
Abstract
Background:
Rural injured workers requiring multidisciplinary assessments for musculoskeletal disorders face health access disparities, which include travel to urban centers. Virtual care can enhance access to multidisciplinary team care for musculoskeletal conditions in rural areas.
Materials and Methods:
A retrospective chart audit of 136 multidisciplinary assessment reports of injured workers was conducted. Comprehensive management recommendations from the health care assessment team were extracted for analysis. The health care team used virtual technologies to join with patients and at least one local rural health practitioner in one of three locations. Remote presence robotics (RPR; Xpress Technology™) or laptop-based telehealth was used to complete the assessments.
Results:
RPR were used in 46% of assessments over two sites, with 54% using laptop-based telehealth at a third site. Frequencies of team members' assessment using technologies were as follows: physical therapist (100%), psychologist (78%), plastic surgeon (8%), and physician (43%). Spine (42%) and shoulder (32%) disorders were the most common problems. Most workers (79%) were 3 or more months postinjury. The most common management recommendation was the need for daily comprehensive rehabilitation care (76%). Travel time was saved by 89% of participants.
Conclusions:
Virtual care was used to unite multidisciplinary assessment teams for the evaluation of injured rural workers with complex musculoskeletal injuries. Future research recommendations include comparing between virtual and fully in-person multidisciplinary assessment and recommendation findings, and evaluation of patient and practitioner experiences with comprehensive virtual team assessments.
Introduction
People living in rural and remote areas experience health care access barriers 1 –4 (e.g., health care after a work injury) and typically score lower on health indices such as mortality. 5 –7 If health care cannot be obtained in a timely manner, poor clinical and economic outcomes can be expected. 8 Health care access has been described by Anderson and Davidson 9 as having the following key components: availability, accessibility, accommodation, affordability, and acceptability to the patient. Russell et al. 10 included timeliness and geography as additional considerations for health care access. Traditionally, rural residents travel to urban centers following a work injury for assessment and treatment, which is a health care access barrier. There is scant research examining how virtual assessments are used for improving health care access to injured workers. 11 There is also a paucity of research on virtual technology utilization in health care teams' complex decision-making processes.
The Canadian province of Saskatchewan has ∼35% of residents living in rural or remote areas, which is about double the national proportion of 17%. 12 Rural residents contribute to Saskatchewan's economy through work in physically demanding industries, such as resource development (e.g., mining), health care, agriculture (e.g., farming), manufacturing, and transportation. 13 Lavoie et al. compared rural injured workers with urban injured workers in the Canadian province of Alberta and noted that rural workers were: older, had less formal education, worked more often in blue-collar industry, had lower salaries, 7 were more likely to have dislocations and lower back injuries, and were less likely to have rehabilitation after evaluation for return to work (RTW) planning. 7
Saskatchewan's labor-intensive rural economies, and the workers within it, require health care teams to engage in a complex decision-making process to determine medical management and rehabilitation, as well as RTW guidelines. Providers who may be needed for this planning include: physical therapists, occupational therapists, chiropractors 11 as well as physicians, psychologists, and specialists such as orthopedic and plastic surgeons. 14
Unfortunately, rural locations have fewer care providers and specialists compared with urban centers, and they are more geographically spread out. 6,15 –18 For example, physical therapy is a common need following musculoskeletal injury, as early access can reduce opioid prescription for back pain. 19 Unfortunately, only 10% of Saskatchewan's physical therapists work in rural locations, which indicates that an access barrier exists. 15 Another rural Canadian health care barrier is access to mental health professionals. 20 Rural citizens have higher rates of depression, 8 which can potentially be exacerbated by both the inability to receive timely treatments 6,15 –18 and the diminished sense of control that workers often report when dealing with third-party payers. 21,22
There are limited data about rural psychologist practice in Saskatchewan; however, a 1999 publication by the Canadian Psychological Association reported only one practicing psychologist in rural Saskatchewan that year, 23 and a report in 2013 indicated that waitlists measured in months. 24 Medical specialist consultation is another rural Canadian health care access barrier. One report indicated that only ∼2% of all plastic surgeons live rurally. 25 Innovative solutions to accommodate access to multidisciplinary teams may facilitate more timely access to care and improved health outcomes for injured rural workers.
