
Abstract
Introduction:
Telemedicine is the practice of caring for patients remotely when the patient and provider are not physically present at the same location. Within orthopedic surgery, telemedicine offers care without the typical obstacles of an in-person appointment such as difficulty ambulating following surgery and patient wait times. In this study, we evaluated patient interest and satisfaction in postoperative telemedicine visits following hip or knee arthroplasty surgery.
Materials and Methods:
Patients were offered either a traditional in-person or a remote telemedicine postoperative visit following surgery. Patients were asked to complete a satisfaction survey following their postoperative visit regarding their experience. Patient-survey responses as well as patient-reported outcome metrics were captured using a mobile and web-based electronic patient rehabilitation application.
Results:
A total of 766 patients were included in this study with 360 offered postoperative telemedicine visits and 402 offered traditional in-person visits. Two hundred fifty-nine patients reported satisfaction levels with their telemedicine visit, with 58.3% of patients characterizing their feelings with the visit as “extremely satisfied,” 32.0% as “satisfied,” 8.9% as “neutral,” 0.3% as “dissatisfied,” and 0.3% as “extremely dissatisfied.” A total of 713 patients reported how the COVID-19 pandemic effected their feelings toward telemedicine with 12.9% of patients characterizing the affect as “extremely positively,” 33.1% of patients as “positively,” 48.9% of patients as “neutral,” 3.6% of patients as “negatively,” and 1.4% of patients as “extremely negatively.” There were no significant differences in the change between preoperative Hip disability and Osteoarthritis Outcome Scores/Knee Injury and Osteoarthritis Outcome Score Joint Replacement, or Veterans RAND 12 Physical and Mental components and these values at 12 weeks follow-up and 1-year follow-up, respectively, in patients who had telemedicine visits versus those who had traditional in-person visits.
Discussion:
The results of this study demonstrate that the patients who decided to have a telemedicine visit during their postoperative visit were satisfied with their experience. Overall, COVID-19 had a positive influence on patient's feelings toward telemedicine visits.
Introduction
The demand for total joint arthroplasty (TJA) is projected to rise annually owing to an aging population in the United States. 1,2 TJA are highly successful procedures that often do not require an in-person assessment for postoperative evaluation. 3 –5 Consequently, a possible alternative to postoperative in-person visits is telemedicine, or the practice of caring for patients remotely when the patient and provider are not physically present at the same location. 6
Telemedicine offers care following TJA without the typical obstacles of an in-person appointment such as, difficulty ambulating following surgery, commuting to provider location, patient wait times, and cost. 7 –10 More recently, the use of telemedicine has provided patients an opportunity to avoid in-person visits and the associated risks of exposure to COVID-19. 11,12 As a result, telemedicine has expanded considerably in the orthopedic clinical setting and has been shown to be effective for postoperative visits. 11 –13
Despite the integration of telemedicine for postoperative medical appointments, there is a lack of orthopedic literature assessing patient sentiment toward telemedicine visits following TJA. The purpose of this study was to assess the functionality and success of remote postoperative visits through evaluating patient interest and satisfaction with postoperative telemedicine appointments following TJA.
Materials and Methods
Initially we included all patients (n = 792) who underwent primary elective hip or knee arthroplasty surgery performed by 13 arthroplasty surgeons at our institution, a tertiary academic orthopedic hospital, between January and December 2020. The only patients excluded from this study were those who chose not to complete their survey following their postoperative follow-up visit or those filled out the form incorrectly.
Following their surgery, patients were offered either a traditional in-person postoperative visit or a remote telemedicine postoperative visit as part of routine care (Fig. 1). The offer of a telemedicine visit versus in-person visit was determined by the surgeon and patients were not randomized into either group.
