
Abstract
Background:
The advance in digital media technologies has enabled the development of technologically mediated health care solutions. Mobile health app for mental health care is one of such innovative tools to monitor and manage users' mental health and psychological well-being.
Objective:
This study examines the factors predicting the acceptance of mental health app (MHA) that are: technological (i.e., perceived ease of use and perceived usefulness) and sociocultural (i.e., perceived stigma toward mental health treatment and prior experience of face-to-face mental health service utilization).
Methods:
Using structural equation modeling, we tested an extended Technology Acceptance Model with data from the Healthy Minds Study, a web-based national survey of U.S. college students (N = 429).
Results:
In addition to the technological factors, the sociocultural factors significantly influenced MHA acceptance. Notably, college students with higher levels of stigma toward mental health treatment were less likely to have experience of using face-to-face mental health service. This, in turn, led to more openness to accepting MHA that does not involve in-person visits but rather private and mediated communication.
Conclusions:
Findings of this study provide critical insight into the increasing needs for and use of mobile apps for mental health care. Implications are discussed and future research directions are suggested.
Introduction
Mental health problems pose one of the most serious and pervasive public health challenges in recent years. With more than million people worldwide experiencing depression, 1 interventions are increasingly leveraging digital health technologies such as mobile apps to help people self-manage their mental well-being. The growing prevalence of mental health problems among college students, 2 in particular, has led to numerous endeavors from researchers and practitioners. One innovative approach is through smartphone- or tablet-based mobile health (m-health) applications that are designed to track or treat users' mental health conditions, which are touted for their increased convenience, accessibility, and flexibility among college students. 3
The rapidly escalating COVID-19 pandemic and social distancing requirements have exacerbated mental health problems while posing difficulty to in-person support, 4,5 witnessing a surge in mental health app (MHA) downloads. 6 MHA provides programs to manage users' mental health in real time and offer mediated interventions or treatments, potentially serving as an adjunct to face-to-face therapy while improving patients' adherence to existing treatment practices for health conditions such as anxiety disorders. 7,8 Studies have also shown the MHA's feasibility for stress and anxiety management by integrating prevention strategies and personal monitoring into users' everyday life. 9 –11 Indeed, an extra layer of privacy and anonymity provided by MHA compared with in-person psychotherapy was found to increase the treatment rates especially among people battling with mental health stigma. 12
Research to date has drawn upon Technology Acceptance Model (TAM) 13,14 to identify an array of factors that predict the acceptance of MHA. However, prior studies have largely taken a technological perspective while overlooking sociocultural context surrounding the MHA acceptance. Informed by earlier findings of mental health interventions, 15 we proposed and tested an extended TAM to incorporate sociocultural variables, 16 specifically the stigma underlying mental health issues and mental health service utilization to better understand MHA acceptance. This research contributes to a more nuanced understanding of the MHA, a burgeoning m-health tool for mental health management and intervention.
TECHNOLOGICAL DETERMINANTS OF MHA ACCEPTANCE
TAM offers a framework for identifying factors that may impact technology acceptance. It posits that perceived ease of use (i.e., whether using the technology is free of effort) and perceived usefulness (i.e., whether the technology will enhance one's performance) are key predictors of individuals' intent to accept the technology. 13,14 Previous studies have found that perceived ease of use influences technology acceptance through perceived usefulness, 17 –19 highlighting that individuals perceive a technology to be more useful as they find it easy to use.
Recently, TAM helped explain the intent to accept m-health apps for specific populations (e.g., health care professionals)
20
or issues (e.g., obesity management).
