
Abstract
Introduction:
Telemedicine is an effective means of delivering health care in Southeast Asian (SEA) countries. This systematic review explored the use of telemedicine systems for delivering health care services in SEA countries during the past 10 years.
Methods:
Literature searches were conducted in PubMed, Embase, Medline, Global Health, and CENTRAL (Cochrane Central Register of Controlled Trials). The inclusion criteria were as follows: (1) studies published between 2010 and 2021; (2) study settings located in SEA countries; (3) articles published in English; and (4) availability of a full-text version of the article. Information was extracted and evaluated for each study based on quality and risk of bias.
Results:
Thirty-seven of 6,554 records were eligible for inclusion. Studies included based on percentage were descriptive (29.73%), cost-effective (8.11%), randomized controlled trials (5.41%), and mixed methods (2.7%). Teleophthalmology and teleconsultation were the major reasons for using telemedicine, representing 21.62% of all studies. A hub-and-spoke and store-and-forward models were used. Free messenger applications supported communication modalities in or out of the systems.
Discussion:
The COVID-19 (coronavirus disease 2019) pandemic increased research studies on telemedicine, with most studies occurring in Singaporean hospitals (49%). Descriptive studies predominated, followed by retrospective and cross-sectional studies.
Conclusions:
Our findings demonstrated that telemedicine was a powerful tool. It is feasible, safe, effective, and less expensive than traditional methods. However, robust research is needed to fully investigate telemedicine systems in SEA countries.
Introduction
Telemedicine is often defined as the delivery of health care service at a distance using information and communication technology (ICT) by clinicians and health care professionals for diagnosis, treatment, prevention of disease or injuries, research, education, evaluation, and the exchange of valid information. 1 Technologies used in telemedicine are diverse in nature and complexity. 2 The Center for Connected Health Policy (CCHP) categorized telemedicine into four types: live video, store and forward, remote patient monitoring, and email/phone/fax. 3
Telemedicine is a useful tool that provides an efficient and cost-effective way to deliver health care. 4 It has been used for more than 100 years to help health care workers deliver services. In 1906, Willem Einthoven, a Dutch physiologist who developed a technique similar to telemedicine, created the first mobile electrocardiograph device to record the electrical cardiac signals of patients from a hospital 1.5 km away from his laboratory. 5 The main benefits of telemedicine are reduced travel costs and time saved, especially for people who live in rural areas with limited access to health care services. 6 Telemedicine provides good opportunities for emerging and developing countries to access basic primary health care services. Health care providers are able to evaluate, diagnose, treat, and provide follow-up care to distant patients by using telemedicine applications. 7,8
Telemedicine effectively delivers last mile health care in Southeast Asian (SEA) countries. ACCESS Health International Southeast Asia recently reported that digital technology is the key to achieving universal health coverage in the Association of Southeast Asian Nations (ASEAN). 9 In Thailand, an initiative, which included the Ministry of Public Health and the National Broadcasting and Telecommunications Commission, used telemedicine to increase health care access for remote areas via telemedicine systems. 10,11
In 2012, the national Expanded Program on Immunization in Vietnam developed and piloted a digital immunization registry program known as ImmReg, a web-based application system to register new clients, to track due dates, and to identify doses required for on-time vaccination. The system automatically sends short message service (SMS) reminders to clients and generates reports to health care workers. 12
In the past decade, many ASEAN countries implemented telemedicine services, but there were no national scientific institutions whose focus was to develop telemedicine on a broad scale. Rather, most efforts were short-term demonstration projects, carried out in conjunction with international companies and large hospitals or universities. 13 Furthermore, there was little published evidence 14 to document the existence of the programs or to evaluate the quality, accessibility, effectiveness, and cost of the telemedicine care provided. 15 Telehealth was not integrated into existing health care service systems because of the financial and technological barriers. In addition, physicians' lack of expertise with the technology also served as impediments to the implementation of telemedicine programs. 13,15,16
During the coronavirus disease 2019 (COVID-19) pandemic, policy changes reduced restrictions on telemedicine, thus enabling health care entities to provide services when face-to-face care was neither safe nor practical. 17,18 Health care providers and systems promptly adopted and expanded telemedicine services to provide a safe online service in place of in-person visits. 19 Unfortunately, telemedicine has some limitations, for instance, it limits the ability of the health care professional to thoroughly observe the patient. The lack of in person contact may negatively impact the guidance provided to the patient and the clinical decisions made by the health care professional. The objective of this systematic review was to explore the implementation and use of telemedicine systems for delivering health care services in SEA countries during the past 10 years.