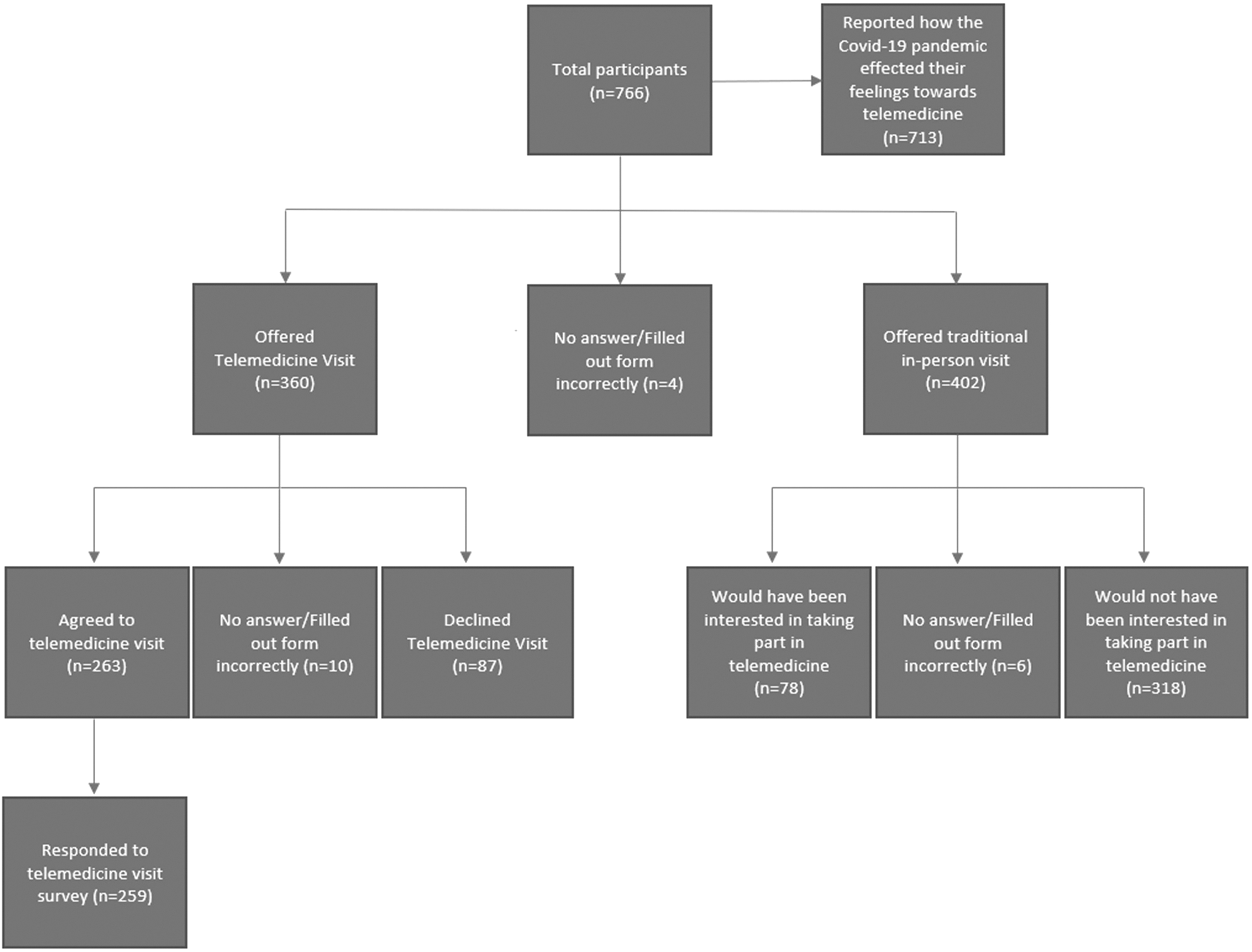
Branching logic flow chart for postoperative follow-up electronic survey. This flow chart demonstrates the different cohorts of patients in the study who were stratified by the offer of a telemedicine visit and the branching logic questions in the electronic survey.
