
Abstract
Introduction:
The COVID-19 pandemic has hastened the adoption of telehealth and the drastic shift to an unfamiliar process may impose significant impact to the quality-of-care delivery. Many providers are interested in understanding the quality of their telehealth services from the patients' experience.
Materials and Methods:
A telehealth patient satisfaction survey (TPSS) was developed by using an iterative stakeholder-centered design approach, incorporating elements from validated telemedicine and customer service survey instruments, and meeting the operational needs and constraints. A cross-sectional study design was employed to collect survey responses from patients and families of a large pediatric hospital. Finally, we performed exploratory factor analysis (EFA) to extract latent constructs and factor loadings of the survey items to further explain relationships.
Results:
A 22-item TPSS closely matched the existing in-person patient satisfaction survey and mapped to a revised SERVPERF conceptual model that was proposed by the interdisciplinary committee. Survey was implemented in the HIPAA-compliant online platform REDCap® with survey link embedded in an automated Epic MyChart (Verona, WI) visit follow-up message. In total, 2,394 survey responses were collected between July 7, 2020, and September 2, 2020. EFA revealed three constructs (with factor loadings >0.30): admission process, perceived quality of services, and telehealth satisfaction.
Conclusions:
We reported the development of TPSS that met the operational needs of compatibility with existing data and possible comparison to in-person survey. The survey is short and yet covers both the clinical experience and telehealth usability, with acceptable survey validity.
Introduction
As the pandemic of COVID-19 swept across the globe, most businesses and services shifted to online platforms to reduce risk of exposure. This also led to a wave of rapid adoption of telehealth services by the health care organizations, a sector that has been slow to adopt new technologies. 1 To rapidly expand the use of telehealth across the United States, the Center for Medicare and Medicaid Services issued an emergency declaration of waivers, which removed provider licensing mandates, patient-provider established relationship requirements, and requirements related to location of telehealth offerings. 2 The Office of Civil Rights waived software privacy requirements, allowing hospital systems to provide telehealth with nonpublic facing video chat softwares, thereby reduced the adoption barriers. 3,4
With the drastic change in health care delivery from in-person to virtual, health care organizations and their providers want to know their patients' telehealth experience and use the feedback to improve telehealth service delivery. There are some existing telehealth surveys, such as the Telemedicine Satisfaction and Usefulness Questionnaire (TSUQ), 5 Telemedicine Satisfaction Survey (TSQ), 6 and Telehealth Usability Questionnaire (TUQ). 7 Unlike the traditional patient satisfaction survey, these instruments revolve around the telemedicine modality with strong emphasis placed on the technology and have limited utility in comparison between telehealth and in-person visits. Moreover, these surveys may not be compatible with previously collected in-person visit satisfaction data.
In this article, we share a survey content design process that consolidated the existing telehealth surveys into core data elements, allowing for backward compatibility with in-person visit satisfaction data collection, and prioritized rapid implementation by balancing the survey validity with operational need. To explain the item relationships to further investigate patient attitude and conceptualize the satisfaction, we performed exploratory factor analysis (EFA) to extract latent factors that might reflect the underlying dimensions of telehealth patient satisfaction.
Approach
SURVEY DEVELOPMENT APPROACH
A working group consisting of key stakeholders from administrative, operation, and clinical departments was formed to inform the development of the survey (n = 21). Survey was developed through the following steps: (1) understand operational needs, constraints, and existing efforts on patient satisfaction surveys across the organization; (2) literature review on theoretical framework on patient satisfaction; (3) survey content development; and (4) review and revision. The general process and timeline are depicted in Figure 1.
