korea) was $1,243 to $1,633. Pediatric patients are authorized a single NMA. Total flight costs for two individuals, the patient and their NMA, ranged from $2,486 to $3,267. Per diem rates for TAMC in 2020 were $117 per night for lodging and $119 per day for food. The average length of stay for routine ambulatory medical evacuations (medevacs) seen at TAMC was 9 days. Using the above government rates for round-trip flight, lodging, and food per diem for 9 days, we estimated the total cost for ambulatory specialty evaluation to be $4,610 to $5,391. With the 710 affirmative responses to the survey question, “Did this consult recapture patient movement?” we estimated total cost saving of ∼$3.3 million for the time period of this study (ranging from $3.2 to $3.8 million) (Fig. 3). Cost avoidance was only calculated based on responses from survey question 1 due to multinational cost variations from different nonmedical facilities.
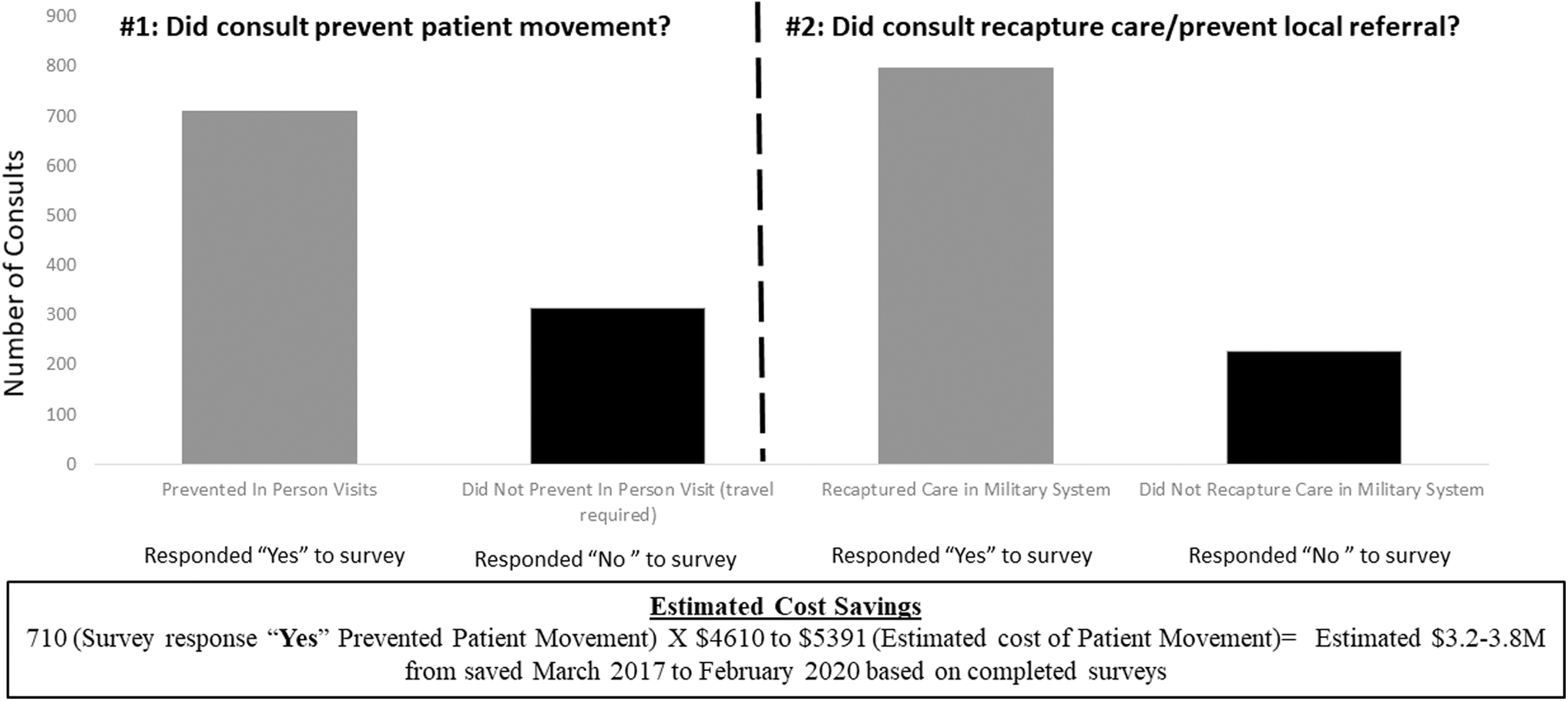
Survey question responses and estimated cost savings from utilization of PATH system. There were 1,025 completed survey responses at the time of this review for all pediatric teleconsultations (41.9% response). Of the 1,025 completed response, 710 (69.4%) were coded as prevented in-person consultation (patient movement) and 797 (77.9%) were coded as recaptured care (care not sent outside military medical system). Taking the average flight cost for Guam, Japan, and Korea given the change in flight cost based on time of year, gas, and other regions, the average flight cost for a round trip in 2020 was $1,243–1,633; per single ticket which would be $2,486–3,267 for pediatric patient and nonmedical attendant (likely parent). The estimated cost savings from avoid patient movement based on these assumptions was $3.2–3.8 million. This is an extrapolation based on the averages used and the coding results and likely underrepresentation of true cost savings. Cost avoidance was only calculated based on responses from survey question 1 due to multinational cost variations from different nonmedical facilities.
Discussion
In this updated analysis of the PATH system, we demonstrated robust utilization that resulted in savings of ∼$3.3 million dollars for the DOD. The estimated impact was that over half of initiated teleconsultations prevented unnecessary patient movement to Hawaii or utilization of care outside the military health system. In comparison to the previously published analysis, we observed growth in utilization from over 1,000 pediatric cases during a 3-year period to over 2,448 observed in our 3-year analysis. 2