Patients who agreed to participate in the remote telemedicine postoperative visits were asked to complete a satisfaction survey following their postoperative visit regarding their telemedicine experience. The satisfaction survey included five possible response options to assess their postoperative visit: “extremely satisfied,” “satisfied,” “neutral,” “dissatisfied,” and “extremely dissatisfied.” Satisfaction survey results were only collected for patients who had a telemedicine visit, patients who had in-person visits were not asked about their satisfaction levels with their visit. Patients who were offered a telemedicine visit but elected to defer participation were asked to provide a reason.
All patients offered either traditional in-person postoperative visits or remote telemedicine postoperative visits were surveyed assessing their feelings toward telemedicine owing to COVID-19. The survey included five possible response options to assess their postoperative visit: “extremely positively,” “positively,” “neutral,” “negatively,” and “extremely negatively.”
Patient-survey responses and patient-reported outcome metric (PROM) scores, which included Hip disability and Osteoarthritis Outcome Scores for Joint Replacement (HOOS, JR), Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS, JR), and Veterans RAND 12 Physical and Mental components (VR-12 PCS/MCS respectively), were captured using a mobile and web-based electronic patient rehabilitation application (Force Therapeutics, New York, NY). All patient responses were included in the analysis except for patients who mistakenly sent in multiple surveys, in which case the extra surveys were deleted and not considered in the analysis (n = 26).
STATISTICAL ANALYSIS
Statistical analysis was carried out in Microsoft Excel (Microsoft Corp., Redmond, WA) and all p-values were calculated using a two-tailed type-2 t-test and values were considered significant at p < 0.05.
Results
A total of 766 patients were included in this analysis, with 360 (47.0%) offered postoperative telemedicine visits and 402 (52.5%) patients offered traditional in-person postoperative visits (Table 1). The decision to offer patients a telemedicine visit versus an in-person visit was solely at the discretion of the surgeon and a part of their routine care, it was not the result of any randomization. Of the patients not offered telemedicine visits, 78 (19.4%) would have been interested in doing their first postoperative follow-up visit over the computer or smart phone and 318 (79.1%) would have preferred a traditional in-person visit. Of the patients who were offered to use telemedicine, 263 patients (73.1%) agreed to the virtual consultation and 87 patients (24.2%) declined and chose a traditional in-person visit (Table 2).
Demographic Data and Surgical Characteristics by Randomization Group (N = 766)
Demographic data for patients in the traditional in-person cohort and the cohort that was offered a telemedicine visit.
Demographic Data and Surgical Characteristics by Telemedicine Participation (n = 360)
Demographic data for the cohort of patients that agreed to the telemedicine visit versus those who were offered the visit but declined.
Of the patients who declined using telemedicine, 9 patients (10.2%) said it was owing to not having the technology to download the necessary software, 17 patients (19.3%) said that they were not comfortable or confident enough with the technology, and 62 patients (70.4%) responded “other” with the option to give a specific explanation.
Of the 62 patients who answered “other,” 21 (33.9%) said they “Preferred seeing their doctor in person,” 10 (16.1%) “Believed in person physical examination was more reliable,” 7 (11.3%) “Needed an X-Ray,” 3 (4.8%) said “It was easy/convenient for them to travel for the in person visit,” 3 (4.8%) “Had no preference for telehealth vs. in person visits,” 1 (1.6%) said their “Doctor instructed them to have an in person visit,” 1 (1.6%) said they “Were unsure how to use technology,” 1 (1.6%) said they “Felt they did not need follow-up as they were healing well,” 6 (9.7%) gave unclear responses and 9 (14.5%) gave no response (Table 3). Of the patients who had a telemedicine visit, 250 patients (95.1%) felt that they had their questions answered appropriately and 11 patients (4.2%) did not.
Reasons Given for Not Taking Part in Telemedicine (n = 62)
Reasons patients gave for not accepting the offer of a telemedicine visit.
A total of 259 patients (71.0%) reported satisfaction levels with their telemedicine visit, with 58.3% of patients characterizing their feelings with the visit as “extremely satisfied,” 32.0% of patients as “satisfied,” 8.9% of patients as “neutral,” 0.3% of patients as “dissatisfied,” and 0.3% of patients as “extremely dissatisfied” (Fig. 2).