Methods
A systematic review of the literature was conducted to elucidate the current use and implementation of clinical care provided via telemedicine in SEA countries. 1
TYPE OF STUDY
The systematic review included: descriptive, observational, analytical, quasi-experimental, clinical trial, and randomized controlled trial studies. Studies that reported on patient outcomes, evaluation methods, or educational outcomes were also included in the review. Surveys or interviews of experts' opinion or experience were excluded.
INFORMATION SOURCES
Literature searches were conducted in PubMed, Embase, Medline, Global Health, and Cochrane Central Register of Controlled Trials (CENTRAL) up to April 25, 2021. Selected reference lists from related articles were also screened to identify additional appropriate studies. Medical subject headings (MeSH) and keywords were used to search PubMed, Embase, and Medline. Relevant articles were retrieved and imported to a reference manager software program, and duplicates were deleted.
SEARCH STRATEGY
Telemedicine and Southeast Asia were the main MeSH terms used to identify relevant studies. In addition to MeSH headings, names and synonyms were used to retrieve the greatest number of articles related to telemedicine in all SEA countries. The search terms used in each electronic database are presented in Table 1.
Literature Searches and Strategies
CENTRAL, Cochrane Central Register of Controlled Trials.
STUDY INCLUSION AND EXCLUSION CRITERIA
The inclusion criteria were as follows: (1) studies published between 2010 and 2021; (2) study settings located in SEA countries, including Brunei, Burma (Myanmar), Cambodia, Timor-Leste, Indonesia, Laos, Malaysia, the Philippines, Singapore, Thailand, and Vietnam. The MeSH heading Australia was used to retrieve additional articles since the country provides support to SEA nations in the health informatics domain; (3) articles published in English; and (4) a full-text version of the article was available. The exclusion criteria were e-health or m-health interventions, survey, and review articles. Endnote was used to retrieve and save research records and articles. 20
STUDY SELECTION
Relevant records were retrieved and imported to a reference manager software program, and duplicates were deleted. All records were screened and evaluated for compliance with the inclusion and exclusion criteria. Full-text versions of the eligible records were retrieved and read.
DATA EXTRACTION
A data extraction form to record the general characteristics, use, and implementation of included studies was adaptively created based on the guideline for developing a data extraction from the Cochrane Handbook for Systematic Reviews of Interventions. 21 For each included study, the following information was recorded: last name of the first author, year of publication, study design, sample size, duration of study, location and country of study, type of telemedicine, participant and disorder, organizational setting, system and technology used, implementation, and main finding of study. A.P. extracted the data from included studies, and then, D.G.S. checked and evaluated the extracted data.
QUALITY OF STUDIES
Each eligible study was evaluated for quality and risk of bias based on the Statement on reporting of evaluation of studies in Health Informatics (STARE-HI). 22 Study design, theoretical background, participant, study flow, outcome measures or evaluation criteria, methods for data acquisition and measurement, and methods for data analysis were all included. The Cochrane Assessment Risk of Bias tool was used to analyze and present the risk of bias graphs. 23
STATISTICAL ANALYSIS
Descriptive statistics were performed for general characteristics of included studies, including frequency and percentage. All information regarding telemedicine is presented.
Results
The literature search identified 6,554 records. After 2,417 duplicates were removed, the titles and abstracts of the unique 4,137 records were screened by applying the inclusion and exclusion criteria for removing extraneous titles. All remaining records were downloaded in full-text format, and the articles were screened again based on the inclusion and exclusion criteria. Thirty-seven eligible studies were included in the review (Fig. 1).