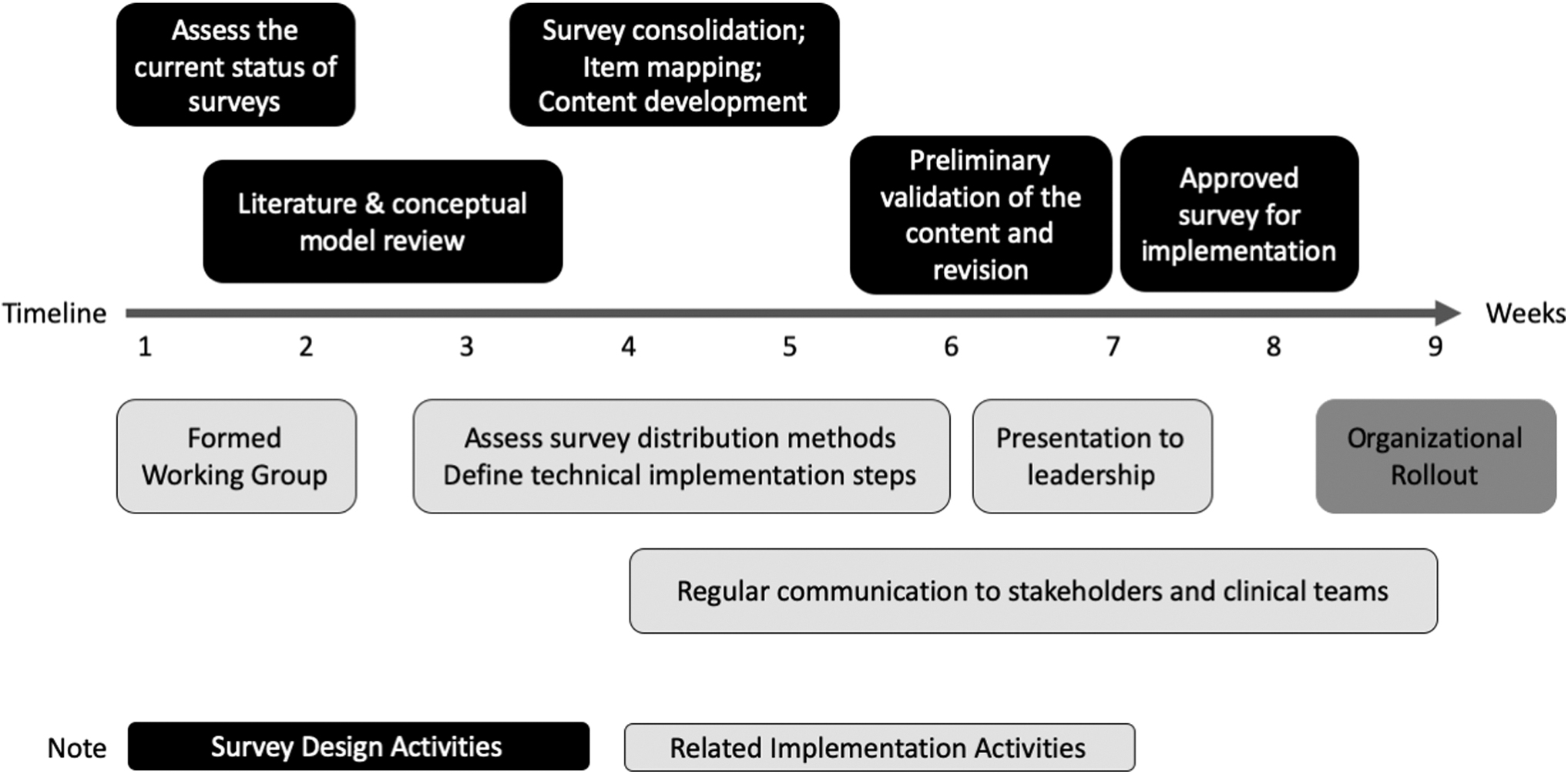
Timeline for survey development.
This study has been reviewed and approved by the Nationwide Children's Institutional Review Board (IRB No. 00001425).
LITERATURE REVIEW ON THEORETICAL FRAMEWORK
We conducted a rapid literature review on the conceptual models for patient satisfaction to develop a survey that matches well to a validated conceptual model. Due to time constraint, we did not conduct an exhaustive literature search, but instead handpicked publications based on conceptual model diagrams, instrument, and validation details provided. 7 –23 In addition to validation of the conceptual model, the working group considered other factors that may impact operational implementation, such as the frequency and length of the survey. These considerations are provided in Supplementary Table S1.
Following stakeholder deliberation, we decided to adapt the SERVPERF model as the theoretical framework on which to further develop our survey. We replaced the “tangible” construct in SERVPERF with telehealth usability to account for the change from physical to digital environment.
