
Abstract
Background:
Health information technology (HIT) may influence pneumococcal vaccination uptake in high-risk populations. This study assessed the association of HIT utilization on pneumococcal vaccine (PCV) uptake among adults ≥40 years with heart disease.
Methods:
This was a cross-sectional study of 2,134 individuals representing 16,813,593 United States adults ≥40 years with heart disease using the National Health Interview Survey data. The independent variables were use of the Internet to (1) look up health information, (2) fill a prescription, and (3) schedule a medical appointment, and use of an e-mail (4) communicate with a health care provider. The dependent variable was PCV uptake. Chi-square analysis was used to evaluate group differences, and a multiple logistic regression was used to analyze the association between HIT utilization and PCV uptake.
Results:
Those who use the Internet to fill up a prescription and to communicate with their health care provider were more likely to take up the PCV (adjusted odds ratio [AOR] 1.56; 95% confidence interval [CI] 1.03–2.37, p = 0.035) and (AOR 1.95; 95% CI 1.23–3.10, p = 0.005) respectively. Compared with those who did not use HIT in any form, those who used HIT in at least three or four forms had a higher PCV uptake (AORs 1.93; 95% CI 1.19–3.13, p = 0.008) and (AOR 2.33 95% CI 1.22–4.47, p = 0.011) respectively.
Conclusion:
Our analysis shows a positive association of HIT utilization and PCV uptake. It further stresses the importance of electronic health in preventive medicine. This implies that HIT can be used purposively in other aspects of preventive health. Larger studies should evaluate the relationship between different uses of HIT and the uptake of different vaccines.
Introduction
Individuals with invasive pneumococcal disease (IPD) are at a high risk of morbidity and mortality. 1,2 Those at the highest risks are individuals with comorbidities such as chronic heart disease, chronic pulmonary disease, diabetes mellitus, and acquired immune deficiency syndrome. 2,3 Although this risk can be reduced with the pneumococcal vaccine (PCV), 4,5 the burden of IPD remains significantly high, with 1.6 million deaths reported annually. 6 This is partly due to the reduced uptake of the PCV over the years, despite the reported efficacy. Some reasons for this reduced uptake include varying vaccination schedules, vaccination fatalistic beliefs, mobile populations such as migrants and ethnic minorities, and antivaccination movement groups. 7 –9
Over the years, different measures have been introduced to address some of these reasons. They include the establishment of minimum vaccination requirements, mandatory vaccinations, and addressing disinformation from antivaccination movement groups. 8,10 Despite these, the Center for Disease Control and Prevention (CDC) reported a vaccination rate of 24.5% and 69% among adults 19–64 years and ≥65 years of age in 2017. 11 A novel approach that may help increase the uptake of PCV is the use of health information technology (HIT), a tool that has been shown to increase the uptake of other vaccines. 12,13
The HIT involves the use of cloud-based services in health care. 14 It mainly utilizes electronic health records (EHR) and other patient-related data in improving the effectiveness and efficiency of delivering health care. 14 Since the implementation of the health information technology for economic and clinical health (HITECH) Act, there has been an increase in the uptake of HIT. Between 2009 and 2014, the use of basic EHR rose from 7.6% to 45.6%. 15,16 This increase has presented numerous positive effects, as shown in various studies. The HIT has been shown to improve patient safety in inpatient settings, 17 improve multiple patient outcomes, both physically and mentally, 18,19 and, more recently, help maintain the provision of high-level care to patients during the COVID-19 pandemic. 14 Despite these benefits, the use of HIT as a potential tool for increasing PCV uptake in adults ≥40 years with heart disease is yet to be studied. This study aims at assessing the prevalence of HIT use among adults ≥40 years with heart disease and at evaluating whether an association exists between HIT utilization and the uptake of the PCV among this population.
Methods
STUDY DESIGN
This study utilized a sample of the adult core data from the 2018 National Health Interview Survey (NHIS). This is a cross-sectional survey of non-institutionalized civilian population of the United States conducted by the CDC with a conditional response rate of 83.9%. The data contained variables on sociodemographic factors, HIT, vaccination, and medical conditions with a total population of 25,417 adults. An IRB review was not required, as a publicly anonymized database was used. Further details of this survey data are available elsewhere. 20
STUDY POPULATION
The study population comprised of 2,134 adults ≥40 years with heart disease, as shown in Figure 1. This was derived from respondents who were ≥40 years of age who answered yes to the question, “have you ever been told by a doctor or other health professional that you had any heart condition or heart disease?”