18
Taken together, the TAM literature suggests that individuals are more likely to accept apps that they perceive to be easy to use and thus useful. Given that behavioral intent has long been recognized as an effective proxy measure of actual behavior,
13
we propose the following three hypotheses in predicting the intent to accept MHA:
CONTEXTUAL FACTORS TO CONSIDER BEYOND TECHNOLOGICAL DETERMINANTS
In the United States, young adults aged 18–25 years show the highest prevalence of major depressive episodes. 21 Moreover, many people with mental health problems do not report their symptoms or even recognize them as problematic, partially due to the negative stereotypes or social stigma toward people with mental health problems. 22 Widespread stigma and negative stereotypes include the ideas that having mental health problems such as depression is being weak, inferior, incompetent, or vulnerable, and that the condition is shameful, embarrassing, or socially unacceptable. 23,24
Indeed, such stigma has been found to be a key barrier to the perceived need for help, and more importantly treatment-seeking behavior, including mental health service utilization. 25 For instance, college students dealing with severe or recurrent depression were reluctant to seek treatment due to fears of being judged if they seek help. 26 More recently, a study across 2009–2015 revealed that college students' greater perception of stigma toward mental health treatment was negatively associated the use of mental health service. 27
Against this backdrop, the convenience and confidentiality that MHA provides may appeal to students with concerns about stigmatization. For example, a study found that young adolescents valued MHA mostly for its keeping users safe from cyberbullying and further stigmatization. 28 In another study, the primary reason for college students to prefer MHA over traditional psychotherapy was convenience, followed by anonymity/reduced stigma, immediate availability, and cost savings, 29 suggesting that students who perceive a greater stigma around mental health services and thus have little experience of in-person mental health service would be more open to using MHA.
Nevertheless, how these contextual factors (e.g., stigma toward and use of mental health treatment) may affect individuals' willingness to adopt and use MHA remains unexplored in tandem with the TAM framework. Traditional technological perspectives only consider user perceptions toward technology itself (e.g., perceived ease of use or usefulness of apps), missing out crucial context surrounding the overall mental health care. Therefore, we propose an extended model that synthesizes the TAM and two contextual factors associated with MHA acceptance, that is, mental health service utilization and perceived stigma. We based our model specifications on the TAM framework and the body of empirical findings on the effects of stigmatizing attitudes and mental health service use on MHA (Fig. 1):