SURVEY ITEM MAPPING AND CONTENT DEVELOPMENT
We mapped the survey questions from the patient satisfaction surveys already developed by some of our clinical departments (four in total) (Supplementary Table S2) to the constructs in the adapted SERVPERF model through group consensus. This allowed us to consolidate similar items and identify gaps in survey coverage. For the constructs that are not well covered, we added items from other developed survey instruments to complete our initial survey design.
SURVEY REVIEW AND REVISION
To finalize the survey design, we presented the initial survey design to the working group, hospital leadership, as well as the NCH family advisory council. Feedback received was discussed with the working group in an iterative process. The finalized survey was reviewed by our literacy and education specialist for readability.
The survey was presented to the working group (n = 21) and the NCH Family Advisory Council (n = 37, including 24 parents) for review and revision. Key feedback from the working group included potential challenges encountered during telehealth visits as well as addressing ambiguity in the questions. Review by the Family Advisory Council ensures that the language and length of the survey are appropriate for our patients to complete with reasonable ease. The readability of the survey met the recommended sixth grade level. 24 In addition, the survey content was translated into four other predominant languages of our patient population, including Spanish, Somali, Nepali, and Arabic (Supplementary Table S3).
SURVEY DISTRIBUTION
Telehealth patient satisfaction survey (TPSS) was delivered automatically through HIPAA-compliant REDCap® Platform with unique survey link sent through MyChart Patient Portal messages after a video encounter was closed. To prevent survey fatigue, each patient was limited to receive one survey invitation in any 2-week period, regardless of number of visits. The survey can be completed by the patient or their caregivers. Each survey is linked to one specific encounter, with date and clinical department noted on the survey. In addition to 16 survey items to be validated as measures of patient satisfaction constructs (Table 1), some demographic questions were collected in the survey as well as directly extracted from the electronic medical record.
Telehealth Patient Satisfaction Survey
Patient Satisfaction Survey for Ambulatory Services (AMB).
Telehealth Patient Satisfaction Survey developed by Center for Surgical Outcome Research (CSOR).
Telehealth Usability Questionnaire (TUQ). 7
NA, not applicable.
Note: Superscripts denote the source survey instrument that the questions were derived from. The survey instruments referenced in this study are detailed in Supplementary Table S2.
SURVEY DATA SET
Our inclusion criteria were as follows: (1) patients of NCH and (2) patients who had completed a video visit at Nationwide Children's Hospital between July 7, 2020, and September 2, 2020. We collected 2,394 survey responses from 22,269 survey sent. Since some patients filled out the survey for different visits, we only selected their first response to ensure independent sample and reduce replicate responses for the purpose of analysis. Of the 2,394 responses, 1,938 responses fit our inclusion criteria.
DATA HANDLING
Survey responses are generally captured on a 5-point Likert scale, except the item comparing level of care between telemedicine appointment and in-person care. The responses for the item are “better/equal/worse/not sure/no in-person visit before,” which does not follow the symmetry and balance of Likert scale. To maintain uniformity of responses among all the items of the survey, we excluded this item for the EFA. 25 A few survey items had a “Not Applicable” (NA) response option (Table 1). We noted that one of these items, “If I had a long wait time, I was kept informed of those delays during my visit,” had 52% (∼1,244) of NA responses, which are mapped to “neither agree or disagree,” given the context of the question (Table 1).
This preserved data and prevented introducing bias by removing all those who did not have a long wait time. For the remainder of the survey questions, 482 (25%) had NA responses. For the factor analysis, we employed list wise deletion method, 26 that is, deleting all cases with a missing response, to handle these cases.
DATA ANALYSIS
We employed EFA to investigate the relationships between the survey items and explore item loading and grouping to inform the conceptual model.