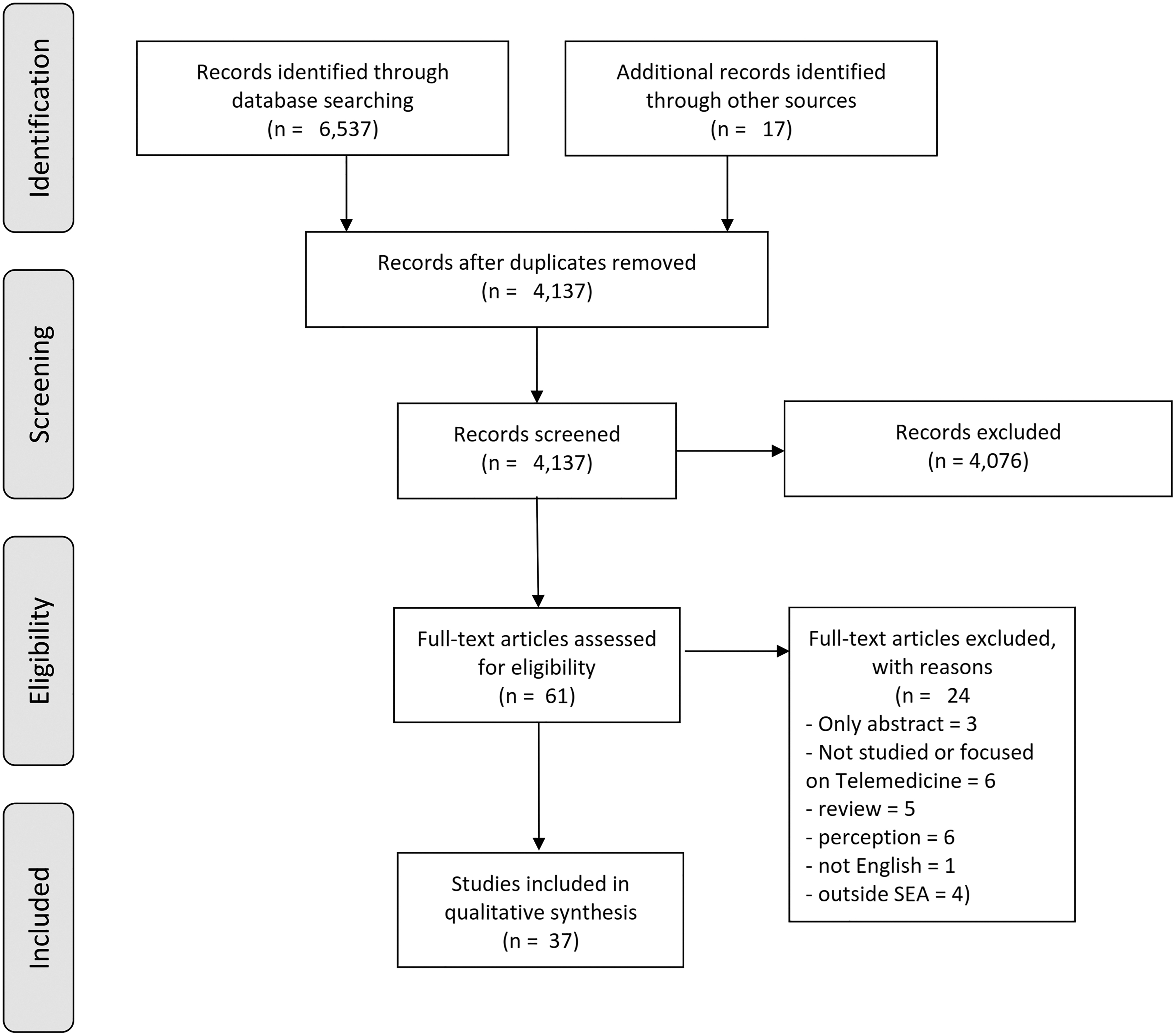
Study flow diagram.
Singapore (48.65%) was the most frequently recorded study setting, followed by Thailand (21.62%) and Malaysia (10.81%). Various study designs were used to investigate telemedicine services, including descriptive studies (29.73%), cost-effective studies (8.11%), randomized controlled trials (5.41%), and mixed methods studies (2.7%). Teleophthalmology and teleconsultation were the major reasons for using telemedicine, representing 21.62% of all studies (Table 2). Most of the included studies were published in 2020 (32.48%), followed by 2015 (10.80%) and 2013 (10.79%) (Fig. 2).