Patient satisfaction with telemedicine visits. This bar graph shows patient responses to the survey question “How would you rate your experience with your telemedicine visit?”
Seven hundred thirteen patients reported how the COVID-19 pandemic effected their feelings toward telemedicine with 12.9% of patients characterizing the visit as “extremely positively,” 33.1% of patients as “positively,” 48.9% of patients as “neutral,” 3.6% of patients as “negatively,” and 1.4% of patients as “extremely negatively” (Fig. 3). Five hundred eighty-two patients (76.0%) reported at least one PROM score of either HOOS/KOOS, JR, or VR-12 PCS/MCS preoperatively as well as at 12-week follow-up and 1-year follow-up.
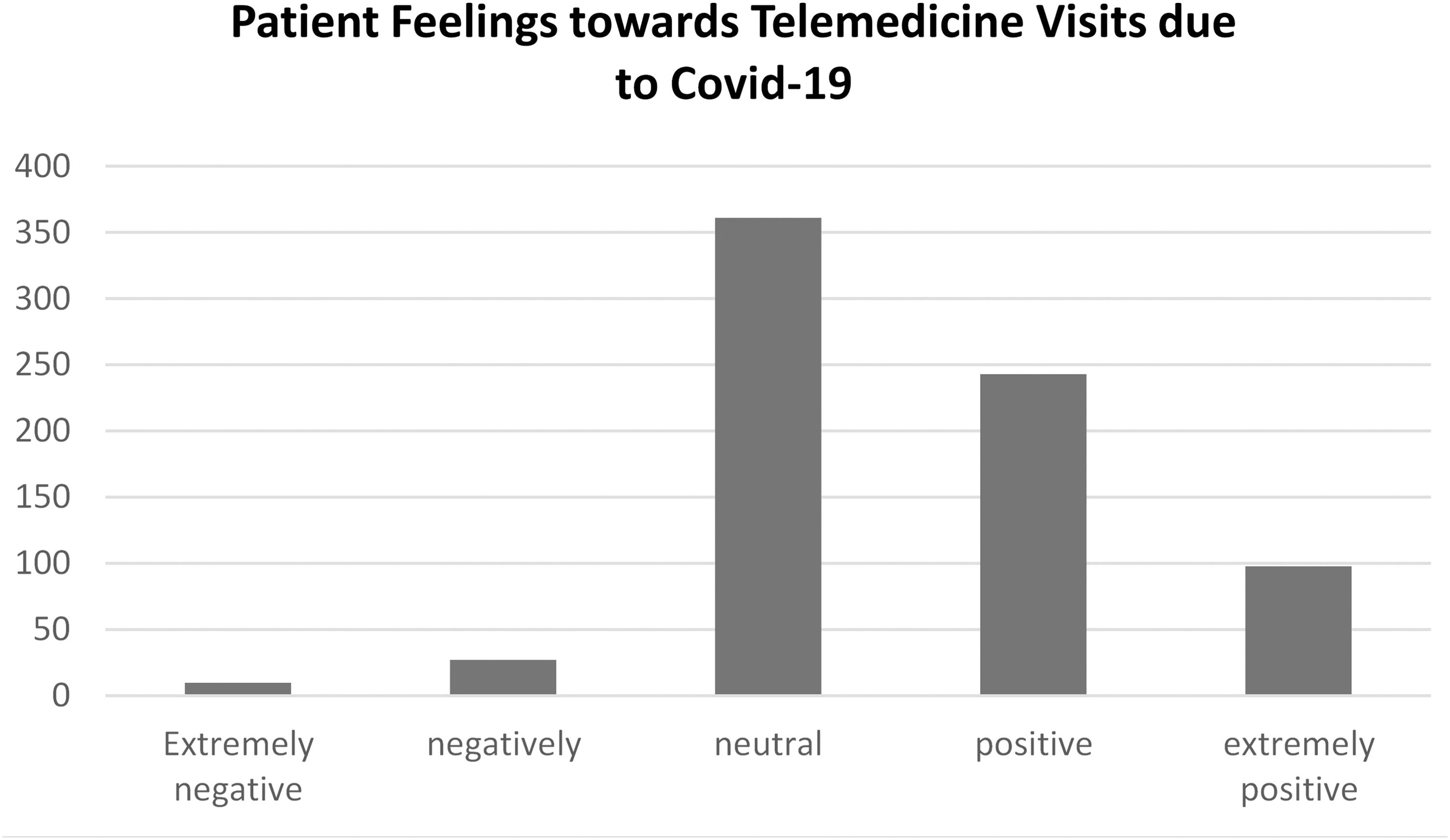
Patient feelings toward telemedicine visits owing to COVID-19. This bar graph shows patient responses to the survey question “How has Covid-19 impacted your perception of telemedicine?”
