
Abstract
Background:
The clinical effectiveness of audio-only telemedicine has not been fully quantified. The pandemic afforded a unique situation to retrospectively observe clinical outcomes of care for three disease cohorts within three care models, including audio-only telemedicine.
Methods:
Patients were classified into three care models: audio-only telemedicine, in-person, and hybrid. Each model was compared with an aggregate group before the onset of the pandemic and within each group during the pandemic. Each disease cohort was evaluated in cross-sectional and paired analyses.
Results:
Patients (n = 52,720) were grouped within one of three care models. A majority (n = 48,335) of patients qualified for the “pre” group comparison. The audio-only telemedicine care model showed similar control of renal disease, hypertension control, and diabetes management than in-person and hybrid care models.
Conclusions:
Audio-only telemedicine appears to be noninferior to in-person or hybrid models for chronic disease management for the diseases studied. In all instances, it had similar control compared with the in-person care model. We acknowledge the limitations of this study, including convenience sampling and a limited observation timeframe. Audio-only telemedicine should be considered a viable care model modality that can be integrated into options for patient care. Further study and investment are warranted, as it provides efficacy and convenience to health systems (Clinical Registration Number # 32449).
Background and Significance
Telemedicine has experienced substantial growth in the United States and globally for the past few years, with exponential adoption noted with the coronavirus disease 2019 (COVID-19) pandemic. 1 Although there has been promotion and advocacy of telemedicine by the government, reimbursement by the Center for Medicare and Medicaid Services (CMS) has been limited to only telemedicine (which includes video), with a special waiver for audio-only visits only during the pandemic. 2 Uptake of audio–video telemedicine has been limited in some health systems due to budgetary issues as well as problems surrounding the “digital divide,” particularly impacting safety net systems. 3
In Dallas, >40% of households are without fixed internet, 4 leading the top 10 cities in the United States with the most considerable digital divide. 5 In addition to internet limitations, many of these same individuals lack cellular capabilities or having limited or metered data plans.
Parkland Health and Hospital System (Parkland) is a safety net health system that provides care for the citizens of Dallas County, a significant number of whom are socioeconomically disadvantaged. The payor mix includes 28% charity, 11% self-pay, and 31% Medicaid. 6 Parkland had not yet started deploying video telemedicine capabilities across the health system when the pandemic began. Thus, we performed audio-only telemedicine for our patients, where applicable.
Parkland observed three “phenotypes” of patient care models: audio-only telemedicine (AOT), in-person care (INP), and a hybrid of both (HYB). The COVID-19 pandemic created a special incentive for patients to avoid in-person visits with their providers. Starting on March 15, 2020, the overwhelming majority of provider encounters transitioned from INP to AOT due to the organization experiencing its first cases of COVID-19. Parkland found itself in a unique situation to review and assess whether the care provided by audio-only telemedicine presented a viable alternative in chronic disease management compared with care provided in-person or through hybrid modalities.
The Institutional Review Board for the University of Texas at Southwestern approved exemption for this study on January 13, 2021, and Parkland Health and Hospital Systems Office of Research Administration provided approval to conduct research-related activities at the site on January 15, 2021. All patients, metrics, and care models were identified through Parkland's Electronic Health Record (EHR).
Methods
We categorized three populations of patients through convenience sampling who utilized one of the three care models: AOT, INP, or HYB. The patients were then separated into disease cohorts of diabetes (DM), hypertension (HTN), and chronic kidney disease (CKD) based on ICD-10 groupers. We retrospectively observed surrogate metrics reflective of chronic disease management (e.g., hemoglobin A1c [HbA1c] for diabetics) for these disease cohorts from 6 months before (Pre) and 3–6 months after (Post) the March 15, 2021 inflection date.
The care models were assessed using four comparison methods. The Pre-metrics were compared between the care models to establish the baseline differences. The Post-metrics were similarly examined for patient outcomes. The difference between the Pre- and Post-metrics within each care model was assessed in two ways. Once between the Post-metrics and the aggregate of all Pre-metrics within a disease cohort. Then a paired analysis was performed to control for the laboratory baseline values for each patient within disease cohorts. We identified matched patients who had the outcome in question (test or blood pressure measurement) performed before the pandemic and again during the later half of the 6-month observation period (on or after June 15, 2020). Individuals who did not have a pairing were excluded from the paired analysis.
Demographic information was collected across three care models to evaluate the comparability of the groups and potential confounding variables (Table 1). Each disease cohort's laboratories were compared between the three care models during the COVID-19 period to signify cohort differences.
Three Disease Group Demographic Table (
Statistical testing of continuous data was performed using t tests. Statistical testing of categorical data was performed with chi-square tests. Paired statistical tests were performed using paired t tests. All statistical tests used p-values of <0.05 as the definition of statistical significance. “Family-wise” Bonferroni corrected p-values are reported throughout for pairwise tests within chronic disease categories. SPSS and Oracle SQL Database statistical functions were used to organize data and perform statistical tests.