In the decade since the impact of the PATH program was assessed on pediatric asynchronous teleconsultations, the overall platform has grown to reach every overseas region where the DOD has medical assets and clinical providers. We attribute that the growth in utilization is the result of both increased volume of originating site providers and the expansion of distant site consultants with experts in more than 60 different specialties. As PATH has expanded, it also opened up opportunities for multidisciplinary provider-to-provider asynchronous telecommunication that includes physician subspecialists, as well as pediatric behavioral health, social work services, and originating site case managers. PATHs feature of secure telecommunications has increased its use for cases of inpatient pediatric transfers, and coordination for scheduled surgical cases that would be occurring at TAMC, which were previously arranged via traditional methods such as telephone and e-mail. The PATH program also has seen growth in pediatric specialty procedures, including asynchronous pediatric PFT interpretation by Pediatric Pulmonology at TAMC, echocardiograms, and radiographs. PATH integrated the administration staff responsible for the PACS for viewing such images, which allowed for TAMC Pediatric Cardiology to view and interpret pediatric echocardiograms asynchronously. The program tracked receipt of images at the distant site and secure communication between the originating site and TAMC Pediatric Cardiologists. The increase in the use of store-and-forward tele-interpretation for PFTs and echocardiograms explains some of the reasons why Pediatric Pulmonology and Pediatric Cardiology were found to have the highest volume of PATH cases during the study window.
The two survey questions provided a source of end user feedback and data to quantify PATHs impact on patient transfers, recaptured care, and estimated cost avoidance as seen in previous studies within the military where asynchronous platforms led to a decrease in unnecessary patient transfers while preserving access to quality subspecialty care. 2,12 Notably, of the 2,448 PATH cases included in this analysis, only 40% (n = 1,025) had survey responses, thus the estimated savings of $3.3 million is likely a significant underestimation of the cost savings. At the time of this analysis, approximately half of the cases were not finalized, accounting for the vast majority of cases without survey responses. Of the finalized cases, ∼18% were closed without completion of the survey. Program managers may consider making the two survey questions mandatory before case closure to improve future data acquisition.