There was no significant difference in the average change in preoperative HOOS, JR at 12 weeks between the telemedicine group (26.25 ± 15.23 [n = 152]) and the traditional in-person group (25.80 ± 18.31 [n = 243]) (p = 0.80). Similarly, there was no significant difference in the average change in preoperative HOOS, JR at 1 yr between the telemedicine group (34.74 ± 16.18 [n = 109]) and the traditional in-person group (31.30 ± 18.65 [n = 175]) (p = 0.10). Like the HOOS, JR scores there was no significant difference in the average change in preoperative VR-12 PCS at 12 weeks between the telemedicine group (12.93 ± 10.70 [n = 158]) and the traditional in-person group undergoing hip arthroplasty (12.08 ± 11.29 [n = 241]) (p = 0.45).
Likewise, there was no significant difference in the delta between preoperative VR-12 PCS at 12 weeks and at 1-year between the telemedicine group (16.17 − 10.90 [n = 112]) and the traditional in-person group undergoing hip arthroplasty (14.87 − 11.05 [n = 176]) (p = 0.33). The average delta between preoperative VR-12 MCS at 12 weeks between the telemedicine group (1.77 ± 10.21 [n = 158]) and the traditional in-person group undergoing hip arthroplasty (3.80 ± 10.86 [n = 241]) also did not have a significant difference (p = 0.06). Finally, there was no significant difference in the average change in preoperative VR-12 MCS at 1 year between the telemedicine group (2.68 ± 9.90 [n = 112]) and the traditional in-person group undergoing hip arthroplasty (3.90 ± 11.14 [n = 176]) (p = 0.33) (Table 4).
Change in Average Preoperative HOOS, JR and VR-12 PCS/MCS Versus 12-Weeks and 1-Year Follow-Up After Hip Arthroplasty
Average change in patient-reported outcome metrics between preoperative values and values at either 12 weeks postop or 1-year postop for hip arthroplasty patients in the telemedicine cohort versus those with traditional in-person visits.
HOOS, Hip disability and Osteoarthritis Outcome Scores; JR, Joint Replacement; VR-12 PCS/MCS, Veterans RAND 12 Physical and Mental components.
There was no significant difference in the average delta in preoperative KOOS, JR at 12 weeks between the telemedicine group (8.89 ± 10.82 [n = 65]) and the traditional in-person group (5.63 ± 14.82 [n = 122]) (p = 0.09). In addition, there was no significant difference in the average change in preoperative KOOS, JR at 1 year between the telemedicine group (18.09 ± 17.52 [n = 43]) and the traditional in-person group (19.76 ± 18.44 [n = 98]) (p = 0.61). The difference in average change in preoperative VR-12 PCS at 12 weeks between the telemedicine group (6.18 ± 9.61 [n = 69]) and the traditional in-person group undergoing knee arthroplasty (7.51 ± 9.22 [n = 155]) was not significant (p = 0.34).