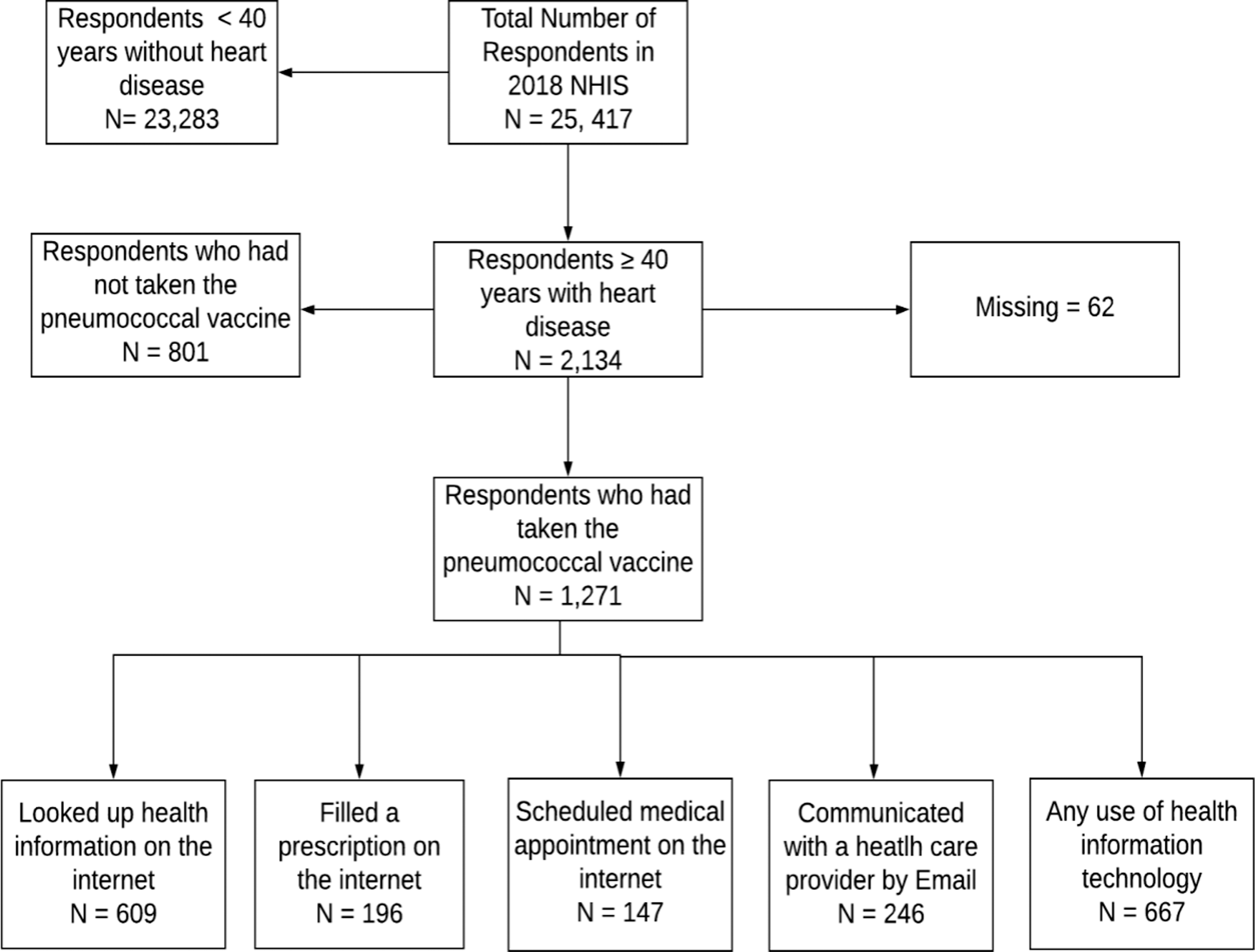
Flow chart of the study population.
MEASURES
Background characteristics
Characteristics of the participants include age, gender, race, marital status, body mass index, hypertension status, diabetes mellitus status, and smoking status.
Independent variable: HIT
In the survey, individuals were asked whether they had used the Internet to: (1) look up health information, (2) fill a prescription, and (3) schedule a medical appointment (appt) whether they had used an e-mail (4) communicate with a care provider. All of these questions have been validated in a previous study. 21 In addition, a composite variable of HIT use was created from the questions cited earlier.
Dependent variable: PCV
Individuals were asked, “Have you ever had a pneumonia shot?” They were considered to have had a shot if they answered “yes.”