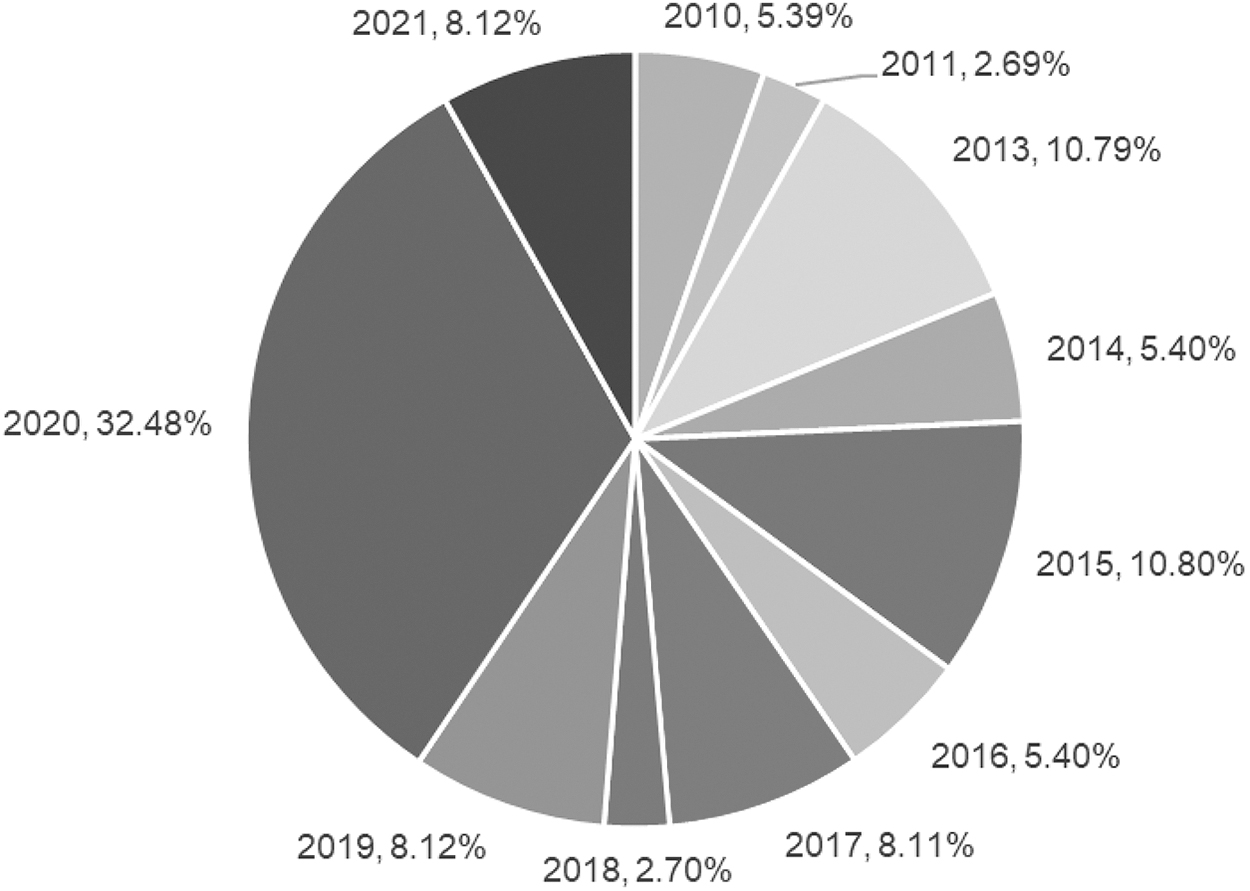
Publication years of included studies.
Characteristics of Included Studies
IMPLEMENTATION AND USE OF TELEMEDICINE
All included studies established that telemedicine was used in several organizational settings, and different types of telemedicine were used for different clinical conditions. We summarized the details of each study (Table 3).