Results
ADAPTED SERVPERF MODEL
Based on the comparison of existing conceptual models on service quality and patient satisfaction from our literature search (Supplementary Table S1), the SERVPERF model was chosen as the basis for our survey design, with modifications to address telehealth-specific components (Fig. 2). 27
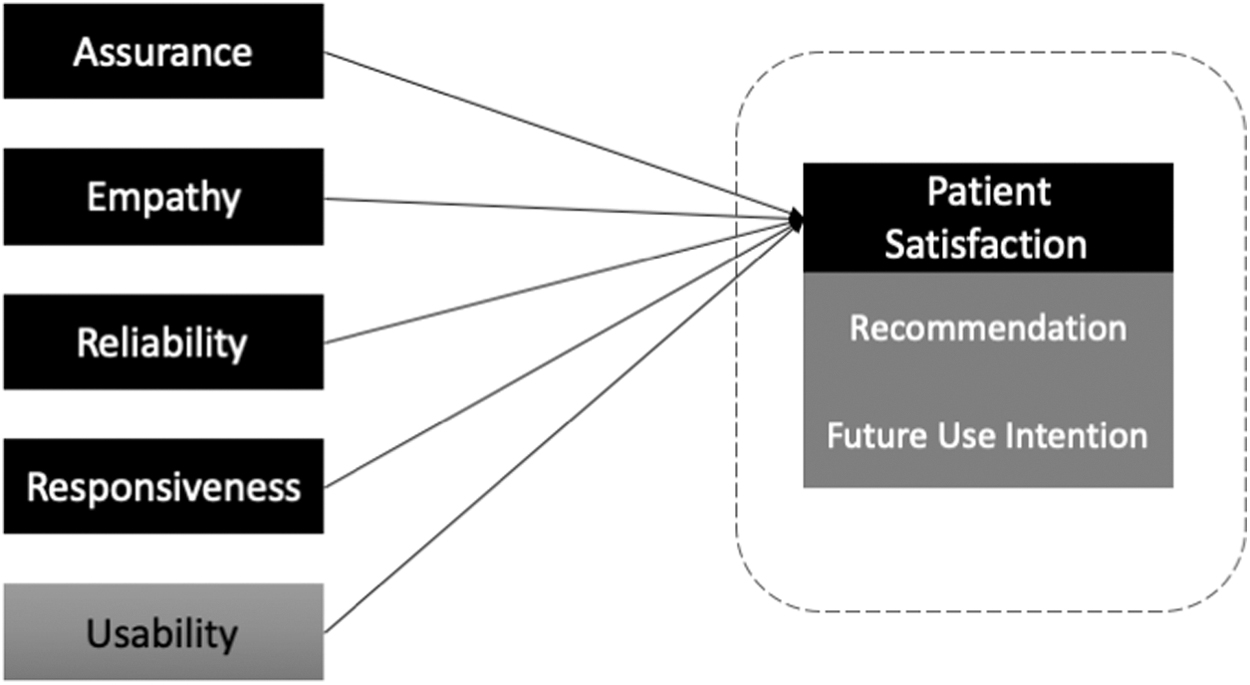
Adapted SERVPERF conceptual model.
The adapted model consists of four “service dimension” constructs from the SERVPERF model. 27 “Assurance” is related to the knowledge and courtesy of staff and their ability to inspire trust and confidence. “Empathy” is related to the caring, individualized attention the organization provides its patients. “Reliability” is related to the ability to perform the promised service dependably and accurately. “Responsiveness” is related to the willingness to help patients and provide prompt service.
We replaced the “Tangibles” construct that is related to the physical facilities, appearance of personnel, and the equipment of the hospital with the use of the telehealth system. The construct of “Usability” is based on the technology acceptance model, 28 and is related to the perceived usefulness and perceived ease of use. For the satisfaction construct, we included questions on overall experience, as well as future service use intention and word of mouth recommendation, which are highly correlated constructs. 7,29
SURVEY DEVELOPMENT
To reduce survey burden and increase response rate, we designed the survey to be easily responded within 5 min. Two to three items were included for each construct, along with questions on the challenges and the use of technology associated with telehealth to help us perform diagnostic analysis (Table 1).
DESCRIPTION ANALYSIS OF SURVEY PARTICIPANTS
Table 2 presents the sample characteristics for 1,938 patients whose telehealth visit experience were surveyed, as well as the demographic characteristics of all telehealth patients during that period. In most cases, the survey was completed by parents (85%). Patient characteristics for the sample were mostly white (75.4%), non-Hispanic or Latino (94.7%), and speaks English (96.0%). Notably, participants ranged in age from 0 to 62 years with mean age of 10 years (standard deviation [SD] 6.29). Although NCH is a pediatric hospital, patients with certain congenital conditions may continue to receive care into adulthood, in addition to a few other scenarios that adults may be cared for at NCH.