During the window of time for this retrospective review and analysis, the operational costs of the PATH program were supported by TAMC. The daily IT costs for staffing (one system administrator and one programmer), hardware and software maintenance was ∼$250,000/year. The medical director and consult manager functions were all performed by military active duty physicians stationed at TAMC as additional voluntary duties; therefore, no additional costs were necessary for consult management personnel during the review time period.
While the authors analyzed the specific costs of airfare and lodging avoided by decreasing travel to Hawaii, there are additional tangible and intangible costs avoided by retaining the patient and parent at their home duty station. Asynchronous teleconsultations decrease time away from school for pediatric patients, missed work by the parent serving as the NMA, and decrease the need for additional childcare if there are siblings in the home. Whether the active duty parent serves as the NMA or remains home while their child is being evaluated across the Pacific, this time and distance infers additional stress that may affect morale and mission effectiveness.
We acknowledge both strengths and limitations of this analysis. We present an update to the current literature regarding the utilization of the PATH system by military providers and cost savings to the DOD. Our cost saving estimates were informed by individual clinician or administrative staff survey responses without an ability to objectively measure prevention of patient movement or outside care. Although the majority of clinicians and administrative staff would be capable of providing such information, the use of an algorithm or checklist would remove any individual perceptions or biases that could impact the response to the survey questions. We observed improved survey question response in the final year of data collected, suggesting increased familiarity and utilization of this data collection function.
The impact of telemedicine and limiting travel on cost avoidance in the setting of a pandemic was not accounted by this model. The financial and health impact of an existing asynchronous teleconsultation platform during a time with travel restrictions and potential self-quarantine after travel is likely even more significant than what was measured in this review. An area for future study could include looking at the impact of PATH based on survey results from the originating site providers during 2020 to 2021, knowing that there has been increased efforts by PATH consult managers to increase compliance with responses to the closing survey questions. These data from the study window closed before international and national travel restrictions due to SARS-CoV-2 global pandemic in March 2020; however, another future study could assess if there was an increase in teleconsultation volume initiated during that time period.
Conclusions
The use of PATH for pediatric patients more than doubled since the initial evaluation of 1,000 pediatric teleconsultations and continue to provide cost savings while expanding access to subspecialty services in areas within the Pacific Rim. 2,5 This asynchronous telemedicine model is an efficient delivery system allowing for unscheduled consultation and rapid response. Consideration for facilities looking to implement similar systems includes an accountability of time for telemedicine, criterion for assessing encounters and a standardized coding system for reimbursement. 13 The model used for receiving, reviewing, and distributing PATH consults is very similar to the operational review of asynchronous consultations used by non-military organizations such as the Swinfen Charitable Trust, which provides store-and-forward teleconsultation with volunteer medical specialists around the globe to support originating site clinicians in remote and/or austere locations with limited access to subspecialty medical care. 14 This similar model utilizes system operators who provide a function similar to the PATH consult managers by reviewing new cases, e-mail notification to specialists informing them of a new consult, and the system operators providing oversight of responses within the platform. One key difference of PATH is that the U.S. military uses the same electronic medical records system across the globe, allowing the distant site provider to review additional medical history by chart review if needed. The use of patient identifiers within each PATH case does require additional security of the system but creates a more fluid integration between the store-and-forward consult in PATH, access to PACS records, and being able to code for the interprofessional consultation.
Future directions for research may include the evaluation of the trends in host nation referrals as a correlation with PATH consultation numbers, cost savings from avoiding transfers to nonmilitary medical facilities, and the utilization of PATH teleconsultations during the COVID-19 pandemic.
Footnotes
Acknowledgment
The authors acknowledge Mr. Yu-Wei Chang for his role in data collection.
Authors' Contributions
M.M. and J.M. conceptualized and designed the study, and drafted the initial article. K.D., C.N., and M.J. reviewed and revised the article. M.L. designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the article.
Disclaimer
The views expressed in this abstract/article are those of the author(s) and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
Disclosure Statement
The authors have no financial relationships relevant to this article to disclose, no competing interest, no personal financial interests, no funding, no other competing interests, and no recent employment that may gain or lose financially from publication of the article.
Funding Information
No funding was received for this article.