Implementation and Use of Telemedicine of Included Studies
AES, Advanced Encryption Standard; ALS, advanced life support; APN, advanced practice nurse; CGH, Changi General Hospital; CI, confidence interval; CIED, cardiac implantable electronic devices; CMV, cytomegalovirus; COVID-19, coronavirus disease 2019; CPOE, computerized physician order entry; CSC, Children's Surgical Centre; CT, computed tomography; DFP, digital fundus photograph; DTD, door to decision; DTN, door to needle; ECG, electrocardiogram; ED, emergency department; ESA, extended screening area; GSM, Global System for a Mobile communications; HbA1c, hemoglobin A1C; HD, hemodialysis; INR, international normalized ratio; iPATH, Internet Pathology Suite; KCMH, King Chulalongkorn Memorial Hospital; KTPH, Khoo Teck Puat Hospital; LED, light-emitting diode; MMS, multimedia messaging system; MRI, magnetic resonance imaging; N/A, insufficient data or no information; NIHSS, National Institute of Health Stroke Scale; NM, nuclear medicine; NNI, National Neuroscience Institute; NSU, neurosurgical unit; OMFR, oral and maxillofacial radiology; PACS, picture archiving and communication system; PPE, personal protective equipment; PR, panoramic radiography; PSAs, Patient Service Associates; ROP, retinopathy of prematurity; rt-PA, recombinant tissue-plasminogen activator; SiDRP, Singapore Integrated Diabetic Retinopathy Programmed; SMS, short message service; TCF, telegeriatric consultation form; Tele-SOC, Telemedicine Specialist Outpatient Clinic; THB, Thai Baht; TMJ, temporomandibular joint; TTSH, Tan Tock Hospital; UCC, urgent care center; UHS, University of Health Sciences; VBCI, video-based contact intervention.
TELEMEDICINE MODEL
A hub-and-spoke system was one of the models applied to developing and using telemedicine systems. Ang et al. used the hub-and-spoke model for telestroke in Singapore. An acute stroke patient at the emergency department (ED) of a study hospital (spoke) was examined by the duty neurologist at the National Neuroscience Institute (hub) via a high-definition webcam. 24 The neurologist viewed the image of the patient's computed tomography brain scan via high-speed internet connection. An ED physician assisted and communicated with the neurologist in real time until a diagnosis of thrombolysis was reached.
Low et al. also applied this model to the telegeriatric system in Singapore. The telemedicine system used a hub (hospital) and spoke (nursing home) model. 25 Teleconsultation sessions were performed with each nursing home two to three times per month. The telegeriatric nurse presented the patient's clinical findings to the specialists, and the doctor and nurse completed the diagnostic workup and care plan on the telegeriatric consultation form. Then, the doctor reviewed and signed off on the telegeriatric consultation form and sent the form back to the nurse via email.
A store-and-forward model was also used for telepathology in Cambodia, 26 telemedicine for retinopathy in Thailand, 27 and teledermatology in Singapore. 28 Kadaba et al. used a hybrid telepathology network based on store-and-forward communication using the Internet Pathology Suite (iPATH) network and videoconferencing using Skype (Microsoft Corporation, Luxembourg). Tissue slides were prepared at a Cambodian laboratory, and images were captured and uploaded to the iPATH network along with diagnostic comments. Specialists worldwide who were invited to join the iPATH network were notified of the meeting and used the opportunity to provide a second opinion on the cases. In addition, telemonitoring was used to monitor patients who were implanted with cardiac implantable electronic devices.
COMMUNICATION
Included studies used several methods for remote communication between patients and doctors, or between health care providers. Video consultation was used in many telemedicine systems for communication between patients and health care providers. 24,28 –35 Videoconferencing or teleconferencing was used to communicate between health care providers, internal and external to the organization, to discuss with patients. 25,26,31,33 –43 Telephone and SMS were the most common systems used by health care providers to contact patients and other health care partners. 35,36,40,44 –47
TECHNOLOGY
Skype and Zoom (Zoom Video Communications, Inc.) were used for videoconferencing. Line (LINE Corporation, Japan) was used for real-time communication in both chat and video call. Email and SMS were used to communicate between nursing homes and physicians. YouTube (Google LLC) was used to provide education for health care staff and patients. A digital fundus camera was the main device used in teleophthalmology. Some studies developed their own communication methods for use with telemedicine systems. For example, Tan et al. developed the teleophthalmology software that allowed offline data retrieval and real-time sampling of patient data. 36 The data were transferred from the primary care centers to the main hospital securely via hospital networks in Singapore.