STATISTICAL ANALYSES
We applied a sample weight in the analysis to ensure generalizability of the result and to reduce nonresponse bias. The association between sociodemographic variables and HIT use was analyzed by using a Pearson's Chi-square test, with frequencies and weighted percentages reported. A bivariate analysis was used to examine associations between sociodemographic variables for the different uses of HIT. Multiple logistic regression models were used to determine the impact of HIT use on PCV uptake, adjusting for covariates as seen in the Supplementary Tables S1–S4. The results of the regression models were presented as crude odds ratios (ORs) and adjusted odds ratios (AORs) with 95% confidence interval. The analysis was performed by using STATA 14.0 software (Stata Corp., College Station, TX, USA), with the statistical significance set at a p-value of ≤0.05.
Results
The characteristics of the study population are outlined in Table 1. The study population were mostly 65 years and older (54.4%), females (51.1%), White (83.6%), married (57.8%), obese (42.1%), nondiabetics (74.2%), hypertensives (68.7%), and nonsmokers (88.0%). The percentage of adults ≥40 years who used HIT was 55.4%. Among these, most of them were between 40 and 64 years old (55.5%), females (52.8%), White (86.9%), married (63.8%), nondiabetics (77.3%), and hypertensives (64.0%).
Baseline Characteristics of the Study Population
BMI, body mass index; HIT, Health information technology.
Table 2 shows the prevalent uses of HIT among adults ≥40 years of age with heart disease. More than half of them reported looking up health information on the Internet (51.3%). However, less than half reported communicating with a health care provider via e-mails (18.8%), filling prescriptions with the help of the Internet (15.6%), and scheduling appointments with health care providers (14.8%).
Proportion of Different Uses of Health Information Technology Among the Study Population
The crude ORs and adjusted AORs of the relationship between the different uses of HIT and PCV uptake are shown in Table 3. The odds of PCV uptake in adults ≥40 years with heart disease, if they used the Internet to look up health information, was 28% lower than those without Internet use for health information (OR = 0.72; 95% CI = 0.59–0.89, p = 0.002). However, this was not significant after adjusting for covariates. The odds of PCV uptake is 9% higher among those who use the Internet to fill up prescriptions than those who do not, but this was not statistically significant (OR 1.09; 95% CI = 0.81–1.46, p = 0.572). However, after adjusting for covariates, it became statistically significant with a 56% higher uptake in these individuals (OR = 1.56; 95% CI = 1.03–2.37, p = 0.035). The odds of PCV uptake in individuals with heart disease was 31% times higher among those who use the Internet to communicate with health care providers versus non-Internet users for the same purpose (OR 1.31; 95% CI = 1.01–1.72, p = 0.047). In fact, the odds even became higher by 95% after adjusting for other covariates (OR 1.95; 95% CI = 1.23–3.10, p = 0.005). On the other hand, the odds of having taken PCV if they use the Internet to schedule a medical appointment was not statistically significant, even after adjusting for covariates.
Multivariable Logistic Regression Model of Health Information Technology Utilization and Pneumococcal Vaccine Uptake
Adjusted for age, smoking status, hypertension, diabetes mellitus, and marital status.
CI, confidence interval.
Table 4 shows the crude ORs and AORs of uptake of PCV by adults ≥40 years of age with heart disease who use HIT for different purposes cumulatively. The adjusted odds of PCV uptake is 81% higher for adults ≥40 years old with heart disease who utilize at least three forms of HIT than those who do not use HIT at all (OR = 1.81; 95% CI = 1.13–2.91, p = 0.014). There is a further increase of 120% of PCV uptake if they use at least four forms of HIT compared with no HIT use at all (OR = 2.22, 95% CI = 1.17–4.22, p = 0.015).
Multivariable Logistic Regression of the Cumulative Use of Health Information Technology and Pneumococcal Vaccine Uptake
Adjusted for age, race, marital status, and diabetic and hypertensive status.