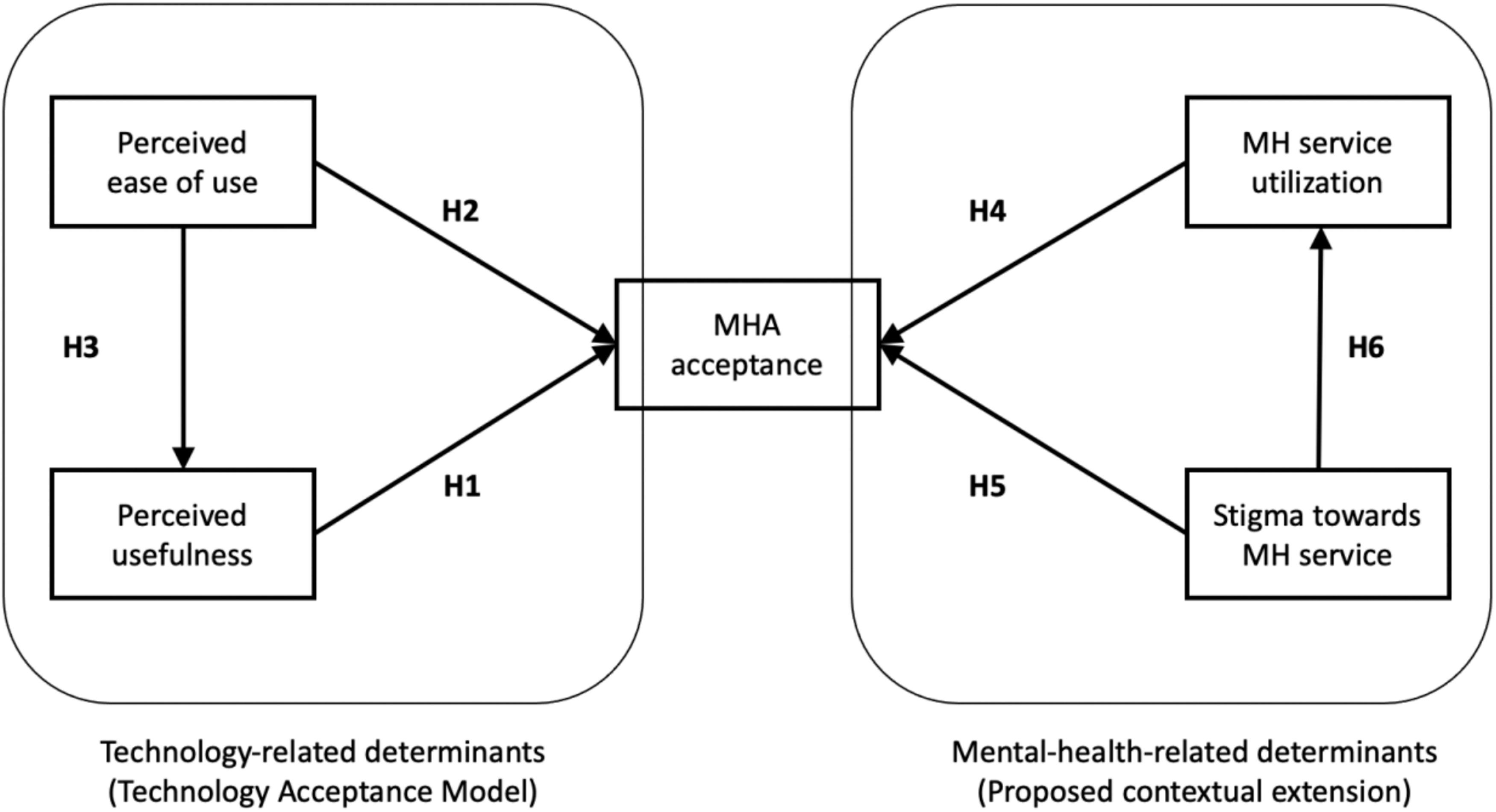
Hypothesized model (TAM with contextual factors). MH, mental health; MHA, mental health app; TAM, Technology Acceptance Model.
Methods
DATA
This study used data from the Healthy Minds Study (HMS), an annual web-based survey examining mental health, service utilization, and related issues among university students aged ≥18 years in the United States. The HMS was approved by the University of Michigan Institutional Review Board and administered at multiple colleges and universities across the U.S. Survey respondents were randomly selected from their respective schools to receive e-mail invitations to participate in the study and provided consent for their data to be used in research. In this study, upon the Data Request Form, 30 we retrieved a deidentified archival data set collected in the 2018–2019 academic year from the Healthy Minds Network research team. The data set contained the responses of students from 79 participating schools. 31
PROCEDURE AND PARTICIPANTS
Out of the 876 students who started the survey, 721 (97.3%) indicated ownership of a smartphone and 429 participants indicated no experience of using MHA. These 429 students were included for analysis in this study given that our outcome variable of interest is behavioral intent, MHA acceptance.
Participants were presented with the definition of MHA in the beginning of the survey: “A mobile application that is designed to track or treat a mental health condition (e.g., depression, anxiety, psychosis, personality disorder, bipolar disorder, insomnia, post-traumatic stress disorder, substance use disorder, eating disorder, ADHD, etc.). This does not include an app that would relate to other aspects of wellness (diet, exercise, stress, general health). Examples of mental health apps include but are not limited to: Talkspace, SAM, Moodkit, PTSD Coach, CBT-I Coach, Operation Reach Out, Optimism.” Participants were on average 23.53 years old (standard deviation = 5.58), predominantly female (61.3%) and white (78.3%) followed by Asian (11.9%), Hispanic (7.2%), Middle Eastern (5.4%), and African American (4.7%).
MEASURES
MHA acceptance
HMS measured MHA acceptance through the question: “Would you prefer to use a mental health app instead of seeing a mental health professional if you were experiencing a mental health condition?” (1 = No, 2 = Maybe, 3 = Yes).