ISSUES AND LIMITATIONS
Most included studies had a small sample size and were of short duration. The Hawthorne effect, which is a change in behavior as a motivational response to the interest, care, or attention received through observation, assessment, or experiment, may be present. 48 Implementation of complete telestroke with both video-teleconferencing and teleradiology is expensive for developing countries to operate and sustain. Low-quality images or unreadable images diminished the ability of physicians to effectively evaluate patients' presentations. In addition, telemedicine software systems and equipment were frequently down resulting in delays in service and diagnoses. Staff members were not familiar with the use of telemedicine equipment, and physicians were not experienced in using teleconsultation programs. Each of these elements diminished the potential for telemedicine having a strong positive impact on SEA patients.
The ability to effectively conduct a clinical examination and assessment is the major limitation in telehealth, resulting in inaccurate physical examinations and clinical findings. Clinical staff often did not have time to obtain informed consent, and as a result, the documentation produced was inconsistent and incomplete. Moreover, primary care centers did not have electronic health records available and lacked standardized, reliable medical records. Patients were easily lost to follow-up or difficult to track when they were transferred to another hospital, and some patients were unable to understand the recommendations that health professionals provided by telephone. Technological barriers, inability to use technology, and difficulty accessing a good quality internet connection were additional common problems.
QUALITY OF INCLUDED STUDIES
Utilizing the STARE-HI principles, 22 two risks of bias graphs were created and summarized (Figs. 3 and 4). Almost half of the studies were at high risk or unclear due to the methods used to perform the data analysis and the study design, whereas most of the studies were at low risk of bias in a participant domain. For study design, 24 studies (64%) were at low risk of bias and 4 studies (11%) were at high risk. For theory and background, 25 studies (68%) were at low risk of bias and 12 studies (32%) were at high risk. We identified several studies (87%) that adequately described the method for selecting participants, users, patients, units, or hospitals.
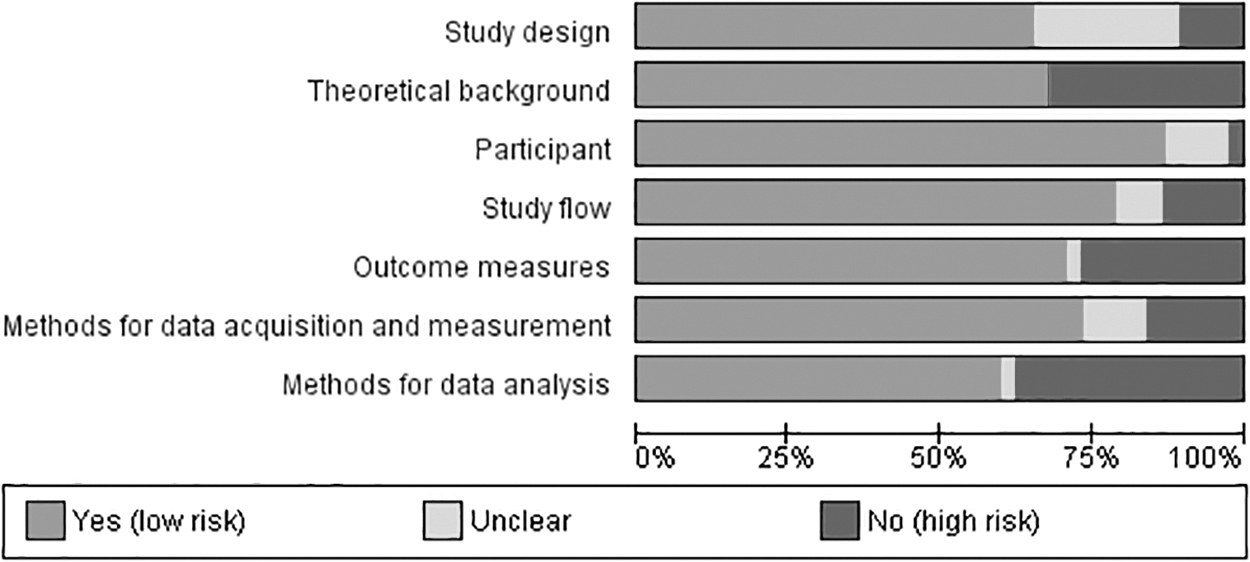
Risk of bias graph: review authors' judgment about each domain presented as percentage across included studies.
