
Abstract
Introduction:
Patient participation and clinical outcomes of a precoronavirus disease 2019 (COVID-19) office-based transdiagnostic psychiatric intensive outpatient program (IOP) were compared with those of telehealth IOP during COVID-19.
Materials and Methods:
Weeks of enrollment, Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7) assessments, and sociodemographic and clinical factors (including group track and diagnosis) were collected during pre-COVID-19 (n = 191) and during COVID-19 (n = 200). Continuous and categorical measures of GAD-7 and PHQ-9 were analyzed; potential sociodemographic and clinical covariates to scores were also explored.
Results:
There were no statistically significant differences in participation between time periods. Associations were observed between PHQ-9/GAD-7 score improvement and number of assessments. Significant score reductions occurred in both periods, and differences in change scores were not significant. Sociodemographic and clinical factors were not significantly different between time periods. Patients with commercial insurance had significantly higher improvement in both mean and categorical PHQ-9 scores (t = 2.77, p = 0.006; χ2 = 10.47, df = 1, p = 0.001) and GAD-7 scores (t = 2.29, p = 0.023; χ2 = 8.58, df = 1, p = 0.003) than those with public insurance. Patients with anxiety disorders had significantly greater improvements (F = 4.49, p = 0.004; χ2 = 9.15, df = 3, p = 0.027) in GAD-7 during COVID-19.
Discussion:
Significant improvements in PHQ-9/GAD-7 scores and measures of participation were not significantly different between telehealth and office-based IOP, nor were they greatly influenced by clinical or sociodemographic factors. Further study is needed of possible care disparities for publicly insured patients.
Conclusion:
Despite some limitations, telehealth IOP appears to be a clinically appropriate option for a diverse sociodemographic and diagnostically heterogeneous psychiatric population.
Introduction
W
Both specialized and transdiagnostic IOPs have been offered through telehealth during the COVID-19 pandemic. 4 –8 In at least one telehealth-based partial hospitalization program, which operates similarly to IOP but with daily services, patient satisfaction ratings were equal to those of in-person services. 9 High attendance rates in telehealth IOP groups have also been demonstrated. 5 Despite these early measures of success, evidence around clinical effectiveness of telehealth IOP is limited. In addition, concerns that, in vulnerable groups, telehealth will only exacerbate existing health care disparities have been postulated. 5,10
Our academic medical center offers a large transdiagnostic general adult IOP with eight tracks, each serving between 9 and 12 individuals with primary mood, anxiety, trauma, or personality disorders. Most patients are <65 years old. All patients receive 3 h of group therapy daily, 3 days a week; hourly weekly individual therapy; and weekly assessment and management by a psychiatrist. As part of routine clinical care, each patient completes a Generalized Anxiety Disorder-7 (GAD-7) questionnaire and a Patient Health Questionnaire-9 (PHQ-9) weekly. 11,12 Changes in scores are monitored to track symptomatic improvement in depression and anxiety over time; validation of these assessment measures in transdiagnostic groups in psychiatric partial hospitals was reported previously. 13,14
Starting March 15, 2020, all IOP tracks at our medical center were offered through telehealth as part of an institutional response to the COVID-19 pandemic. Office-based IOP was immediately suspended. Nearly all patients engaged with online video platform services (Microsoft Teams® and Vidyo®); very few patients connected by telephone. All continued to receive weekly GAD-7 and PHQ-9 assessments.
This report represents the findings of a quality improvement project conducted to examine for differences in patient IOP participation and clinical outcomes, measured by GAD-7 and PHQ-9 scores, before and after COVID-19–related changes in treatment delivery were instituted. A secondary aim was to determine whether any specific patient sociodemographic or clinical factors impacted IOP participation and PHQ-9/GAD-7 change scores with treatment, specifically during the COVID-19 telehealth visit period and in comparison with when office-based visits were conducted prepandemic.
Materials and Methods
This quality improvement initiative was approved by the University of Pittsburgh Medical Centre (UPMC) quality review committee, separate Institutional Review Board approval was not required. PHQ-9 and GAD-7 scores were culled from the electronic medical record Epic for all patients who participated in 1 of 11 adult IOP tracks, starting with the pre-COVID-19 period of January 1, 2020, to March 15, 2020, and then extending from March 15, 2020, to June 30, 2020, during the COVID-19 period. Patients who started IOP before March 15, 2020, but continued thereafter were included in the pre-COVID-19 period. Weeks of enrollment were obtained from administrative documents, as were number of assessments completed. We used both as measures of patient participation. Sociodemographic and clinical data related to patient age, race, legal gender, diagnosis, federal poverty level of zip code of primary address, and primary insurance type were also obtained.