Perceived ease of use
Two items were used to measure the perceived ease of MHA use: “If I wanted to seek out a wellness or mental/emotional health app, I would know how to find an app I could trust”; “If I wanted to seek out a smartphone app for my mental/emotional health, I would know what kind of app to look for, given my needs” (1 = Strongly disagree; 6 = Strongly agree). These items were significantly correlated, r = 0.72, p < 0.001.
Perceived usefulness
Perceived usefulness was measured with the question: “How helpful on average do you think wellness or mental/emotional health apps are for people your age who are having mental or emotional health problems?” (1 = Not helpful; 4 = Very helpful).
Stigma
HMS measured stigma toward mental health service utilization using a single item indicator: “I would think less of a person who has received mental health treatment” (1 = Strongly disagree, 6 = Strongly agree).
Mental health service utilization
Participants' experience of mental health service utilization was measured with a single item: “How many total visits or sessions for counseling or therapy have you had in the past 12 months?” (1 = Never, 2 = 1–3 times, 3 = 4–6 times, 4 = 7–9 times, 5 = 10 times or more).
Results
Structural equation modeling analyses were performed to test the hypotheses using the lavaan package in R. 32 The overall chi-square test of model fit was statistically nonsignificant, χ 2 (7) = 4.54, p = 0.712. The comparative fit index was 1.000. The root mean square error of approximation was 0.000, 90% confidence interval (CI) [0.000 to 0.045], and the p value for the test of close fit was 0.97. The standardized root mean square residual was 0.015.
In sum, the indices consistently demonstrated that our extended TAM model was a good fit to the data. Also, this model was found to be a better-fit model (Akaike Information Criterion [AIC] = 6,157.987) than a model with the original TAM constructs only (AIC = 6,168.093). The AIC penalizes model with more parameters thereby a lower score suggests more parsimony that explains a greater amount of variation using the fewest possible variables.
Figure 2 summarizes the model results. Students high on the perceived ease of use found MHA more useful, β = 157, p < 0.001, 95% CI [0.086 to 0.229], which led to a greater intent to accept MHA, β = 0.169, p = 0.001, 95% CI [0.061 to 0.276], indirect effects coefficient = 0.027, p = 0.006. Similarly, students high on the mental health stigma were less likely to use in-person services in the past year, β = −0.270, p = 0.014, 95% CI [−0.511 to −0.029], which in turn predicted their MHA acceptance intent, β = −0.133, p < 0.001, 95% CI [−0.207 to −0.059], indirect effects coefficient = 0.036, p = 0.036.

Summary results of structural equation modeling of mental health app acceptance. Note: Standardized path coefficients for the analyzed model. *p < 0.05, ***p < 0.001. Solid lines represent significant results, whereas dotted lines represent nonsignificant results. χ 2 (15, 429) = 359.806, p < 0.001; CFI = 1.000; RMSEA = 0.000 (0.000–0.045); SRMR = 0.015. CFI, comparative fit index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual.
Meanwhile, the difference between these two indirect effects was not significant, p = 0.682, indicating equal predictive powers of the two paths. The direct effects of perceived ease of use, β = 0.025, p = 0.292, 95% CI [−0.058 to 0.107], and the stigma toward mental health service, β = 0.015, p = 0.356, 95% CI [−0.065 to 0.095], on MHA acceptance were both nonsignificant.
Therefore, results showed that the acceptance of MHA was positively predicted by the perceived usefulness (H1 supported), but not by the perceived ease of use (H2 rejected), while confirming the positive relationship between perceived ease of use and usefulness (H3 supported). In addition, MHA acceptance was predicted by the lower level of in-person mental health service utilization within a year (H4 supported), but not directly predicted by the stigma toward in-person mental health service itself (H5 rejected), while confirming the significant effects of stigma on the reluctance of mental health service utilization (H6 supported).
Discussion
Given a growing need for and use of technologically mediated health care solutions, this study contributes to the understanding of the mechanism surrounding the use of MHA, a burgeoning m-health tool to monitor and manage users' mental health and psychological well-being. The findings presented in this study advance the existing literature and practices of mental health management and intervention that are digitally mediated through mobile technologies.