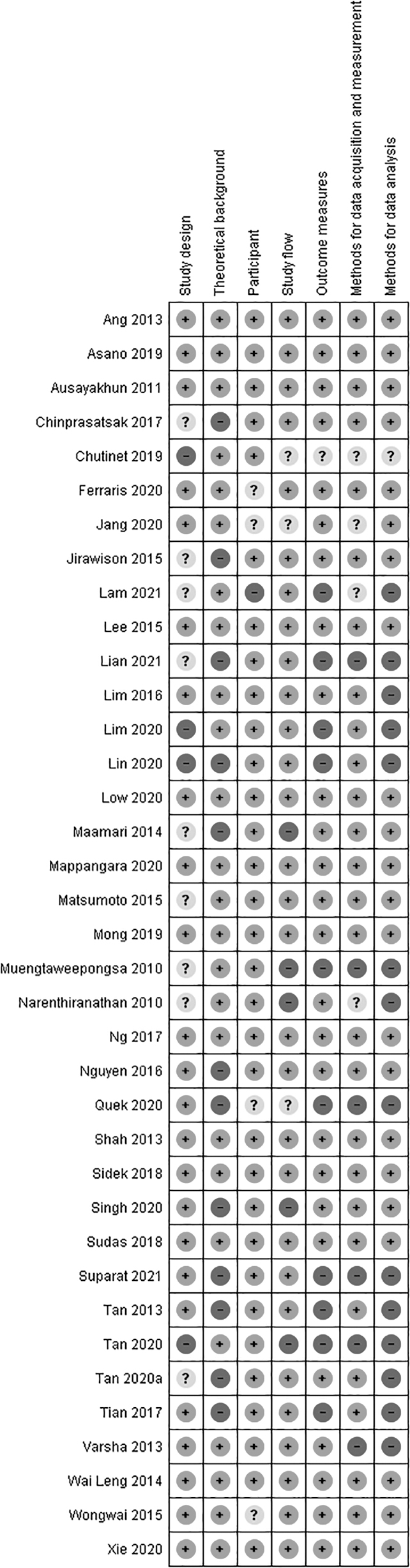
Risk of bias graph: review authors' judgment about each domain for each included study.
Twenty-nine studies (78%) provided sufficient details on study flow, including study period, study activities, timeline of activities, or flow diagram. Twenty-six studies (70%) clearly defined the outcome or other variable measures that were used in the studies, whereas 10 studies (27%) were at high risk. Methods for data acquisition and measurement, such as questionnaires, interviews, observations, type of data collection, were described sufficiently in 27 studies (73%).
For methods of data analysis, 14 studies (38%) were at high risk of bias as they did not describe details of data analysis in terms of quantitative and qualitative methods. Furthermore, we found that many studies were at high risk of bias because of small sample sizes.
Discussion
As a result of the COVID-19 pandemic, the authors observed that the number of research studies conducted on the various aspects of telemedicine increased in 2020. Overall, most of the included studies were conducted in Singapore (49%). This systematic review also demonstrated that a hub-and-spoke modality was widely used throughout the SEA region, and the majority of telemedicine systems were hospital-based with teleophthalmology being the most common, followed by teleconsultation. A descriptive study design predominated, followed by retrospective and cross-sectional studies.