Virtual applications in health settings such as remote presence robotics (RPR) and telehealth are increasing and include use for musculoskeletal injuries, 26 –28 work-related injuries, and occupational rehabilitation. 11 Virtual care may produce comparable clinical outcomes to traditional health care experiences in some instances. 29,30 From a physical health perspective, virtual assessments have high validity for assessing pain, swelling, joint range of motion, muscle strength, gait, functional assessments, 27 and balance. 31,32 Other virtual care studies demonstrate good satisfaction 33 –35 and experience of patients and providers. 26,36
There is a paucity of research, however, evaluating team-based musculoskeletal care, 37 which is a critical component in the evaluation and management of complex work-related musculoskeletal injuries. Research is also limited in the evaluation of hybrid care models (combination of in person and virtual care), the use of virtual strategies for management of injured workers with complex conditions, and evidence demonstrating the financial impact of virtual care.
The purpose of this study was to describe the demographics, assessment findings, multidisciplinary assessment team composition, management recommendations, and travel implications associated with multidisciplinary team assessments for rural injured workers. Virtual technologies were used to unite the assessment teams with injured workers and their rural health practitioners.
Methods
A retrospective chart review was completed on assessment reports compiled by a multidisciplinary team consisting of urban health professionals collaborating with rural team members and injured worker patients using virtual technologies. Data were extracted by one research team member. There were 141 patient charts, with 5 charts discarded due to absenteeism (e.g., the patient failed to show for their appointment), leaving 136 charts left for review.
MULTIDISCIPLINARY TEAM AND PATIENT ASSESSMENT PROCESS
The in-person component of the assessment occurred at one of three rural sites within the Canadian province of Saskatchewan. At least one local team member was present with the injured workers at all times, with remaining team members joining from other locations using RPR or telehealth. The RPR was the Teladoc Health Xpress V2™, a portable device facilitating live audio and video, as well as adjunctive capacities including Littman Bluetooth stethoscope. 38 The RPR stethoscope assessment tool was required for medical screening examinations at sites when the physician was located remotely. The telehealth software utilized at the third site was Zoom for Healthcare™. 39 An administrative coordinator ensured a streamlined process of appointment timing so remote health providers could join the patient and rural team member at the scheduled times.
All incoming referrals for multidisciplinary assessments, as well as the associated documents, were received electronically through a portal system managed by a third party and were maintained in accordance with the Saskatchewan College of Physical Therapists regulations. 40 Each team member had access and reviewed pertinent case information before assessment. The administrative coordinator ensured collation of paperwork and communication between practitioners for consistency in file management.
Informed consent was received for clinical assessment as per clinical and regulatory requirements. This included discussion of the purpose and expectations of assessment, as well as explanation of virtual components. Following consent, each practitioner completed their assessment and discussed findings and recommendations for follow-up care. The practitioner who served as the team lead and report writer prepared the document containing final assessment and management recommendations, which was the data source from which the retrospective chart review occurred. Ethics for this project was received from the University of Saskatchewan's Biomedical Research Ethics Board (Bio ID No. 781).
Variable definitions and subcategories
Forty-three data categories were extracted and can be viewed in Table 1.
Description of Data Variables Extracted
TRTW, transitional return to work.
Demographics
“Patient residence” was classified as urban or rural by using the first three digits of the patient's home area code. 41 “Job category” was classified using publicly available industrial categories from a third-party payer. 42 “Work status” identified whether the client was working in some capacity at time of assessment. Workers coded as not working were further classified with an employment status of unemployed or employed at time of assessment. “History of depression” and “history of anxiety” were extracted from the patient's medical history and the psychological profile assessment, which was completed by a psychologist. “Comorbidities” included conditions such as diabetes mellitus, hypertension, neurological, and other medical conditions. Multiple surgeries occurring on the same body part were coded as one incidence of “musculoskeletal surgery.”
Remote assessment characteristics
“Patient's closest assessment site” was a comparison of kilometers required to travel from their residence to both the remote assessment site (where the patient actually went for their assessment) and the closest urban assessment where a fully in-person assessment could occur. The two distances were compared, and the assessment site associated with shortest distance was documented. The item “round-trip time saved” was the distance the patient traveled to their remote assessment subtracted from how far they would have traveled for a full in-person urban assessment. Three cases were removed from this analysis because the worker's home address was out of province. This round-trip time estimate is not reflective of how kilometer per diem is calculated, and thus, the data herein were not converted for these purposes.
“Level of assessment” described secondary or tertiary level of assessment. Tertiary assessments typically include a psychological evaluation and/or other medical specialist consultation. “Assessment time per team member” was a calculation of the total time taken per initial assessment divided by the number of team members (physically present and joining remotely).
