
Abstract
Introduction:
Telemedicine has become increasingly important over the past decade. With the pressure of the COVID-19 pandemic, demands for remote health care solutions have seen an unprecedented rise. However, many questions regarding the feasibility and benefits of telemedicine remain. The aim of our study was to evaluate both the technical feasibility and patient satisfaction with video consultations in a tertiary center for obstetric care.
Materials and Methods:
This prospective single-center trial was part of the larger open Video Service project on telemedicine at the Department of Gynecology and Obstetrics at the University of Münster. Patients requiring prenatal or prepregnancy counseling were included. A questionnaire was designed for the evaluation of patient satisfaction and filled in by both patient and health care provider at the end of the video consultation.
Results:
Of 80 eligible cases, 75 video consultations were carried out and data from the questionnaire were collected. Overall patient satisfaction was high (95%, 71/75) although technical problems occurred in 37% (29/75) of the appointments. Health care providers' satisfaction was equally high and in 88% (66/75) of cases, remote consultations avoided an in-house visit without effect on health care quality.
Conclusions:
Remote consultations are feasible and yield high satisfaction rates even in a medical field as sensitive as perinatal medicine. Further research is necessary to determine the cost-effectiveness and effects on perinatal outcome. Health care systems should be offered clear guidance on medicolegal issues and funding of remote consultations to integrate telemedicine into routine health care.
Introduction
The COVID-19 pandemic has challenged the medical sector worldwide in many different ways. Besides the obvious burden that the increasing number of severely ill patients has put on hospitals and primary caregivers, health care professionals also struggle to maintain routine health care amid government restrictions on patient mobility. While routine appointments were largely put on hold at the beginning of the pandemic, it now becomes increasingly important to develop alternative ways to deliver medical care.
Telemedicine was originally defined in the 1960s as a technology providing regular medical services “without the usual patient-physician confrontation.” 1 With the widespread availability of new technologies, the use of telemedicine has become increasingly attractive. As early as 2014, 11% of intensive care patients in the United States (U.S.) were treated using telemedicine. 2 Initially seen as a means to bring specialist care to rural settings with limited access to medical services and to reduce health care costs, 3 the COVID-19 pandemic has given the demand for telemedicine an unprecedented momentum. 4
Telemedicine includes various electronic applications for the exchange of medical data and images, as well as programs for remote video consultation between the patient and health care provider. Due to advances in mobile telecommunication technology, telemedicine is also used for e-health or m-health. 5
As telemedicine is propelled from the sidelines into the mainstream of medical care, legal and ethical issues arise. 3 Unlimited access to mobile data transfer is confronted with the need for strict data security and confidentiality. This is especially true for Germany, where digitization is slow and people tend to be more reluctant to embrace new technologies for the sake of data protection. 6 The lack of personal interaction between the patient and health care provider has raised concerns about the quality of the doctor/patient relationship in telemedicine. 7,8
Despite these controversies and the impossibility of remotely conducting a physical examination of the patient, many medical specialties have taken first steps toward the use of telemedicine. Studies using telemedicine in fields such as neonatology, diabetes surveillance, and remote assessment of patients with chronic heart failure have shown potential benefits and cost-effectiveness of remote interventions. 9 –12 However, results are sparse when it comes to patient satisfaction.
In all areas of modern medicine, consideration of patient satisfaction is the key factor for treatment adherence and economic success of health care institutions. 13 To our knowledge, there are little data so far demonstrating patient satisfaction with remote medical counseling in an area as sensitive as prenatal medicine. The aim of this study was, therefore, to evaluate both the technical feasibility and patient satisfaction with video consultations in a tertiary center for obstetric care.
Methods
This prospective single-center trial was conducted at the Department of Obstetrics and Gynaecology of the University of Münster between April 2020 and April 2021. The study was part of the larger open Video Service (oVID) project based at the University Hospital Münster and aims at evaluating telemedicine solutions in various medical fields such as trauma surgery, palliative care, and obstetrics.