CKD, chronic kidney disease; HTN, hypertension.
Surrogate markers of disease control included HbA1c and microalbumin for people with diabetes, systolic blood pressure (SBP) for those with HTN, and estimated glomerular filtration rate (eGFR) for patients with CKD.
Results
A significant number of patients (n = 158,337) had completed a visit with a Parkland provider during the “pre-” period and 148,924 patients during the post-period. Of those in the post-period, 48,366 patients had AOT only visits, 52,312 had INP only visits, and 48,246 had both (hybrid) (Table 1). Subgroup analyses of chronic disease management surrogates occurred within each, respectively (Fig. 1).
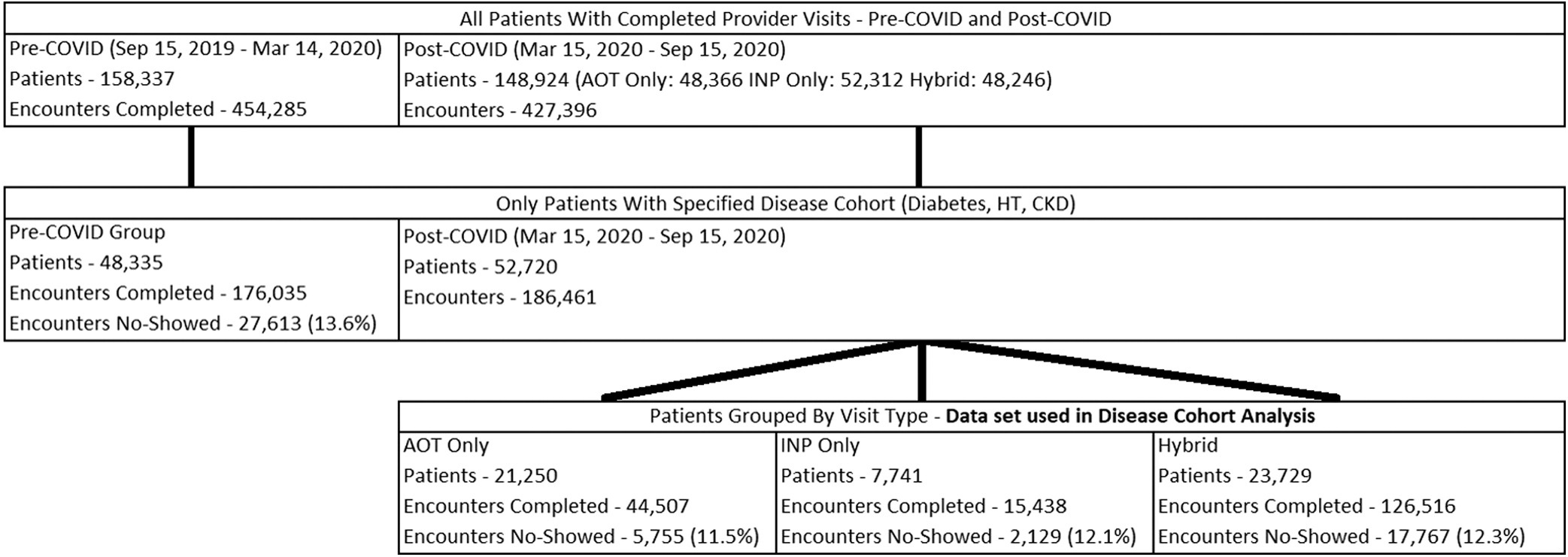
Diagram mapping of patient groupings by care model.
Demographic analysis of the groups showed greater female patients overall. The AOT group had fewer non-Hispanic white patients and the lowest percentage of those who identified English as their primary language. It also had an older demographic compared with INP and hybrid. INP had more commercial payors, whereas all had similar percentages of charity/self-pay. There was a higher percentage of Medicaid/Medicare payor mix in the hybrid group than in INP or AOT.
BASELINE COMPARISON
The baseline eGFR for the AOT group was significantly higher compared with both INP and HYB (Table 2). In contrast, the hybrid group diabetic and hypertensive patients had higher microalbumin and SBP readings, respectively. All groups showed no statistical difference for HbA1C values (Supplementary Appendix Table SA1).
Baseline Comparison
AOT, audio-only telemedicine; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HYB, hybrid of both; INP, in-person care.
PRE- TO POST- COMPARISON
Every surrogate marker that exhibited significant changes worsened between Pre- and Post- measurements (Table 3). HbA1C results for all groups increased by a significant degree when compared with aggregate Pre- levels. SBP was higher in AOT and INP groups than aggregate Pre- values and higher in the HYB group when paired. Every paired group's eGFR declined over time, as well as the INP and HYB groups aggregate eGFR. There were no significant changes in microalbumin results between any care model or comparison method (Supplementary Appendix Table SA2).