Assessment findings
“Primary injury” was transcribed from the initial assessment report, and the anatomical location of the injuries was converted into an injured body part classification system, which is publicly available. 42 The variables “current depression” and “current anxiety” were extracted from the patient's psychological profile, which was evaluated by a psychologist during tertiary assessments. The “Roland Morris Questionnaire” 43 was subdivided into 4-point intervals. 44 The psychological tools used in the initial assessment did not have the raw scores present for data extraction as they were individually calculated by the psychologist (see Table 1 for Depression Anxiety Stress Scale, Million Behavioral Medicine Diagnostic, and the Current Problem Checklist).
Hence, these items were only coded as being used in the assessment (yes or no). The Pain and Activity Questionnaire was stratified into low, medium, and high categories. 45 Neck Disability Index stratifications were none, mild, moderate, severe, and complete. 46 A detailed explanation of the Dictionary of Occupational Titles (DOT) subcategories can be found within the study by Cain and Treiman, 47 and the U.S. Department of Labor. 48
Proposed treatment
“Treatment level” described the follow-up rehabilitation required for optimal care (primary, secondary, or tertiary). “Treatment education” described patient education recommended (stages of tissue healing, symptom control, posture, nutrition, hurt versus harm principles, lifting strategies, and pain management). This variable was coded as “all courses,” “select courses,” or “none.” Transitional return to work (TRTW) is a recommendation to initiate some return to workplace functioning at the onset or early during rehabilitation programming in an alternate job role.
Graduated return to work (GRTW) is a recommendation to start the RTW process in the preinjury job role near the end of or following formal rehabilitation programming. Permanent disability relating to the preinjury occupation is the expectation of post-treatment permanent functional impairment that will likely not allow a full return to all the previous preinjury job hours and/or duties. Hence, a person with a permanent disability relating to preinjury occupation would still have either a TRTW or GRTW plan recommendation, and some level of function would be expected.
STATISTICAL ANALYSIS
Data were entered into a Microsoft Excel 49 spreadsheet. The following descriptive statistics were applied to all variables: frequency, percentage, median, and interquartile range (IQR).
Results
DEMOGRAPHICS
Demographic variables are described in Table 2. There were equal proportions of males and females, and the median age was 50 years (IQR = 41.70–59.00). Most of the sample (79%) was assessed 3 or more months since injury, with median time since injury being 5.3 months (IQR = 3.22–8.48). There were 72 patients (53%) with employment but not working. More than half of the sample (61%) had two or less comorbidities, and 50% reported no previous musculoskeletal surgeries. History of depression was present in 12% of workers, and anxiety in 6%.
Demographics Breakdown
REMOTE ASSESSMENT CHARACTERISTICS
Two assessment sites used RPR technology (63 cases, 46%), and the third site used Zoom for Healthcare software 39 (73 cases, 54%). RPR allowed remote auscultation, in the rural locations where a physician was not available in person. Table 3 shows remote assessment characteristic variables. We found that 11% of patients lived closer to an urban in-person assessment team (but still went to a rural virtual assessment). These patients lost a median of 87.06 min (IQR = −48.57 to −138.72), whereas 89% saved a median of 161.28 min (IQR = 107.76–225.24).
Remote Assessment Characteristics Breakdown
The median multidisciplinary assessment duration was 275 min (IQR = 250–295). Figure 1 shows multidisciplinary team composition. Typically, there were two to three health care providers using RPR or telehealth per assessment. Assessment time per team member was a median of 72.50 min (IQR = 68.75–75).
