
Abstract
Introduction:
Teleneonatology (TN) allows remote neonatologists to provide real-time audio-video telemedicine support to community hospitals when neonates require advanced resuscitation or critical care. Currently, there are no published economic evaluations of U.S. TN programs.
Objective:
To evaluate the cost of TN from the perspective of the health care system.
Methods:
We constructed a decision tree comparing TN to usual care for neonates born in hospitals without a neonatal intensive care unit (NICU) who require consultation. Our outcome of interest was total cost per patient, which included the incremental cost of a TN program, the cost of medical transport, and the cost of NICU or non-NICU hospitalization. We performed threshold sensitivity analyses where we varied each parameter to determine whether the base-case finding reverted.
Results:
For neonates requiring consultation after birth in a hospital without a NICU, TN was less costly ($16,878) than usual care ($28,047), representing a cost-savings of $11,168 per patient. Sensitivity analyses demonstrated that at least one of the following conditions would need to be met for TN to no longer be cost saving compared to usual care: transfer rate with usual care <12% (base-case = 82%), TN reducing the odds of transfer by <8% (base-case = 52%), or TN cost exceeding $12,989 per patient (base-case = $1,821 per patient).
Conclusions:
Economic modeling from the health system perspective demonstrated that TN was cost saving compared to usual care for neonates requiring consultation following delivery in a non-NICU hospital. Understanding the cost savings associated with TN may influence organizational decisions regarding implementation, diffusion, and retention of these programs.
Introduction
Teleneonatology (TN) is the use of real-time, audio-video telemedicine to support neonatal care from a distance. TN connects neonatologists with care teams in community hospitals that do not have a neonatal intensive care unit (NICU). Through telemedicine, neonatologists can visualize the neonate, guide care teams through complex resuscitations, and provide consultation for neonates requiring critical care. 1 –3
As telemedicine becomes integral to health care delivery, program value must be evaluated, which may include metrics such as quality of care, patient safety, patient and family experience, and cost of care. TN has been shown to improve the quality of high-risk neonatal resuscitations that occur in community hospitals without a NICU. 4 In addition, evidence suggests that TN facilitates safer care as illustrated by improved adherence to the standard of care 5 and reduction in settled birth injury cases. 6 Importantly, TN enhances collaboration between the remote neonatologist and the community hospital care team; thus, facilitating patient triage and reducing the likelihood that a neonate will require transfer to a higher level of care. 3,7,8
Pediatric telehealth programs are especially crucial given the vulnerability of and health disparities seen in this patient population. 9,10 Economic evaluation of these care models based on the entire health care system is critical for establishing value, ensuring payment, and maintaining program funding. 9 While there is evidence of the positive impact of TN on patient care, there have been no published economic analyses of U.S. TN programs. The aim of this study was to evaluate the cost of TN from the perspective of the health care system.
Methods
For this study, cost was defined as the per-patient cost of TN compared to usual care for a neonate requiring consultation after birth in a hospital without a NICU. Usual care was defined as neonatal care provided by staff at the non-NICU birth hospital, with or without phone consultation by a neonatologist. The costs of care for each cohort were determined using published literature and informed by any between group differences in rate of transfer to a higher level of care and cost of hospitalization. The health care system was defined as the hospital providing TN consults, the non-NICU community hospital receiving TN consults, and interfacility medical transport services. The Mayo Clinic Institutional Review Board (IRB) deemed this study exempt from review (Mayo Clinic IRB#20-002524).
DECISION TREE OVERVIEW
A decision tree models the progress of individuals under different treatment strategies. Various clinical events may be included and will depend on the condition of interest. For example, in the context of TN, events included transfer rate, mode of transfer, and NICU and non-NICU hospital stays. Decision tree models are often restricted to a specific timeline (e.g., weeks, months, years) depending on the specific duration for which the effects of the intervention need to be assessed. Costs are accrued for the chosen duration and weighted by the probability that an event may occur. Sensitivity analyses, which assess the impact of specific parameters on model predictions, typically accompany modeling studies, including decision trees.
TN DECISION TREE
We constructed a decision tree comparing TN to usual care for neonates born in hospitals without a NICU who required consultation after delivery. We constructed our model in TreeAge Pro v.2019. Our outcome of interest was total cost per patient, which included the incremental cost of a TN program, the cost of medical transport, and the cost of NICU or non-NICU hospitalization. A diagram of our decision tree is shown in Figure 1. Our timeline included the initial NICU or non-NICU hospitalization, as applicable. Due to the short duration of the model timeline, no discounting of cost was needed.