Discussion
The purpose of this study was to assess the prevalence of HIT use among adults ≥40 years with heart disease and evaluate the relationship between HIT utilization and PCV uptake by using a nationally representative sample. Overall, our findings showed that adults ≥40 years with heart disease have a high rate of HIT utilization, and the odds of receiving a PCV shot increases with the use of multiple forms of HIT. In addition, two of the four categories of HIT (fill up the prescriptions and communicate with health care providers) showed a positive impact in a PCV shot uptake in this population in the multivariate modeling. These findings are consistent with the study by Kindratt et al. that concluded that HIT use contributes more toward influenza preventive services, in particular, vaccine uptake. 22
Further, we considered adult populations with heart disease due to their high mortality and morbidity index from pneumococcal-related illnesses, as HIT use has been associated with improved heart disease outcomes. Several studies have shown that HIT use improved heart failure-related hospitalization, mortality, length of hospital stay, medication adherence, and cardiovascular risk factors in populations with heart diseases. 23,24 For example, Widmer et al. reported that HIT use in cardiac rehabilitation reduces rehospitalization and cardiovascular risk factors such as blood pressure, excessive weight, and physical inactivity. 25 Another study also showed that digital health technologies enhanced medication adherence among individuals suffering from coronary heart diseases. 26 To the best of our knowledge, no other studies have evaluated the effect of HIT utilization in improving PCV uptake in adults ≥40 years with heart disease.
Our study revealed that HIT utilization predominantly involves looking up health information on the Internet (51.3%). In addition, two other forms of HIT utilization, which include filling up prescription medications (OR = 1.56, p = 0.035) and communicating with health care providers by e-mail (OR = 1.95, p = 0.005), were the significant digital forms that increased the odds of PCV shot uptake among adults ≥40 years of age with heart disease. The possible explanation is that these two HIT forms use a direct mode of electronic communication with the health care system, indicating a greater patient engagement for preventives services such as vaccination, and ultimately better health outcomes. 27 This engagement with the health care system may be the predominant factor in the increased uptake of PCVs. Previous studies have shown that greater involvement of patients with health care providers using digital communication (e.g., e-mail) improves medication adherence, weight loss, and clinical outcomes of patients with hypertension and diabetes, two significant risk factors for heart disease. 28 –30 Hence, there is a need to increase the awareness of a potential means of engagement through HIT with the health care system among adults ≥40 years, as this may lead to a greater access to health care interventions such as vaccination. This greater engagement using HIT may significantly impact individuals seeking other preventive services and potentially increase survival outcomes from other comorbidities.
Interestingly, it is important to mention that our study findings showed that utilization of the only two significant forms of HIT would not improve PCV uptake. Rather, we found out that the pneumococcal vaccination rate would not be positively impacted unless there is at least utilization of three forms of HIT (OR = 1.81, p = 0.014). Previous studies have shown that the use of multiple forms of HIT showed a positive effect on medical outcomes. 31 –33 Kruse and Beane demonstrated that 25 out of 37 studies (81%) exhibited multiple HIT forms in the improvement of medical health outcomes. 18 However, most outcomes in the studies were not related to PCV uptake, reflecting the significance of our study.
STRENGTHS AND LIMITATIONS
A few studies have researched the association between HIT use and vaccination uptake. In fact, to the best of our knowledge, our study is the first to demonstrate a positive association between multiple uses of HIT forms and PCV uptake in adults with heart disease. Another strength of our study is that we have two subpopulation groups for our study: first, adult populations who are 40 years and older; second, a population with a confirmed or unconfirmed heart condition.
Due to the cross-sectional nature of our study, causality cannot be inferred. Our results show a positive association between the use of HIT in accessing health care and PCV uptake. Another limitation is that all the measured variables were self-reported, making the responses questionable in certain instances. In addition, the survey instrument was not exhaustive of the different ways that HIT can be used and, as such, the responses of the participants are questionable. Lastly, with the way the composite variable was coded it was difficult to identify which of the uses of HIT play a significant role in increasing the correlation with PCV uptake. Future studies should explore other uses of HIT and evaluate HIT as a preventive tool among other populations.
Conclusion
The study used a national survey that suggests that adults 40–64 years old with heart diseases are more likely to utilize HIT than adults who are 65 years and older, especially to look up health information. Users who use HIT in communicating with their health care providers are more likely to take a PCV shot, and this communication may underlie patient's engagement as a prior factor for increased vaccine uptake. The study concluded that no linear relationship exists between the number of HIT forms utilized and PCV uptake, as we found only two significant correlations out of four. Further, there is a need to conduct more research to explore other uses of HIT or the frequency of HIT forms that would improve pneumococcal vaccination among the adult population with heart disease. Longitudinal studies might also be helpful to assess HIT utilization and PCV uptake.
Footnotes
Authors' Contributions
Conceptualization: O.K., J.A., and O.F. Data analysis: O.K. Editing and text writing: O.K., J.A., S.S., A.A., and O.F.
Data Statement
Data used for this analysis are available at
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.