Pre- Vs. Post- Group Comparison
OUTCOME COMPARISON
After time had passed, patients in the AOT group still had significantly better mean eGFR than either INP or HYB, but slightly worse SBP control than the HYB group (Table 4). Although the microalbumin results showed no significant differences between patients in any of the care models in aggregate or paired analysis, the AOT care model was no longer statistically different from the HYB group. All other surrogate markers were not significantly different between groups.
Outcome Comparison
Discussion
This study retrospectively compared the clinical effectiveness for three of the four standard care models used in population health (widescale audio–video telemedicine visits were unavailable at our institution at the time of the study). Although all disease cohorts experienced some decline in chronic disease control during the pandemic, the data demonstrate that AOT has similar control and by proxy, health outcomes, to in-person and hybrid care groups in the time these groups.
The pandemic presented a unique opportunity to study the care models separately to assess for differences in surrogate markers of disease management. We captured what we consider to be discrete outcomes of care for the selected chronic diseases. The intent was to allow a minimum of 3 months' intervention in a specific care plan before observing outcomes. Our primary focus was to assess the efficacy of audio-only telemedicine, as it has not been readily studied. Current reimbursement models disfavor this model, which is often necessary when utilizing virtual care modality in a safety net health system for patients who may not use audio–video solutions. 7 Furthermore, many payors are not reimbursing for AOT, and CMS has indicated it may not continue to reimburse these methods after the pandemic ends. 8,9
We found no significant difference in diabetic glycemic management or microalbumin progression with AOT versus the other care models in cohort or paired analysis. The AOT group had the smallest decline in renal function over the time studied, including paired analysis. HTN analysis indicated AOT had a worse baseline and outcome compared with the hybrid model. The hybrid model showed a significant deterioration of control in paired analysis, whereas AOT did not.
The authors recognize the limitations of virtual care for particular patient care needs (e.g., vaccinations, pap smears, and foot examinations) 10 and, as such, chose not to study and highlight that aspect of care. In that same vein, one can say that audio-only telemedicine has the same limitations as audio–video telemedicine. The authors concede that virtual visits have boundaries as to appropriate use cases. We intended to compare those attributes in which audio–video virtual care may be used and whether audio-only virtual care may also be efficacious. As the study showed no significant differences in disease management between the three groups, we submit that audio-only telemedicine visits should be considered a viable care model for the ambulatory care of patients.
There are several areas of possible critique to this study. First, it was retrospective, and the patient care model designations may have carried selection bias, offering virtual care to the healthier or better-controlled individuals. To address that, we used the paired analysis to match specific patients with their “pre-” selves when assessing for differences in the three models to allow for comparisons of the individual matched patients. Second, although we preferred to observe the three groups longer, our “pre-study” analysis showed a significant increase in the crossover from one model to the other by September as the pandemic improved and many practices attempted to return to “normal” in-person operations.
At that point, volumes of in-person visits increased, and there was an extensive crossover between the care models, thus decreasing the size of the groups. We feel that of observation range of 3–6 months was sufficient time for allowing differences in disease management between models to occur, particularly in the pandemic when changes in the patients' level of activity may have markedly impacted control of chronic diseases, depression, adherence with medications and diet, and overall general medical well-being, 11 –13 and given the observation of statistically significant worsening of many disease groups from the “Pre-” group.
Summary and Conclusions
Audio-only telemedicine is an important tool in the care of patients with chronic diseases. Prior studies have shown significant satisfaction by the patients with this modality of care 13 –17 and equity in specific outcomes, 18 and in our institution overall, there was more than a 7% greater “show” rate for the virtual care patients. From our study, it appears to offer similar abilities to manage chronic diseases to that of INP or hybrid care models for the diseases studied, and it affords more convenience for patients and offers efficiencies in clinical practice.
Our retrospective study found that overall care of common chronic conditions can be as effectively managed as with patients seen in person. There appeared to be no substantive difference in the quality of care for patients with those diseases we consider prime examples of good use cases for virtual care with audio-only telemedicine. Given significant limitations to patients being able to adopt audio–video solutions, particularly in inner-city safety net populations where socioeconomic limitations are more commonly encountered, audio-only telemedicine may be a useful alternative. Further investigation is warranted into reimbursement models for this care modality, which can provide a simplified continuity of care for these common chronic diseases as well as other potential health engagement interactions with patients.
Practitioners may wish to consider utilizing audio-only telemedicine as an additional solution for chronic disease management of their patients, particularly those who have difficulty keeping in-person appointments (e.g., socioeconomic struggles, travel insufficiency, and childcare obligations). The authors hope this study stimulates further investigation into audio-only telemedicine's value, efficacy, and utilization, particularly for populations at risk, disparity-impacted, and living in digital deserts.
Footnotes
Authors' Contributions
The authors all have contributed to the creation of methodology, data collection and interpretation, article creation, and review of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this study was provided internally by Parkland Health and Hospital System.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.