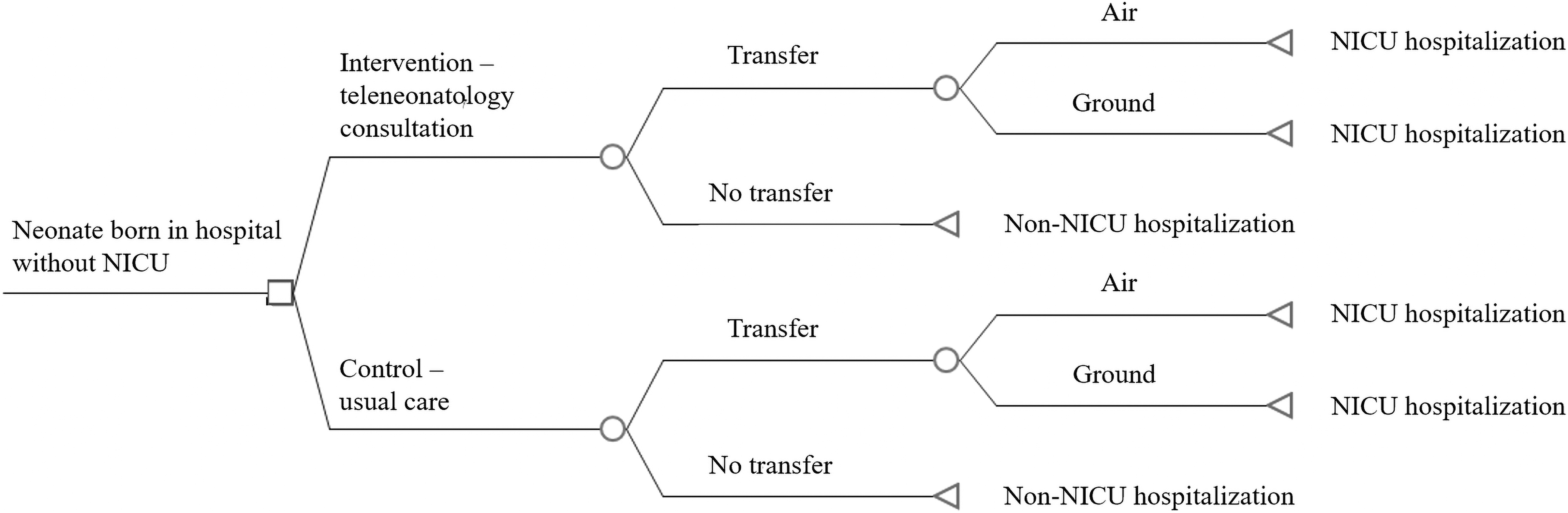
Cost decision tree for TN. Square = decision node; circle = chance node; triangle = endpoint node. NICU, neonatal intensive care unit; TN, teleneonatology.
MODEL PARAMETERS
The parameters used in the base-case model are summarized in Table 1. Model parameters for differences in transfer rates between usual care and TN were taken from Haynes et al. 7 In brief, this study evaluated neonatal transfer rates in six rural California hospitals over a 4-year period. The authors demonstrated that 64% of infants who received TN were transferred compared to 82% of infants who received telephone consultations (usual care). The adjusted odds of transfer following TN compared to phone consultation was 0.48 (95% confidence interval: 0.26, 0.90, p = 0.02), which was the value used in our base-case model.
Model Parameters
NICU, neonatal intensive care unit; TN, teleneonatology.
We estimated the proportion of transfers that occur by air versus ground and assumed in the base-case model that the proportion of transfers would be equivalent in the TN and usual care arms. Thus, we estimated that 50% of neonatal transports would be by air (rotor or fixed wing) and 50% by ground, recognizing that the percentages may vary widely based on location, geography, transport distance, patient acuity, and so on. 11 –14
There are no published reports on the cost of TN programs. Therefore, TN costs were estimated using the published costs of other similar acute care telemedicine programs, that is, pediatric tele-critical care and telestroke. We averaged the total costs reported in two studies on telestroke ($597 to $1,049 per patient) and one study on pediatric critical care tele-consultations to rural emergency departments (EDs) ($3,641 per patient). The average cost was updated to 2020 U.S. dollars (USD) to generate the $1,821 per patient cost of TN used in the base-case model. 15 –17
For the cost of transfers, we used published Medicare reimbursement rate formulas
18
:
We estimated mileage based on Karlsen et al., which found that neonatal transport teams most commonly report a 1-way transport radius of 51–100 miles or 101–200 miles depending on the team type. 12 Based on these data, we used a mileage estimate of 200 miles roundtrip.