Ethical Approval
The study was designed according to the Declaration of Helsinki and approved by the Ethics Committee of the local medical council and the University of Münster (trial no. 2019-683-f-S). The oVID project is funded by the European Regional Development Fund (no. EFRE-0801384).
Women older than 18 years seeking appointments for prenatal or prepregnancy counseling were included in this study if they agreed to have remote video consultation instead of an in-house visit. Verbal consent was obtained from all participants before enrollment.
For remote counseling, La Well-CGM's ELVI software (CompuMedicalGroup, Koblenz, Germany) was used. Women accessed the platform through an invitation link issued by the provider. All video consultations were carried out by senior clinicians and specialists in perinatal medicine.
A questionnaire was designed for the evaluation of patient satisfaction. The providers completed their and the participants' answers at the end of the online session. The complete set of questions is shown in Tables 1 and 2.
Questionnaire Patient
Questionnaire Health Care Professional
Statistical Analyses
As the majority of the questions are in a single/multiple choice format, the results take the form of categorical variables. These were analyzed descriptively in terms of absolute and relative frequencies. Continuous variables are presented as mean ± standard deviation. For the descriptive evaluation, we used Python 3.8. IBM SPSS® Statistics 27 for Windows (IBM Corporation, Somers, NY) was used for data analysis.
To quantify evidence of differences between the distance from the University Hospital Münster and the fact whether a patient had been treated at the University Hospital Münster or the Department of Obstetrics before, the Mann–Whitney U-test was used. Multiple group comparisons were performed using the Kruskal–Wallis test. All inferential statistics are intended to be exploratory (hypotheses generating), not confirmatory, and are interpreted accordingly. p-values are considered noticeable in case p ≤ 0.05.
The topics covered during these video consultations included a wide range of issues such as prepregnancy counseling due to preexisting maternal conditions or maternal medication, history of recurrent pregnancy loss or complications during a previous pregnancy, advice on maternal medication or treatment during pregnancy, as well as lactation counseling.
Results
Eighty (n = 80) women were offered a video consultation. However, in five cases, the planned video consultation could not take place. In three of these, the patient did not connect to the program and was unavailable by phone. One woman declined to have a video consultation and preferred to speak to the provider on the phone. In one case, the video consultation had to be rescheduled due to technical problems.
Altogether, 75 video consultations were carried out and data from the questionnaire were collected. In six cases of these, women requested an additional video consultation for follow-up. The general characteristics of the study population are displayed in Table 3. The mean maternal age was 32 years. Mean distance from the University Hospital Münster was 46 km, with a minimum of 2 km and a maximum distance of 166 km. A total of 62.7% (47/75) of the included patients were regular patients at the University Hospital Münster, but only 28.0% (21/75) had been previously treated at the Department of Obstetrics.
General Characteristics of the Study Population
A total of 13.3% of video consultations covered recurrent pregnancy loss, 48.0% covered preexisting maternal diseases or medication, 20.0% were about prepregnancy counseling after a pregnancy with complications, in 13.3% consultations centered around complications or treatments options during a current pregnancy, and in 5.3% of cases, video consultation was used for lactation counseling. Seventy-two women with a video consultation agreed to respond to the questionnaire. For 95% (71/75) of patients, the video consultation provided useful answers to their questions and gave them security on the following treatment steps.
Without the option of video consultation, the majority of women would have scheduled a regular appointment at the University Hospital Münster (88%; 66/75), while only 5% (4/75) would have abstained from seeking medical advice. Eighty-eight percent (66/75) of participants had never used a video consultation with a health care professional before, but 96% (72/75) of participants would do so again after their experience.
A majority, 76% (57/75), of consultations were held with the patient alone, while in 23% (17/75) of cases, a family member was also present. Fifty-one percent (38/75) of participants chose to leave individual comments to the questionnaire. Many pointed out that video consultations made the appointment easier for them, as transport to the clinic, waiting time in the hospital, and additional requirements, such as child care during the appointment, were avoided.
All health care professionals agreed to respond to the questionnaire. Health care professionals' satisfaction with remote appointments was equally high. In 88% (66/75) of cases, they found that video consultation avoided an in-house visit. Ninety-six percent (72/75) of remote consultations were considered useful and in 93% (70/75) of cases, all necessary aspects for clinical decision-making could be addressed through video consultation.