For purposes of analysis, patient race was categorized as Caucasian, African American/Black, or Other. “Other” included patients of Hispanic, Asian, Native American, and unreported race. Legal gender was male or female. Each patient's primary insurance was categorized as commercial or public. Individuals with Medicare with a secondary private insurance were classified as having commercial insurance. All other Medicare and Medicaid recipients were classified as publicly insured. Individuals listed as self-pay were excluded from the analysis due to small sample size (n = 7).
Primary billing diagnosis at patient enrollment was collected, and the following diagnostic groups were created (and were inclusive of the listed diagnoses): depressive disorders (major depressive and persistent depressive disorders), bipolar disorders (bipolar I, bipolar II, and unspecified bipolar disorders), anxiety disorders (generalized anxiety and panic disorders), and other (borderline personality, post-traumatic stress, hallucinogen use, other psychotic, eating, and adjustment disorders). Two patients with schizoaffective disorder were excluded from analysis.
Each of the eight IOP tracks was also categorized into one of three groups. The general mood and anxiety disorders grouping was the largest (seven tracks), followed by the high complexity grouping (two tracks; patients had primary or comorbid borderline personality disorder), and the bipolar grouping (one track). Finally, patients' zip codes were analyzed through the U.S. census database (
Statistical analysis was carried out using SPSS Version 26.0. Sociodemographic, clinical characteristics, and type of IOP attendance were examined for the pre-COVID-19 and during COVID-19 time periods using bivariate statistics, namely independent and matched t tests for continuous measures and contingency tests (chi-square or Fisher's exact) for categorical measures.
Two measures for changes in anxiety (GAD-7) and depression (PHQ-9) scores were employed—a continuous change measure, calculated as the absolute difference between the final and initial PHQ-9 and GAD-7 scores, and a categorical measure that represented a change in GAD-7 and PHQ-9 severity as established by conventional norms. “Improvement” was assessed if the final severity category for GAD-7 or PHQ-9 was of a lower severity that the baseline category for the respective scale, and “no improvement” if the final category was the same or higher than baseline.
General linear models were used to examine factors and covariates associated with changes in GAD-7 and PHQ-9 scores as continuous measures, and logistic regression models were used to examine predictors for categorical improvement in GAD-7 or PHQ-9. Student's t tests or one-way analyses of variance using groups based on gender, race, and types of insurance, poverty level, or IOP track assignment were employed to examine changes in GAD-7 or PHQ-9 scores relating to those characteristics. Significance was determined using an alpha set at 0.05.
Results
Between January 1, 2020, and June 30, 2020, 393 patients attended IOP. Two patients with schizoaffective disorder were excluded from analysis. Of the remaining 391 patients, 389 had at least one GAD-7 assessment, and 388 had at least one PHQ-9 assessment. In total, 191 patients started IOP between January 1, 2020, and March 15, 2020 (pre-COVID-19 time period), and 200 patients started between March 16, 2020, and June 30, 2020 (during COVID-19 time period). Change scores for GAD-7 and PHQ-9 as both continuous and categorical measures were calculated as already described. In instances where only one assessment for GAD-7 or PHQ-9 was available, a “last observation carried forward” (LOCF) strategy was used to impute the final score to eliminate bias.
The average number (±standard deviation [SD]) of weeks of patient enrollment in the pre-COVID-19 time period was 3.9 ± 7.6, which was not statistically different from during the COVID-19 time period (4.9 ± 8.9 weeks). Similarly, the mean number of GAD-7 and PHQ-9 assessments completed per patients was statistically equivalent between time periods (3.25 ± 2.3 in the pre-COVID-19 and 2.84 ± 2.4 in the COVID-19 time periods). The sample comprised 140 (36%) male and 251 (64%) female patients. The mean age (±SD) of the sample was 33.1 ± 12.5 years with a range of 18 to 78 years. Most patients were Caucasian 297 (76%), 67 (17%) were African American, and 27 (7%) were of other races.