There are no published data on the cost of NICU and non-NICU hospitalization for newborns requiring neonatology consultation after delivery in a hospital without a NICU. Therefore, we estimated these costs using the 2018 Hospital Inpatient National Statistics. 19 Using the HCUPnet tool, we selected the neonatal Medicare-Severity Diagnosis Related Group (MS-DRG) codes. We classified MS-DRG codes 792 (prematurity without major problems) and 794 (neonate with other significant problems) as non-NICU discharges. MS-DRG codes 789 (neonates, died, or transferred to another acute care facility), 790 (extreme immaturity or respiratory distress syndrome, neonate), 791 (prematurity with major problems), and 793 (full-term neonate with major problems) were classified as NICU discharges (Table 2). 20
Non-neonatal Intensive Care Unit and Neonatal Intensive Care Unit Hospitalization Cost Estimation Using the 2018 Hospital Inpatient National Statistics
In 2018 USD.
DRG, Diagnosis-Related Group; MS-DRG, Medicare-Severity Diagnosis-Related Group; USA, U.S. dollar
Of note, we excluded DRG 795 (normal newborn) as these neonates would be unlikely to require consultation, and therefore would not be included in our model. The weighted average cost per patient discharge was calculated by first multiplying the total number of discharges in each MS-DRG group by their respective mean hospital costs. Then, we divided the total aggregated costs by the total number of hospital discharges. Estimated non-NICU and NICU hospital costs were updated to 2020 USD using the Consumer Price Index (CPI) price deflator. 21 For the base-case model, we used a non-NICU hospital cost of $3,067 and a NICU hospital cost of $28,615.
SENSITIVITY ANALYSIS
We performed threshold sensitivity analyses where we varied each parameter, one at a time while holding all others constant, to determine whether the base-case finding reverts, and if so, by how much. Specifically, we focused on varying the probability of transfer, mode of transport, cost of TN, and the cost difference between NICU and non-NICU hospitalization. Identifying how changes in the various model parameters impact TN costs may influence organizational decisions on TN implementation, retention, and diffusion.
Results
BASE-CASE ANALYSIS
In our modeled cohort of newborns requiring neonatology consultation after birth in a hospital without a NICU, TN was less costly ($16,878 per patient) than usual care ($28,047 per patient), representing a cost-savings of $11,168 per patient. This base-case model assumed an 82% newborn transfer rate for usual care, a transfer rate odds ratio of 0.48 for TN, transport mode equally distributed between ground and air for both usual care and TN, and a TN cost of $1,821 per patient.
SENSITIVITY ANALYSIS
We used threshold sensitivity analysis to identify when TN would no longer be cost saving and would instead favor usual care. Three variables had a threshold at which TN became costlier than usual care: the transfer rate for usual care, the odds ratio for transfer with use of TN, and the cost of TN (Fig. 2).