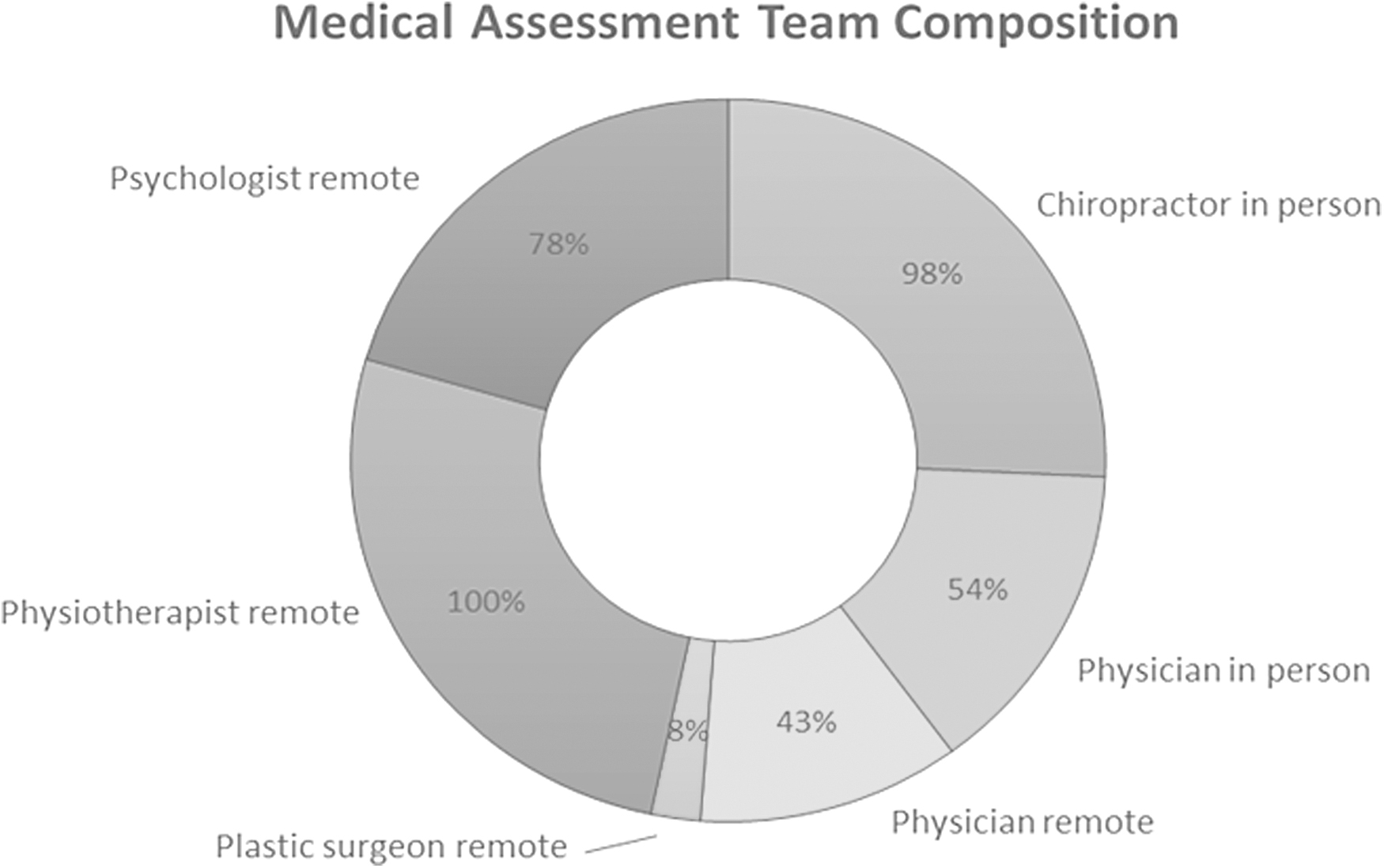
Medical assessment team composition, described as a percentage of total initial assessment where the health care provider was either in person or through remote assistance.
ASSESSMENT FINDINGS
As shown in Table 4, injuries to the back or shoulder accounted for 74% of patients. Both depression (15%) and anxiety (15%) were identified in the sample at time of assessment by the psychologist team member. In terms of disability risk stratification, 78% of the sample were ranked as “medium” or less. The Neck Disability Index was used on 23% of the sample, with patients scoring a median of 15.00 (IQR = 10.00–22.00), which is a moderate disability ranking.
Assessment Findings
IQR, interquartile range.
PROPOSED TREATMENT
Assessment recommendations are found in Table 5. Tertiary care (daily, comprehensive multidisciplinary treatment) was recommended for 76% of workers. Eight or more weeks of treatment was recommended for 87%, exercise therapy for 98%, and education for 99%. A recommendation for early TRTW planning occurred for 84% of patients, with 97% of all patients progressing into a GRTW recommendation.
Assessment Recommendations
Of the remaining 3% (four injured workers), three workers were already working full time, and the fourth worker was not employer attached. When initiating early RTW recommendations, 82% began within the sedentary DOT in a part-time capacity concurrent with treatment. Their functional hours and duties would then be subsequently progressed through combined RTW and comprehensive multidisciplinary in-person treatment programming. Permanent disability related to preinjury occupation was anticipated in 37% of patients.