Depressive disorders accounted for 55% of all diagnoses, followed by bipolar (19.9%), anxiety (15.1%), and other disorders (10%). Fourteen percent of patients lived in zip codes with poverty level <5%, 66% lived in zip codes with poverty level 5% to 20%, and 20% lived in zip codes with poverty level >20%. Insurance information was available on 369 patients of whom 71% had commercial insurance, 27.1% had public insurance, and 9% were self-pay. Twenty-two patients (5.6%) had missing insurance information.
Most patients (71.1%) attended general mood/anxiety disorder IOP groups, 18% attended high complexity groups, and 10.8% attended bipolar IOP group. Group information was not available for three patients. There were no significant differences in the distribution of any of these sociodemographic or clinical characteristics between the pre-COVID-19 and during COVID-19 time periods (Table 1).
Sociodemographic and Clinical Characteristics for Patients (
Gender listed in the chart, generally indicative of legal gender.
Includes patients identifying as Hispanic, Asian, and Native American.
COVID, coronavirus disease; SES, socioeconomic status.
Although there were no significant differences in the initial or final mean PHQ-9 scores across the entire period, or in either the pre-COVID-19 or COVID-19 time periods, the mean initial GAD-7 score in the COVID-19 period was significantly higher than the mean initial GAD-7 score in the pre-COVID-19 period (t = 2.1, p = 0.038). Final GAD-7 scores, however, were not significantly different between the two time periods (t = 1.6, p = 0.100). Significant reductions were observed in the mean GAD-7 and PHQ-9 scores in both the pre-COVID-19 and COVID-19 periods (Table 2), and the differences in change scores between the two time periods were not significant.
Changes on GAD-7 and PHQ-9 Scores in Pre-COVID-19 and COVID-19 Periods
GAD-7, Generalized Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9; SD, standard deviation.
However, an examination of GAD-7 and PHQ-9 improvement based on categorical change scores showed that significantly more patients had PHQ-9 improvement in the pre-COVID-19 period (46.8%) than in the period during COVID-19 (37.0%). No difference in categorically determined improvement between time periods was observed for GAD-7 (Table 3).
Comparison of GAD-7 and PHQ-9 Scores in the Pre-COVID-19 and COVID-19 Periods
ns, nonsignificant.
The associations between sociodemographic and clinical characteristics with mean or categorical changes in GAD-7 and PHQ-9 scores were examined. Although there were no statistically significant differences in the mean ages of the pre-COVID-19 and COVID-19 groups, all patients aged 65 years and older (n = 6) participated only during the pre-COVID-19 period (Fisher's exact two-tailed p = 0.013). Nonetheless, there were no significant associations between age and improvements in either mean or categorical GAD-7 or PHQ-9 scores in either period.
Overall, female patients had significantly higher mean baseline and final GAD-7 scores than male patients, though significant differences were notable only for the baseline GAD-7 scores during the COVID-19 time period. Moreover, there were no overall gender differences in either the mean or categorical GAD-7 or PHQ-7 improvement across the whole observation period and during either the pre-COVID-19 or COVID-19 time periods. Similarly, there were no overall or pre-COVID-19/COVID-19 time period racial differences in mean or categorical GAD-7 or PHQ-9 improvement.
Although there were no overall differences in score changes for the two measures based on diagnosis, patients with anxiety spectrum disorders in the COVID-19 time period had significantly higher improvements in mean (F = 4.49, p = 0.004) and categorically determined changes (χ 2 = 9.15, df = 3, p = 0.027) in GAD-7 (Fig. 1). Assignment based on IOP tracks did not show any overall differences, however, mean GAD-7 score improvement was significantly higher for patients in the general mood/anxiety and bipolar groupings in the pre-COVID-19 period (F = 3.40, p = 0.035). In addition, categorical improvement in PHQ-9 scores was observed for the same IOP tracks in the pre-COVID-19 time period (χ 2 = 10.59, df = 2, p = 0.005).

GAD-7 categorical improvements by diagnostic grouping. The percentage of patients whose GAD-7 scores improved from baseline versus the percentage of patients who did not improve is depicted. Patients are separated into diagnostic groups and by the time period in which they participated in IOP, that is, pre-COVID-19 or during COVID-19. Patients with anxiety spectrum disorders in the COVID-19 time period had significantly higher improvements in mean change and categorical change, and as shown, a higher percentage of patients improved on GAD-7. COVID-19, coronavirus disease 2019; GAD-7, Generalized Anxiety Disorder-7; IOP, intensive outpatient program.