The World Health Organization ranked the national health care system in Singapore as the sixth best system in the world based on the program's excellent medical ICT capabilities. 49,50 Among Asian countries, Singapore is a leader in applying information technology to the health care industry. In 2000, the government deployed the Singapore One Infrastructure, which built and enabled an e-government and e-health environment 49,51 that included high-speed broadband internet and appropriate technology to implement telemedicine applications throughout the country. 52
The National Telemedicine Guidelines (NTG) addressed the relevant components for the delivery of telemedicine services by health care providers through four domains: “Clinical Standards and Outcomes,” “Human Resources,” “Organisational,” and “Technology and Equipment.” The NTG is the only guideline among SEA countries that addresses the scalability, maintenance of the technology, equipment calibration, end of life and e-waste disposal, upgrade and replacement of appropriate technology, and equipment. 18,52
The hub-and-spoke model was the most widely used telemedicine system. 53,54 Although the model provides many benefits, it has risks due to congestion at hubs, overextension of spokes, staff dissatisfaction at spokes, and transportation disruptions. 53 The store-and-forward concept, in which medical information is collected, compiled, and transferred through the internet, is also used in many telemedicine systems. 55 This concept is the main methodology for deploying telemedicine services in Singapore. 56 Moreover, Deldar's systematic review of teleconsultation and clinical decision-making revealed that the store-and-forward model was used by 31% of included studies. 57
Ibrahim et al. reported that most health care professionals were dissatisfied with the reduction in face-to-face communication with their patients. 58 Ibrahim et al. also noted that the success of telemedicine depended on the perception and knowledge of the participating health care professionals. 58,59 Our study found that staff members and/or physicians were uncomfortable using telemedicine or teleconsultation equipment 28 probably because they had limited familiarity with the technology. Thus, the lack of comfort and skills of health care workers clearly had a negative effect on the adoption of telemedicine systems and services in SEA countries. 60
Similarly, a systematic review by Durrani and Khoja of telehealth in Asian countries found that untrained service providers, including physicians and staff, were the most significant barriers to the successful implementation of telehealth. 61 Health care organizations and institutions should provide training, instructional materials, and resources about telemedicine to ensure that staff are capable of using the system effectively. Telemedicine has the potential to have a greater impact on health care practice in developing countries than in developed countries 59 if health care professionals could be motivated to learn how to use the systems effectively in both rural and urban areas. 58
Telemedicine programs in developing countries were frequently small-scale pilot or informal projects with limited implementation. 12 High telecommunication and device costs were the major barriers to implementing telemedicine systems in many Asian countries, 61 and ICT resources were frequently unavailable in clinical units. 62 By contrast, health care providers and patients frequently used a telephone, SMS, multimedia messaging system, Line, Facebook Messenger, iMessage, WhatsApp, Chatbot, and email to communicate with each other. 37,62 –64
Health care providers also used messaging applications in their daily work to share information with colleagues. 65 Although using free messaging applications provided many advantages to improving communication, it likely increased the risk of exposing data to privacy and security abuses. 65 –67 While the applications available are free, they may not offer the sophisticated technology that is needed to conduct effective telemedicine patient–physician interactions in a safe and secure environment. 68
The inability to conduct clinical and physical examinations was the most serious limitation of telemedicine when compared with face-to-face interactions. For example, doctors and therapists experienced difficulty evaluating and managing several cases using telerehabilitation because of their inability to operate the program. Both patients and providers lacked the knowledge, skill, and technical know-how to interact during telemedicine services. 69
Another significant barrier perceived by the therapists was patient assessments, such as the inability to physically test muscle power or balance 70 as well as the barriers of interaction between the patient and the therapist. A mixed method study conducted by Lee et al. 71 found that most participants preferred telemonitoring.
Clearly, technology issues are the biggest barriers to successful implementation of telemedicine. Finally, it is important to note that some participants were concerned about sharing their data with family members and were concerned about malware that could infiltrate telemonitoring devices and attack their personal information.
Conclusions
The review was conducted using a rigorous methodology and transparency. A comprehensive literature search was conducted using a variety of databases and related sources to retrieve all related studies on telemedicine in SEA countries. The present study had some limitations. First, we did not include studies of m-health or e-health as the goal was to focus on the overall implementation of telemedicine systems. Second, articles were included only from the last 11 years of published peer-reviewed studies. Third, no gray literature was included. Moreover, a meta-analysis could not be conducted because of heterogeneity among included studies.
The overall finding of the present review provides an important perspective on the use and implementation of telemedicine across SEA settings. Studies on clinical applications of telemedicine are critical to inform the usability and quality of the systems, but there was limited information and a lack of good quality studies to assess. Most research efforts were conducted with a small sample size without calculation, which had no power to estimate the difference. Thus, generalizability is limited to the study settings only.
The review illustrates that telemedicine is a powerful tool. It is feasible, safe, effective, and less expensive than traditional methods. However, the unintended consequences of health information technology 72 are less likely to be reported in telemedicine studies. Robust research is needed to fully investigate more effective training, patient safety, use, and implementation of telemedicine systems in the Southeast Asia region.
Footnotes
Acknowledgments
We gratefully acknowledge Ross Koppel, PhD, for his valuable comments and suggestions to our project. We would like to thank Dr. Monique Saran for her idea to explore the topic of telemedicine.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.