The difference in average delta in preoperative VR-12 PCS at 1-year between the telemedicine group (10.31 ± 10.80 [n = 56]) and the traditional in-person group undergoing knee arthroplasty (11.83 ± 10.38 [n = 102]) was also not significant (p = 0.40). There was no significant difference in the average change in preoperative VR-12 MCS at 12 weeks between the telemedicine group (−0.22 ± 11.25 [n = 69]) and the traditional in-person group undergoing knee arthroplasty (0.77 ± 10.60 [n = 155]) (p = 0.54). Finally, there was no significant difference in the average delta in preoperative VR-12 MCS at 1 year between the telemedicine group (1.26 ± 10.54 [n = 56]) and the traditional in-person group undergoing knee arthroplasty (0.65 ± 10.31 [n = 102]) (p = 0.73) (Table 5).
Change in Average Preoperative KOOS, JR and VR-12 PCS/MCS Versus 12-Weeks and 1-Year Follow-Up After Knee Arthroplasty
Average change in patient-reported outcome metrics between preoperative values and values at either 12 weeks postop or 1-year postop for knee arthroplasty patients in the telemedicine cohort versus those with traditional in-person visits.
KOOS, Knee Injury and Osteoarthritis Outcome Score.
Discussion
The use of telemedicine among orthopedic surgeons has increased dramatically since the beginning of the COVID-19 pandemic. 11,14 A study performed by Hurley et al. found telemedicine use in orthopedic surgery increased from 20.5% before the pandemic to 84.8% afterward. 11 Although the transition to telemedicine during the pandemic was primarily in response to reducing risk of exposure to COVID-19, there are other notable benefits to telemedicine for both patient and provider, such as patient costs, wait time, and reduced travel. 15,16 This study aimed to better understand patients' attitudes and acceptance of telemedicine visits after total hip and knee replacement surgery now that a greater proportion of patients are using telemedicine as standard of care for follow-up visits for TJA.
In this study, 90.3% of patients who decided to have a telemedicine postoperative visit were satisfied or extremely satisfied with their experience. We also found that 46.0% of patients characterized their feelings about telemedicine as either positive or extremely positive because of COVID-19. Of the 767 patients in this study 259 were offered a telemedicine visit, agreed to take part in the telemedicine visit, and completed a survey to describe their satisfaction levels with telemedicine. This report evaluated these 259 patient's satisfaction levels with their telemedicine visit and is, to our knowledge, the largest assessment of patient satisfaction with telemedicine visits after hip and knee replacement surgery.
Previous research assessing patient satisfaction with remote follow-up visits for TJA was mostly positive. El Ashmawy et al. have evaluated satisfaction levels of 56 patients with telemedicine visits following total hip and knee replacement surgery and found that 89.92% of patients were either “satisfied” or “very satisfied” with their postoperative visit. 13 Marsh et al. assessed patient satisfaction following a web-based follow-up assessment versus in-person follow-up appointments. 17 Enrolled patients completed quality-of-life and function questionnaires remotely and underwent postoperative radiographs near their home.
The percentage of web-based patients (76.5%) who were either extremely or very satisfied with their follow-up visit was significantly lower than those patients who had in-person follow-up visits (82.0%; p < 0.01). 17 In the study, surgeons would not meet with their patient remotely if the patients were experiencing noticeable medical problems or if there were important imaging findings warranting clinical intervention. These patients were also scheduled to see their surgeon in-person at the 1-year follow-up. 17 This protocol is different from our study, where remote patient follow-ups were consistently performed with videoconferencing rather than a web-based follow-up assessment and may contributed to the higher overall satisfaction levels (90.3%) as a result.
A separate study performed by Sharareh and Schwarzkopf reviewed 34 patients who underwent telemedicine and in-person follow-up visits versus 44 patients who had only in-person follow-up visits. The authors found patient satisfaction for postoperative care augmented by telemedicine (9.88 ± 0.34) was significantly higher than patient satisfaction in the in-person-only group (8.1 ± 1.1; p < 0.05). 18
Our study also assessed patient sentiment of telemedicine during the COVID-19 pandemic. Patients had mostly positive feelings toward telemedicine owing to COVID-19, with 46.0% patients expressing positive or extremely positive feelings toward telemedicine, 48.9% of patients feeling neutral, and 5.0% of patients expressing negative or extremely negative feelings toward telemedicine. Other orthopedic literature has found patients more willing to use telemedicine as a result of the COVID-19 pandemic. Buchalter et al. surveyed 382 patients regarding patient satisfaction of telehealth visits for orthopedic procedures during COVID-19. 19 Overall, patients were satisfied with their telemedicine visits (4.25/5.00 ± 0.96).