Patients with commercial insurance had significantly higher improvement in both mean and categorical PHQ-9 scores (t = 2.77, p = 0.006; χ 2 = 10.47, df = 1, p = 0.001) and GAD-7 scores (t = 2.29, p = 0.023; χ 2 = 8.58, df = 1, p = 0.003) when compared with those with public insurance. In comparing the pre-COVID-19 with the COVID-19 time period, only in the COVID-19 time period did patients with commercial insurance demonstrate statistically greater improvement in mean and categorically determined GAD-7 (t = 2.31, p = 0.023; χ 2 = 8.20, df = 1, p = 0.004) and PHQ-9 scores (t = 2.44, p = 0.016; χ 2 = 7.81, df = 1, p = 0.005) ( Figs. 2 and 3 ).

Changes in GAD-7 scores by insurance grouping. Pre–post changes in mean GAD-7 scores between public and commercially insured cohorts in the pre-COVID-19 and COVID-19 time periods are illustrated. During the COVID-19 time period, patients with commercial insurance had statistically greater improvement in mean GAD-7 scores (t = 2.31, p = 0.023) than did publicly insured patients. GAD-7, generalized anxiety disorder-7.
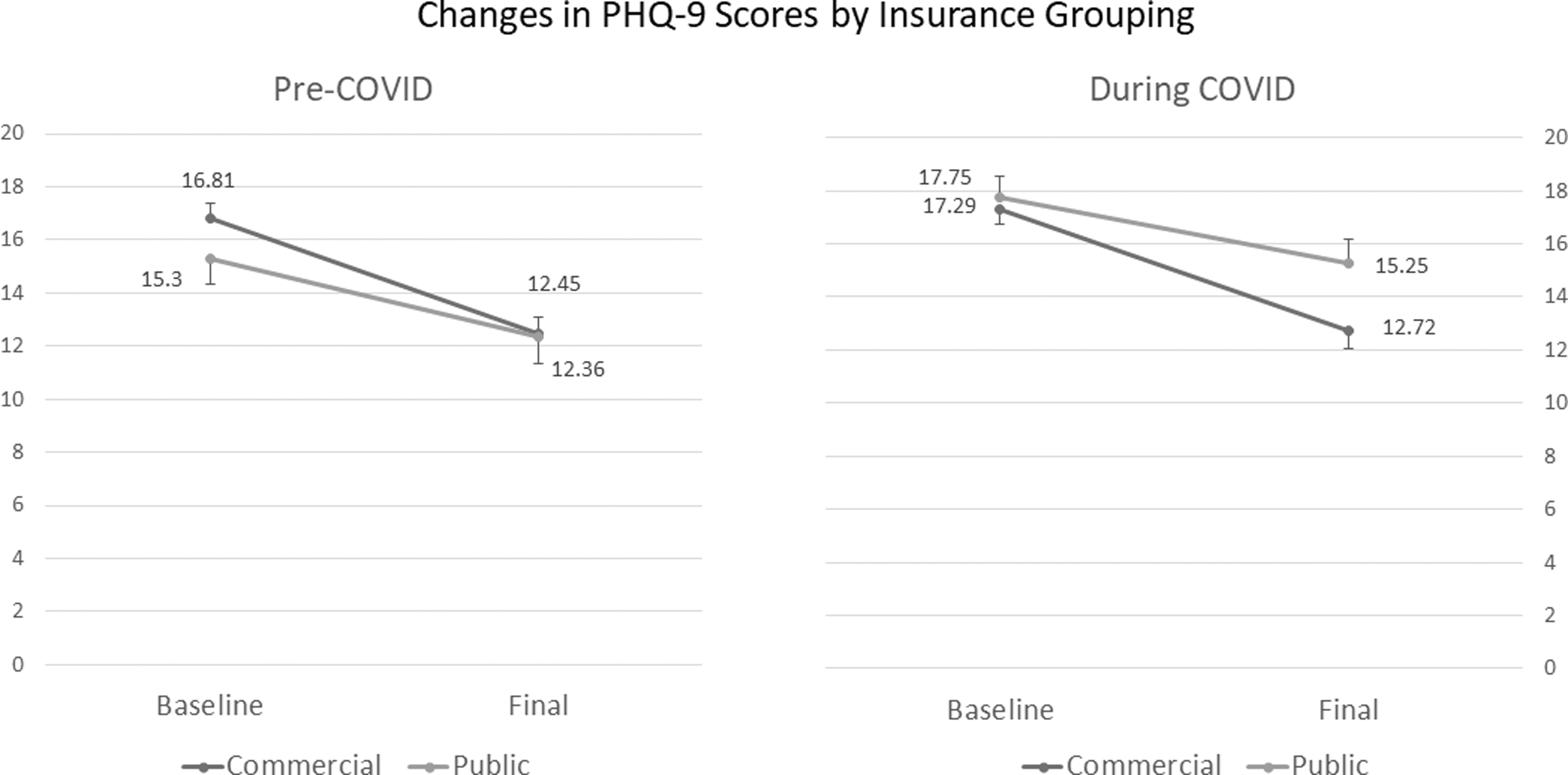
Changes in PHQ-9 scores by insurance grouping. Pre–post changes in mean PHQ-9 scores between public and commercially insured cohorts in the pre-COVID-19 and COVID-19 time periods are illustrated. During the COVID-19 time period, patients with commercial insurance had statistically greater improvement in mean PHQ-9 scores (t = 2.44, p = 0.016) than did publicly insured patients. PHQ-9, Patient Health Questionnaire-9.