Telehealth Patient and Survey Participant Demographic
p-Value indicating statistically significant difference between the demographic characteristics of survey respondents and all telehealth patients.
The survey responses were collected from patients visiting 43 department specialties with 44.5% for Behavioral Health (including behavioral health, psychiatry and psychology) and 23.7% for the Clinical Therapy Specialties (including speech, occupational, and physical therapies). Compared to overall telehealth patient demographics, more white male patients and their families participated in the survey. In addition, we observed higher response rates from the Clinical Therapy Specialties.
DATA DISTRIBUTION
Distribution of data and weight of outliers are important properties that can affect factor analysis
EXPLORATORY FACTOR ANALYSIS
To extract relevant dimensions as factors, we used EFA. In the factor analysis, “groups of items that tend to be inter-related with one another more strongly than they relate to other groups of items will tend to form factors.” 34 We used Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy test and Bartlett's test of sphericity to test the sampling adequacy and examine whether the variables are measuring common factors or not. Our data have shown a high KMO index (0.94) and a significant Bartlett's statistic (Bartlett's K-squared = 3,279, p < 0.05), 35 indicating its suitability for factor analysis. Since our data violate the MVN distribution assumption, MINRES was used for factor extraction instead of the default maximum likelihood extraction method that assumes the MVN distribution of data 36 with Direct Oblimin rotation approach. 37,38
We expect the Eigenvalue to be >1 for factor extraction threshold 39 and conducted scree test with parallel analysis. The results from the Scree plot and parallel analysis indicated that our items correspond to three unobserved factors (constructs). 39,40 We considered the items with factor loadings >0.30 for our analysis. 41 Construct reliability was acceptable (Cronbach's alpha >0.6) (Table 3). 42
Factor Loading
We removed one item (“Informed of long wait time”) as the factor loading was below the cutoff of 0.30. There were no cross loadings of items observed. Factor 1 and Factor 2 had high reliability scores (Cronbach's alpha) of 0.93 and 0.83, whereas Factor 3 score (0.67) was reasonable. 43 The overall reliability score of the model was high with a Cronbach's alpha score of 0.91.
DEFINING CONSTRUCT
Reviewing the items within each factor and existing frameworks and literature, 12,24,44 –46 labels for the constructs were discussed by the authors and confirmed by consensus. Factor 1 consists of most items that reflect the patient/family's clinical encounter experience; we label it more broadly as “Perceived Quality of Service” and define it as “the patient/family's assessment of the overall excellence of the service.” The four items loaded to Factor 2 relate to telehealth, including the overall experience rating, future use, and perceived usefulness. Thus, Factor 2 closely relates to “Telehealth Satisfaction,” defined as “positive attitudes toward the use and value of telehealth.”
Factor 3 consists of two items, one about scheduling and the other about check-in to appointment, both relate to the process “before” the start of the clinical encounter. We thereby label the factor as “Admission Process” and define it as “subjective experience of the admission process that precedes receiving healthcare.” The three new factors can form a new conceptual model to be further validated.
Discussion
In this study, we describe the development of the TPSS that is generalizable across clinical disciplines. This is particularly useful for large health care organization. The advantage is manifold. First, the same survey can be delivered as an institutional effort, reducing duplication of effort and making implementation and analysis more efficient. Second, the survey allows for compilation and comparison between different service lines. Third, this centralized approach can set appropriate mechanism in place to reduce patients receiving multiple survey requests, for example, in our case, we set the logic to limit only one survey link be sent to patient within a 2-week period.
The TPSS development was operationally driven. Nevertheless, we leveraged a conceptual framework to inform our survey design as well as to reveal item relationships. While we initially matched our survey items to an adapted SERVPERF model, our factor analysis supports a new 3-factor model. We observed some degree of consistency between the two models (Tables 1 and 3): for instance, three questions on assurance and two questions on empathy were grouped into new Factor 1 (perceived quality of service), and two questions on usability were grouped into new Factor 2 (telehealth satisfaction). Several reasons may account for the difference.