Furthermore, 37.0% of patients would prefer future visits to be conducted using telehealth and 93.9% of patients would continue to use telehealth after the COVID-19 pandemic. 19 Similarly, Kirby et al. found 88.8% of sports medicine patients to be “satisfied” or “very satisfied” with telemedicine visits during COVID-19, with 42% of patients preferring future telehealth visits over in-person visits outside the pandemic. 12 A study by Sabbagh et al. compared in-person follow-ups for shoulder surgery before the Covid-19 pandemic versus telemedicine follow-ups during the pandemic. Of interest, although patients reported no significant differences in patient satisfaction and patient-reported outcome measures between in-person and telemedicine follow-ups (p = 0.289), 83.33% of the telemedicine group preferred traditional in-person visits over telemedicine visits. 20
In addition, our study also analyzed the difference in patient's preoperative HOOS/KOOS, JR and VR-12 PCS/MCS and these respective values at 12-week follow-up and 1-year follow-up. We found no significant difference in any of these PROM scores between the patients who had telemedicine visits and those who had traditional in-person visits at either 12-week follow-up or 1-year follow-up ( Tables 4 and 5 ). This result confirmed our hypothesis as we expected any differences in patient's sentiments between these groups following surgery to be more of a function of their comfort with technology than having to do with the success of their hip or knee arthroplasty.
There were a number of limitations of our study. Patients were not randomized to participate in telemedicine or in-person postoperative visits; it was solely at the discretion of the individual surgeon to decide whether to offer the telemedicine visit. This could lead to selection bias when enrolling patients, for example, the surgeon may have not offered a telemedicine visit to patients who seemed like they were not recovering well.
In addition, in-person postoperative satisfaction was not assessed. As a result, there is no comparison for in-person versus telemedicine patient satisfaction. Also, the satisfaction survey for postoperative telemedicine visits has not been formally validated. Another limitation of the study was the small number of response options for reasons why patients chose to forgo postoperative telemedicine visits, thus analysis regarding this topic was limited. Finally, an additional limitation of the study was that we only had PROM scores for 582 (76%) of the 766 members of the study population.
As a result of significant integration of telemedicine in outpatient management, which increased significantly in response to the COVID-19 pandemic, orthopedic visits traditionally done in person are now often performed using telemedicine. This study demonstrated that patients who elected to participate in telemedicine visits after total joint replacement were generally satisfied or very satisfied with their postoperative telemedicine visits.
However, although, patients with postoperative telemedicine visits during the COVID-19 pandemic had mostly positive feelings toward telemedicine, a significant portion of patients remain reluctant to use this technology for their postoperative care. Future research is needed to determine the reasons patients are dissatisfied with telemedicine care after total joint replacement, and to determine how to optimize the experience and increase participation when appropriate in the future.
Footnotes
Acknowledgments
Members of the Force Writing committee: Craig Capeci, Roy Davidovitch, Matthew Hepinstall, Justin Lamont, William Macaulay, Ivan Madrid-Fernandez, Morteza Meftah, Scott Marwin, Joshua Rozell, Ran Schwarzkopf, Jim Slover, Joseph Zuckerman, and Daniel Waren.
Ethical Approval
This study was exempt from human-subjects review by our institutional review board (IRB).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
Consent to publish was obtained from all individual participants included in the study.
Disclosure Statement
M.R.M. and M.S.G. have nothing to disclose. R.S. is a paid consultant for Smith & Nephew, and Intellijoint. He also has stock options in Gauss Surgical and PSI outside the submitted work. J.D.S. is a paid speaker for Pacira and paid consultant for Horizon Pharma.
Funding Information
No funding was received for this article.