In the pre-COVID-19 period, patients with commercial insurance had significantly more weeks enrolled than publicly insured patients (t = 2.75, p = 0.007); there were no significant differences in weeks enrolled between these groups during the COVID-19 time period. Mean number of assessments completed was not statistically different between the commercially and publicly insured groups in the pre-COVID-19 period. However, during the COVID-19 time period, mean number of assessments for the commercially insured group was significantly higher than for the publicly insured group (t = 2.54, p = 0.012). There were no overall or time period effects of zip code-based poverty characteristics on changes in mean or categorical GAD-7 or PHQ-9 scores.
There were no statistically significant differences in the number of times GAD-7 and PHQ-9 scales were administered during the pre-COVID-19 and COVID-19 periods, and significant associations were observed between improvement in GAD-7 and PHQ-9 scores and number of assessments completed (Table 4). Multivariate statistics using mean GAD-7 or PHQ-9 score changes or categorical improvements in either measure as dependent variables also confirmed number of assessments completed as the most significant predictor of score improvement.
Assessment Completion (Mean ± SD) and Improvement in GAD-7 or PHQ-9
Discussion
Expanding on previously reported census and patient satisfaction findings for IOP telehealth groups during the COVID-19 pandemic, 5,9 our study compares clinical outcomes of pre-COVID-19 office based to COVID-19 telehealth in a large transdiagnostic IOP. Unsurprisingly, GAD-7 scores were higher during COVID-19 at IOP entry, consistent with higher general population anxiety scores during the pandemic. 15
Nonetheless, significant improvements in both PHQ-9 and GAD-7 scores were demonstrated during both the pre-COVID-19 and COVID-19 time periods, and neither mean change PHQ-9 and GAD-7 scores, weeks of enrollment, nor mean assessments completed were significantly different between time periods. Number of assessments completed did predict improvement, suggesting the importance of length of participation, regardless of modality.
PHQ-9 scores in both time periods decreased from moderately severe to moderate, 12 though PHQ-9 categorical improvement was statistically more common in the pre-COVID-19 period. This could suggest some limitations of telehealth IOP. Spontaneous interactions between group members and behavioral activation implicit to highly routinized in-person treatment may be compromised by telehealth.
In contrast, although GAD-7 scores remained in the moderate category during both time periods, 11 patients with anxiety disorders had significantly higher mean and categorical GAD-7 improvements in the COVID-19 time period. This may suggest that telehealth IOP is particularly efficacious for anxiety disorders; though long-term avoidance of stressors may prove countertherapeutic, telehealth minimizes the anxiety-provoking commutes and interactions with strangers associated with office-based visits.
IOP demographics were representative of the region's population. There were no significant differences in racial/ethnic distributions between the two time periods, consistent with previously reported findings from New Haven, 5 nor were there significant differences in gender distribution. Although female patients had statistically significantly higher GAD-7 scores at IOP entry in the COVID-19 period when compared with male patients, no further racial/ethnic or gender associations with clinical outcomes were observed. It has been reported that female patients positive for COVID-19 may experience higher GAD-7 and PHQ-9 scores than COVID-19-positive men. 16 Rates of COVID-19 were not collected in our sample, so this effect cannot be ruled out.