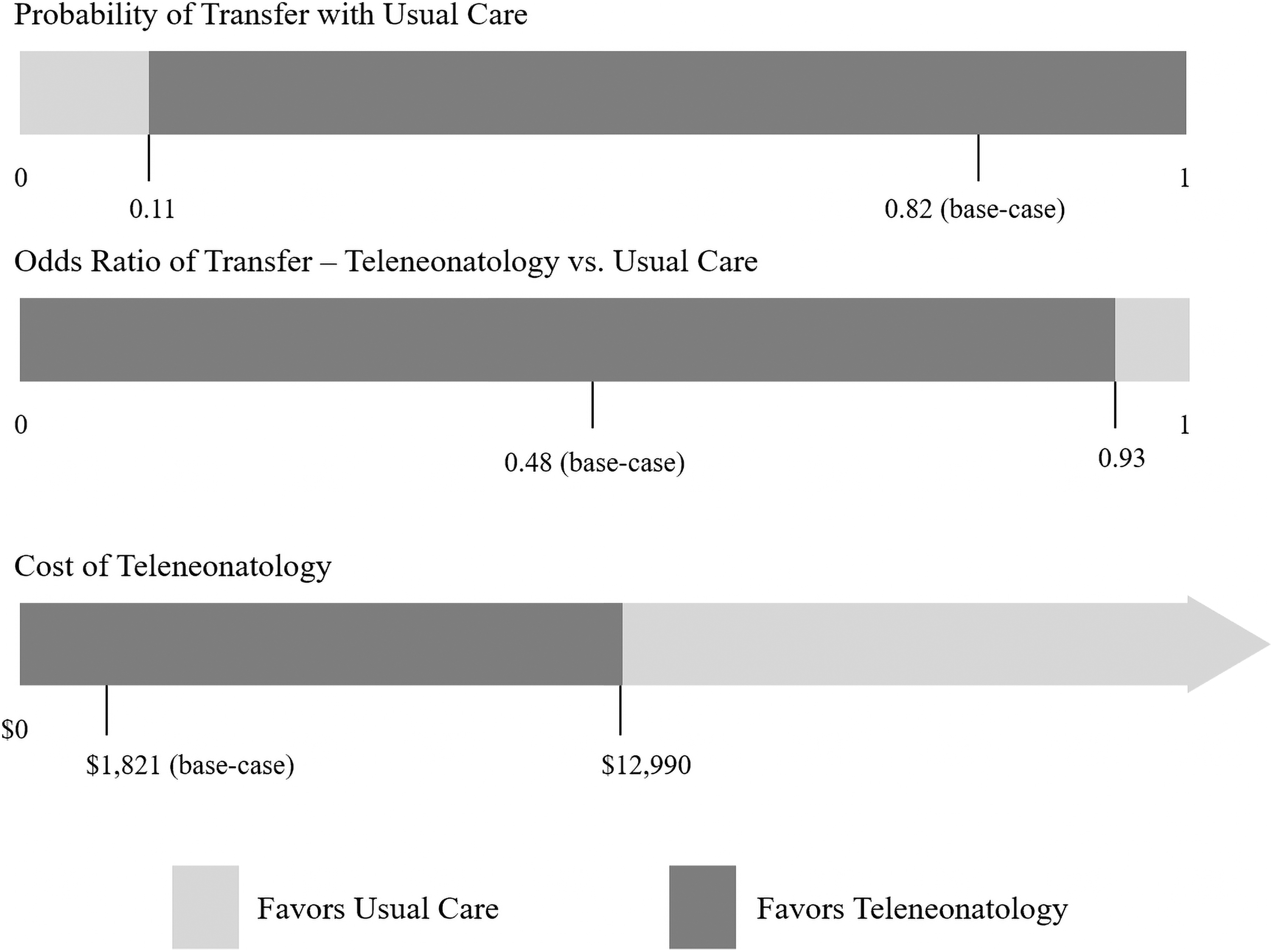
Threshold sensitivity analysis for when TN would no longer be cost saving compared to usual care.
The base-case value for rate of transfer to a higher level of care for neonates receiving neonatology consultation under usual care was 82%. We found that if the transfer rate for neonates requiring consultation fell below 12% for usual care, TN would no longer provide cost savings. Furthermore, in the base-case model, TN reduced the odds of transfer by 52%. We found that if TN reduced the odds of transfer by less than 8%, then TN would no longer be cost-saving.
The per-patient cost of the TN program also impacted cost savings. In our base-case model, TN cost $1,821 per patient and TN was cost-saving compared to usual care. We found that TN would remain cost-saving up to a cost of $12,989 per patient. When the cost of TN exceeded this amount, then TN would become costlier than usual care.
We further looked at the mode of transport (air or ground) between TN and usual care. We found that even if all TN transfers were by air and all usual care transfers were by ground, TN would remain cost-saving ($18,169) compared to usual care ($25,358).
The cost of NICU and non-NICU hospitalizations did not change the cost savings associated with TN. For example, we tested a cost difference of $0 between NICU and non-NICU hospitalizations and found that TN was still cost saving ($6,821) compared to usual care ($7,093). In other words, even in the unlikely circumstance where the cost of a non-NICU stay was the same as the cost of a NICU stay, TN would still be cost saving.