First, we kept many of the questions from in-person patient experience survey as requested by clinical departments for ease of analyzing patient satisfaction regardless of mode of delivery. These different items were matched by the construct definition, but may not have adequate discriminative power to reflect different constructs. Second, we were able to use only two to three items for each construct, which may likely affect coverage of construct and the factor loadings. 47
Existing surveys on patient satisfaction, such as the Hospital Consumer Assessment of Healthcare Providers and Systems survey or survey based on SERVPERF, 27,48 focus primarily on the clinical experience and do not cover the usability aspect of telehealth care delivery. Moreover, these surveys do not consider home/nonclinical site as primary location. Often, the social determinants, including access to device, connectivity, and safe private space, are not considered.
Our survey includes a barrier question to identify the challenges associated with telehealth. The list of challenges and barriers was based on literature 49 and our clinical operational experience. Although this question is not considered part of our overall patient satisfaction conceptual model, it was deemed operationally relevant for more diagnostic analysis for future quality improvement effort.
LIMITATIONS
There are some limitations to the current survey. We recognize that some questions kept from previous internal surveys were double-barreled, which introduced ambiguity. These questions are “The provider was able to diagnose problems and treat my or my child's condition”; “I was given home care instructions and able to ask questions”; and “Overall, my needs were met. I would recommend others to Nationwide Children's Hospital.” While this approach is useful for comparison to historical data, we recommend others who plan to adopt this survey to separate the questions into two distinct questions to reduce ambiguity.
This survey delivery method, while operationally efficient through automation, imposes a “survivorship bias.” Patients who encountered sufficient challenges that prevented them from completing the telehealth visit were not surveyed. Nevertheless, for patients who are unable to initiate or conduct the telehealth visit, most of the questions in this survey will not be applicable. We recommend future studies to consider the challenges and experiences of those who declined or tried, but failed to have a telehealth visit. For example, we recently used clinical notes to study reasons of “just-in-time” (close to appointment time) canceled or rescheduled telehealth appointment, which revealed certain challenges in initiating telehealth visits. 50
The trade-off for a generic survey is that the questions may not be tailored for certain clinical service lines. A related limitation is that at the time of study, not all clinical service lines were offering telehealth visits. Since the volume of telehealth visits was different between clinical departments, the results may be skewed toward the high-volume clinical lines (e.g., behavioral health and clinical therapies). We also noted that the survey respondents were mostly White, English-speaking parents of young patients. This may affect the generalizability of the survey results. In addition, we used a single telehealth platform. Organizations using multiple platforms may need additional software-specific considerations.
FUTURE WORKS
Additional validation of survey items and conceptual model with confirmatory factor analysis and structural equation modeling is presented in a companion article. 51 We have also completed a separate survey for provider's view on telehealth, and future work will include a comparison of the provider and patient perspectives.
Conclusions
We developed a telehealth satisfaction survey based on operational guidelines, tested factor loadings and internal consistency, and eventually proposed a conceptual model to understand the patient satisfaction toward telehealth. It is versatile to be used across diverse clinical disciplines and covers both the clinical experience as well as the telehealth usability aspect. With the strong adoption of telehealth during the pandemic, telehealth is becoming not just a modality, but positioned to be a new “venue” or “setting” for providing health care. Well-designed survey to capture patient experience and pinpoint challenges is important to ensure high quality of health care delivery.
Footnotes
Authors' Contributions
S.L. conceived and presented the idea. E.-J.D.L., M.G., and E.S. drafted the article. M.G., E.S., and R.G. conducted data preparation and analysis. Collectively, E.-J.D.L., Y.H., L.M., J.L., U.R., and S.L. designed and implemented the survey. All authors contributed, critically reviewed, and revised the article. The final version of the article is approved by all authors.
Acknowledgments
We thank the Nationwide Children's Hospital telehealth committee and the family advisory team for contributing feedback to the design and implementation of the survey. The authors thank Sirina Lu and Sarah Wagner for supporting the technical implementation of the survey. They also thank Dr. Megan Gregory for helpful discussion and the NCH transcription services for survey translation.
Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding information to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.