Although poverty impacts patient access to the hardware, software, and internet connectivity necessary for telehealth, no significant differences were found in engagement related to zip code poverty association. Consistent with one previous report, no differences were found in IOP attendance between commercial and public insured groups during the COVID-19 time period. 5 However, publicly insured individuals had significantly fewer weeks enrolled than commercially insured individuals during the pre-COVID-19 time period. Informally, IOP patients with public insurance commonly report transportation and childcare stressors, which impact office-based attendance. Telehealth IOP may mitigate these stressors and so facilitates longer enrollment.
Individuals with commercial insurance demonstrated significantly greater improvements in PHQ-9 and GAD-7 scores; when the COVID-19 and pre-COVID-19 periods were analyzed separately, these improvements remained only in the COVID-19 time period. This suggests that publicly insured individuals did not experience improvements in anxiety or depression equal to that of the commercially insured group, despite equal enrollment length. An important limitation is that in the publicly insured group, the mean number of GAD-7 and PHQ-9 assessments completed during the COVID-19 time period was significantly less than for the commercially insured group, even though the groups had similar number of weeks attended.
During office-based IOP, therapists facilitated assessment completion during groups. However, during the COVID-19 period, electronic assessments were completed by patients outside of groups. Lack of live therapist prompting and encouragement may have contributed to overall (but nonsignificant) decreases in GAD-7 and PHQ-9 completion; among the publicly insured, this may have been compounded by competing priorities to timely form completion. Although it is possible that “missing” GAD-7 and PHQ-9 scores in the public insured group influence our findings, the importance of patient buy-in and clinician support to enhance full clinical participation is further emphasized.
Our study does have a few other limitations. Although adults >30 years old were more represented in the COVID-19 period than in the pre-COVID-19 period, few (n = 6) patients >65 years enrolled in these IOP groups did so pre-COVID-19. Although this number is too small to suggest that telehealth adoption was a barrier for older adult participation, further study is suggested. 17 In addition, as none of the IOP-enrolled patients carried primary diagnoses of dementia, schizophrenia spectrum disorders, or intellectual disability, effects of cognitive impairment were unexplored, although some patients with schizophrenia do benefit from telehealth groups. 18
Nonetheless, caution should be used in interpreting broader applicability of these findings to these diagnostic groups as well as to populations with lower rates of technological literacy. Finally, ongoing pandemic stressors, or sequelae of COVID-19 infection itself, could be driving treatment effects, potentially confounding generalizability beyond the pandemic.
Conclusions
During the COVID-19 pandemic, adult patients in a multitrack transdiagnostic telehealth adult IOP had statistically equivalent participation rates and clinical outcomes, as measured by PHQ-9 and GAD-7 assessment scores, to IOP patients attending office-based services before the pandemic. In both the COVID-19 and pre-COVID-19 time periods, number of assessments completed highly correlated with clinical improvement, highlighting the importance of participation over time.
Although improvements were similar for patients regardless of sociodemographic and clinic characteristics, individuals with commercial insurance sustained significantly greater mean improvements in assessment scores than those with public insurance. These findings may be limited by a participation effect in the publicly insured group. In addition, individuals with anxiety disorders had significant improvement in the COVID-19 period, suggesting effectiveness of IOP telehealth in this population. Given these findings, but considering several important limitations, more study is needed to further define outcome optimization beyond the COVID-19 pandemic.
Footnotes
Acknowledgments
The authors express their thanks to Ms. Joan Spinogatti for her assistance in article preparation for journal submission. We also thank Ms. Travea Ghee and Ms. Elizabeth Janco for providing information on clinical operations that strengthened data collection and interpretation. We extend our gratitude to Dr. Jatinder Babbar and all the physicians, advanced practice providers, therapists, nurses, and staff devoted to providing excellent patient care in IOP. Finally, we thank our patients for trusting their care to us.
Authors' Contributions
J.M.G. carried out conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing, visualization, and project administration. J.S.B. carried out formal analysis, investigation, data curation, writing—original draft, and writing—review and editing. S.Z. was involved in investigation, resources, data curation, and writing—review and editing. T.P. was involved in conceptualization, investigation, methodology, resources, writing—review and editing, and supervision. K.O'T. carried out conceptualization, methodology, investigation, resources, writing—review and editing, and supervision. K.N.R.C. was involved in conceptualization, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.