Discussion
Using a decision tree model, we demonstrated that TN resulted in an estimated cost savings of $11,168 per neonate requiring consultation after birth in a non-NICU hospital. Our sensitivity analyses showed that TN remained cost saving for the health system as long as the transfer rate with usual care (i.e., phone consultation) was ≥12%, TN reduced the odds of transfer by at least 8%, or the cost of TN did not exceed $12,989/patient (assuming other model parameters remained constant). This economic analysis demonstrates that TN generates value by reducing health system costs – building on previous studies that have shown the value of TN through improved quality of care and patient safety.
Our economic evaluation supports and strengthens previous work that secondarily estimated the financial impact of TN based on cost savings associated with reduced transfer rates. 1,3,8,22 TN programs in California and Utah reduced the odds of patient transfer following consultation by ∼30–50%. 7,8 The latter program estimated that reducing medical transports from the eight community hospitals in their TN network corresponded to a cost savings of $1.2M/year. 8
Similarly, a tele-NICU program in Texas found that about 55% of neonates were able to remain at the originating hospital following consultation, resulting in ∼$0.9M in saved transport costs. 3 Finally, a neonatal tele-consultation program in Queensland, Australia, demonstrated that 26% of transports were avoided, resulting in a net health systems savings of AUD 54,400 per year (about USD 40,000). 22 The authors projected if tele-consultation was used for all retrievals from the four originating hospital nurseries, the net savings would be AUD 206,073 (about USD 150,000).
The favorable cost analysis for TN is similar to findings from systematic economic evaluations for other acute care telemedicine programs, for example, telestroke and tele-emergency medicine. From a societal perspective, a telestroke network was cost saving and more effective compared with no network, when including initial and recurrent stroke treatment, rehabilitation, long-term care, and caregiver costs. 23 Similarly, accounting for technology costs, hospital revenues, and patient-associated savings, an adult tele-emergency medicine program resulted in a net savings per avoided transfer. 24 A cost-effectiveness analysis of telemedicine consults to children in rural EDs demonstrated telemedicine was less costly than telephone consultation, resulting in a cost reduction of about $4,600 per child/ED/year. 17
There are limitations and assumptions within the current study that warrant discussion. In our base-case model, we estimated the proportion of transfers by air and ground. In practice, this will vary by health system and is dependent on many factors. Furthermore, our model used a short timeline that terminated after the initial non-NICU or NICU hospitalization. Future models may consider a longer timeline, a different perspective (e.g., societal perspective that includes family costs such as travel, meals, and lodging), or evaluate cost-effectiveness based on short- and long-term health outcomes such as mortality and serious morbidity. Finally, costs used in the model were based on previously published data or the Centers for Medicare and Medicaid Service (CMS) fee schedule. Actual costs will vary by health system, although we aimed to capture cost variation in our sensitivity analyses.
Conclusions
Economic modeling from the health system perspective demonstrated that TN was cost saving compared to usual care for neonates requiring consultation following delivery in a non-NICU hospital. The cost savings was sensitive to baseline transfer rates with usual care, the degree to which TN reduced the odds of transfer, and the cost of the TN program. Understanding the cost savings associated with TN may influence organizational decisions regarding implementation, diffusion, and retention of these programs.
Footnotes
Authors’ Contributions
V. T. designed the decision tree, carried out the analyses, drafted the initial article, reviewed and revised the article, and approved the final article. R.D. assisted with data analyses, critically reviewed the article for important intellectual content, and approved the final article. B.L.K. conceptualized the study, critically reviewed the article for important intellectual content, and approved the final article. J.P.M. provided guidance on decision tree construction, critically reviewed the article for important intellectual content, and approved the final article. C.E.C. conceptualized the study, critically reviewed the article for important intellectual content, and approved the final article. B.M.D. conceptualized the study, critically reviewed the article for important intellectual content, and approved the final article. B.J.B. conceptualized the study, critically reviewed the article for important intellectual content, and approved the final article. J.L.F. conceptualized the study, drafted the initial article, and reviewed and revised the article, and approved the final article.
Disclosure Statement
J.L.F. and C.E.C. have licensed intellectual property and earn royalties from Teladoc Health, and J.L.F. owns stock in the company. The other authors have no conflicts to disclose.
Funding Information
This study was partially funded by the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Minnesota.