More than one-third (37%, 29/75) of the video consultations encountered technical problems of some kind. A list of the most frequent technical issues is displayed in Figure 1. Altogether, unsatisfactory quality of image or sound, as well as insufficient internet quality, was the most frequent problem.
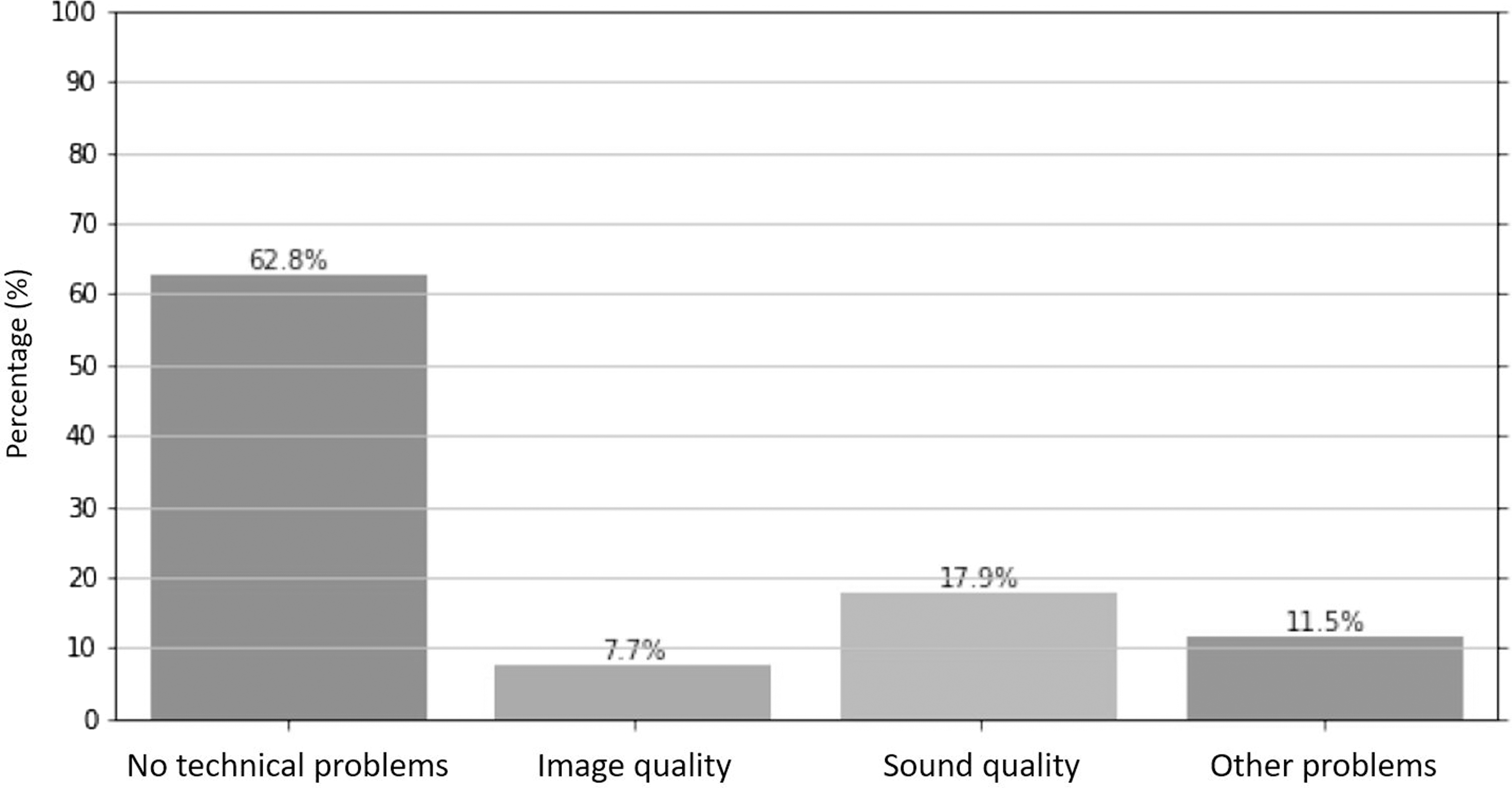
Technical problems experienced during video consultations.