The TAM highlights attitudes toward technology (e.g., “perceived ease of use” and “perceived usefulness”) as the key determinants of technology adoption and use. When it comes to MHA that has a specific goal of managing mental health compared with other technologies, simply relying on the technological determinants to predict MHA acceptance may miss out on important effects of other contextual factors underlying MHA acceptance. To address this gap, this study proposed incorporating individuals' perceived stigma toward mental health treatment and their service utilization into the TAM and tested the model using 2018–2019 HMS data. Our findings demonstrate the promise of the extended TAM, contributing to a more nuanced understanding of MHA acceptance.
In addition to the support of technological determinants of MHA acceptance, we found that college students with greater stigma toward mental health treatment were less likely to have experience of using face-to-face mental health service in the past year, which in turn led to more openness to MHA use. This is consistent with previous findings on the negative relationship between stigma and intention to seek professional help. 33,34 Interestingly, however, our results show that the stigma was not a direct barrier to the MHA acceptance.
Instead, stigma was indirectly, yet positively, related to MHA acceptance through the lower level of in-person service utilization, pointing to the possibility that MHA may work as a technological substitute for in-person psychotherapy. Indeed, college students who are unwilling to seek professional help from therapists were found to be still open to self-help tools such as mobile MHA. 35 Therefore, MHA may serve as an alternative to face-to-face counseling, providing less intimidating and intense experiences enabled by the mediated and private format.
Notably, our findings revealed that there was no significant difference in the indirect effects of technology determinants (i.e., perceived ease of use → perceived usefulness → MHA acceptance) and of sociocultural determinants (i.e., stigma → mental health service utilization → MHA acceptance). That is, the two paths seem equally important, suggesting the importance of simultaneously considering technological and sociocultural determinants in intent for technology acceptance. 16
There are study limitations worthy of note. First, this study relied on a random sample of students from 79 participating schools in the United States, not a complete census of the student population. In addition, our sample was largely composed of white students (78.3%). Therefore, it should be noted that our sample is not nationally representative of all schools or students in the United States. Future research with more diverse groups of students may consider racial 36 and cultural 37,38 differences in predicting the MHA acceptance. Second, the interpretation of our findings should consider the limitations from the use of secondary data, that is, the research group was not involved in the questionnaire design, and thus the fit between research questions and the data available as well as the single-itemed measures should be noted. For instance, our measure of mental health service utilization was limited to the past 12 months, thus caution should be taken in interpreting the results.
In addition, our outcome variable was behavioral intent, not the actual behavior. Although behavioral intent is a strong predictor of actual behavior 39 and thus widely used in research as a valid proxy measure for behavior, 16,40 it would be meaningful for future research to examine how this intent leads to actual use using longitudinal data. This could be also addressed by studying an actual MHA user group with additional measure of their experience with MHA and examining how it may interact with their in-person mental health service-related attitudes and experience to jointly influence MHA use. Replicating our model in different settings and populations will strengthen the external validity of our findings on the relationships among the MHA acceptance-related variables.
Conclusions
This study recognizes the role of user perceptions of the technology itself, and more importantly sheds light on the contextual factors surrounding the technology use. The acceptance of m-health apps for mental health care is a decision based not merely on individuals' perception of the technology itself, but also on their contextual understanding of mental health and care. MHA allows mental health management at one's convenience at fingertips, highlighting anonymity and self-efficacy of controlling the treatment process, all of which may constitute advantage over in-person mental health consultation as this study demonstrated. Future research on MHA will benefit from an extended TAM that incorporates sociocultural factors, namely, mental-health-related stigma and face-to-face treatment experience.
Footnotes
Acknowledgment
The authors would like to thank Margaret McLaughlin for insightful feedback.
Disclosure Statement
No potential of conflict of interest was reported by the authors.
Funding Information
No funding was received for this article.