There was no correlation between women's distance from the University Hospital Münster and previous treatment at the University Hospital Münster or the Department of Obstetrics (p = 0.384 and p = 0.986, respectively). Also, the distance from the University Hospital Münster did not correlate with the topic of the video consultation (p = 0.490). There was no correlation between maternal age and previous treatment at the Department of Obstetrics (p = 0.413) or the topic of consultation (p = 0.091).
Discussion
Our study showed that video consultation was feasible and broadly accepted even in a sensitive medical area such as prenatal care and prepregnancy counseling. Overall, patient satisfaction was high despite the technical problems experienced in a significant number of video consultations. Provider satisfaction was equally high and in many cases, in-house visits could be avoided without impacting the quality of medical care. To our knowledge, ours is one of the few studies examining patients' and providers' satisfaction with virtual medical care in an obstetric setting.
Our results are in line with previous studies on the use of remote care in obstetrics. In 2017, Pflugeisen and Mou published a study comparing patient satisfaction with the use of telemedicine as a supplement to standard care in a low-risk obstetric cohort with traditional in-house care. 14 The virtual obstetric care model has been described by the same group in 2016 15 and has been shown to be safe in low-risk obstetric patients. On inclusion in the 2017 study, patients could choose to have part of their prenatal visits as video consultation and patient's opinions were assessed using a four-domain satisfaction questionnaire.
General satisfaction was high in both groups, with significantly higher satisfaction scores in the virtual care group. Scheduling assessment differed most strongly between the treatment groups, indicating easier appointment planning and scheduling when assigned to telemedicine. A total of 96 (12.1%) traditional-care and 75 (19.8%) virtual-care patients responded, yielding a significantly higher response rate among virtual-care patients. However, as response rates to the satisfaction survey were low, the results may be subject to substantial bias.
In their review on telemedicine in perinatal care, van den Heuwel et al. analyzed the results of more than 70 studies on the subject. 9 While results were inconsistent on the economic evaluation of telemedicine, studies showed a benefit of telemedicine in diabetes surveillance, smoking cessation, improvement of lifestyle, gestational weight gain, and mental health. Patient satisfaction was reported to be high, but no systematic study was available to support this assertion.
In the largest study on patient satisfaction to date, Butler et al. randomized 150 patients in the first trimester into a telemedicine group and compared women's stress levels during pregnancy with patients receiving standard care. 16 While results on pregnancy outcome and treatment adherence were similar in both groups, perceived stress levels turned out to be lower in the group with remote appointments in addition to in-house visits.
Provider satisfaction is a relevant factor contributing to the success of remote health care. Health care professionals not only tend to have more reservations regarding the use of telemedicine compared with their patients, but are also more aware of potential risks. 17 This may be due to several factors such as age, medical background, or education level. However, Willcox et al. included a broad variety of applications in their study ranging from public and even commercial websites and apps to social networks and programs for video consultations, some of which may raise medicolegal risks, such as privacy issues and incorrect medical advice. These results must, therefore, be interpreted with caution.
Under the pressure of the major COVID-19 outbreak in New York City, Madden et al. evaluated the feasibility of telemedicine for pregnancy-related consultations and provider satisfaction with telehealth. 18 During the study period, over 4,000 visits were carried out, 30% of which were performed using telemedicine. By the end of the study period, telemedicine was used for 61% of visits in maternal/fetal medicine, and genetic counseling was provided almost exclusively as teleconsultation. Thirty-six practitioners responded to the survey, and the overall satisfaction with telemedicine as an additional option to regular care was overwhelming. However, the authors also concluded that additional office staff, as well as IT support, are needed for implementing and maintaining the telemedicine in clinics.
The benefits of telemedicine have also been shown in other medical fields. In their Cochrane analysis, Flodgren et al. found no difference in mortality among patients with chronic heart failure with and without remote appointments as addition to standard care. 12 In this study, they saw an improvement in metabolic control and mental health in patients receiving remote care. Unfortunately, data on hospital admissions were inconsistent.
In their review, Makkar et al. reported promising data on the use of telemedicine for the follow-up of preterm children in various settings after hospital discharge. 19 Parents' satisfaction with the use of remote appointments for the follow-up of their preterm infants was high, as they felt strengthened in their role as primary caregivers. 20 Several studies on the use of telemedicine in pediatric settings found a reduced transfer rate among hospitals and reduced length of hospitalization. 10,21
Acceptance of and satisfaction with remote counseling through video consultation varies broadly among patient groups and providers. Many factors influence the patients' perceptions of these new technologies such as age, medical conditions and their severity, level of education, and general accessibility of health care close to the patients' home. Therefore, conclusions regarding effectiveness and patient involvement are difficult to draw and further studies targeting specific medical areas and patient groups are required. 22
Like in other medical fields, prenatal and postpartum care has been strongly affected by the COVID-19 pandemic. In their large cross-sectional study, Ceulemans et al. evaluated the impact of the COVID-19 outbreak on perinatal care in Belgium. 22 A total of 2,647 pregnant women and 3,823 breastfeeding women were included in the study and completed the online surveys about the primary care they received. More than half of the patients reported a reduced amount of medical counseling and fewer appointments due to restrictions. First-time mothers during the puerperium turned out to be the most vulnerable group.
While it is impossible to replace all health care visits with remote consultations, telemedicine can be helpful when managing routine health care during a pandemic. As our study has highlighted that patients of childbearing age may be especially amenable to telemedicine, probably due to the fact that young women are accustomed to the use of the internet and mobile devices in their daily lives.
One limitation of our study is the pandemic setting in which the study was carried out. In this exceptional context, remote health care appointments were covered by health care insurance, which had previously not been the case. Due to government restrictions on mobility, patients may have been prompted to accept a video consultation even though they would have preferred an in-house visit, had there been an opportunity. Likewise, they may have been more likely to overlook some technical problems, given the overall strain on internet capacity in Germany during the pandemic. Under normal circumstances, these technical issues may have reduced patient satisfaction. However, given the number of patients willing to receive a video consultation, our study's results can be considered reliable in this specific setting.
So far, much attention has been devoted to the efficacy and cost-effectiveness of telemedicine. Patient satisfaction and the acceptance of a doctor/patient relationship through telemedicine have been neglected in previous research. 23 As one can expect that telemedicine will remain an important addition to medical care even after the end of the COVID-19 pandemic, further research should be dedicated to questions such as treatment adherence, long-term follow-up via telemedicine, and the effects on obstetric outcome.
Conclusions
Patient and provider satisfaction with the use of telemedicine for remote counseling in perinatal care was very high, despite frequent technical problems such as insufficient internet quality. As telemedicine is likely to remain an important addition to regular care in areas such as perinatal medicine, prospective studies are needed to quantify cost-effectiveness and effects on obstetric outcome. Health care providers need adequate equipment and personnel, sufficient internet coverage, and a clear regulatory background to integrate telemedicine into everyday practice.
Footnotes
Acknowledgments
The authors would like to thank everyone who voluntarily dedicated their time and effort.
Authors' Contributions
K.O.—study design, data acquisition and analysis, and article writing and editing. R.S.—data analysis and article editing. M.M.—data acquisition and article editing. J.B.—data acquisition and article editing. D.D.—data acquisition and article editing. M.S.—data acquisition and article editing. H.A.K.—data acquisition and article editing. G.A.—data management and statistical analyses, and article editing. M.E.—data management and statistical analyses, and article editing. K.F.—data management and statistical analyses, and article editing. M.S.—data management and article editing. F.E.—study design and article editing. J.W.—study design and article editing. C.J.—study design and article editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
Licenses for the ELVI platform were acquired as part of the oVID project, which is funded by the European Regional Development Fund (no. EFRE-0801384).