DOT CHANGES: PREINJURY TO EXPECTED OUTCOMES
Figure 2 identifies DOT levels for this injured worker population. The work time component of the DOT (part-time or full time) was consistently underreported for any of the three measures (preinjury, current status, and expected DOT with treatment). Both the preinjury DOT and the expected DOT with treatment were similar for lifting loads in the “medium” category (51% for preinjury DOT, 58% for expected DOT with treatment). This indicates that with treatment, the patients were expected to return to this functional lifting load. Most patients (82%) were expected to transition back to work in a part-time capacity (if they had not already started), with 54% of cases starting with lifting loads in the “sedentary” or “sub-sedentary” categories.
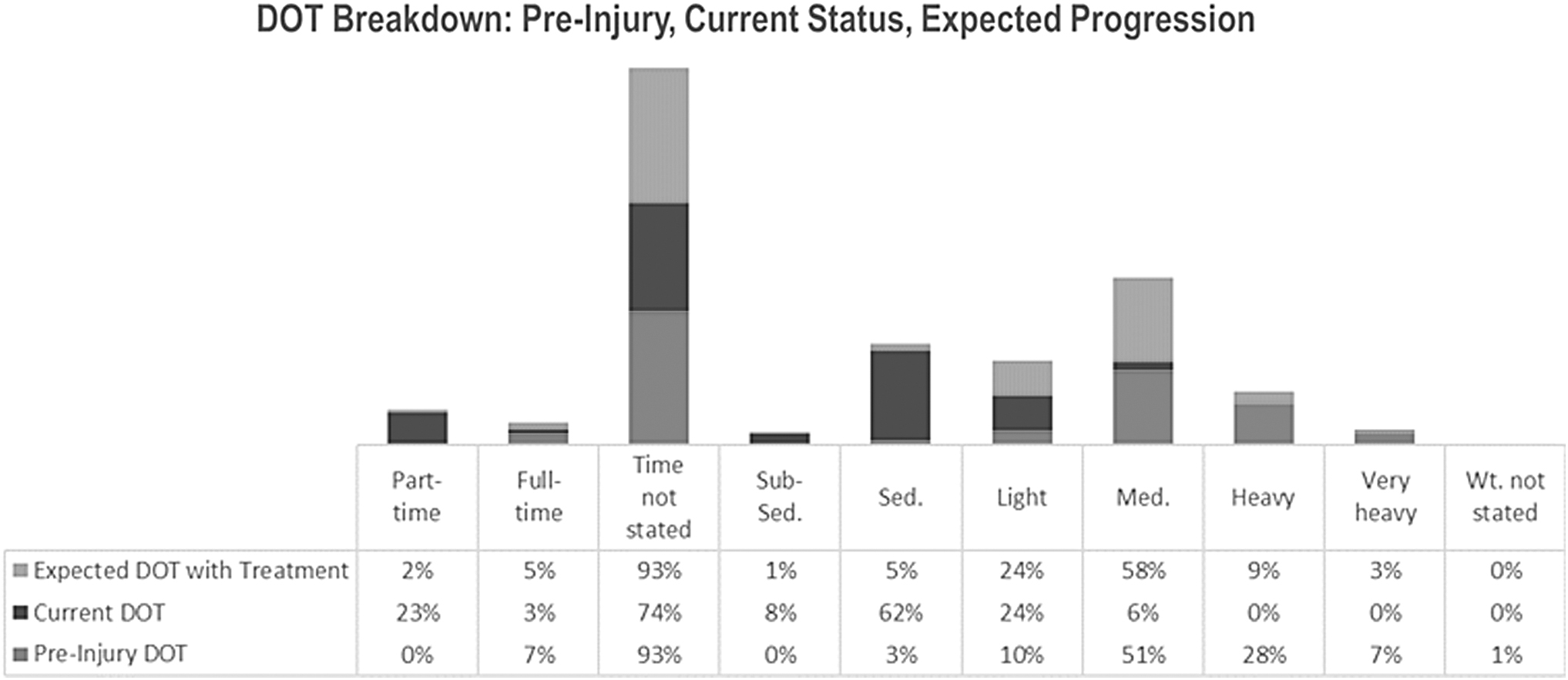
DOT of participants for preinjury, current status, and expected progression. DOT, Dictionary of Occupational Titles; Med., medium; Sed., sedentary; Wt., weight.
Discussion
Rural residents face health care access disparities 15 –17 including access to rehabilitation and specialized health practitioners following a work injury. If a rural resident cannot access care provisions in a reasonable time, clinical and economic outcomes will worsen. 8 This project provided insight on the use of virtual technologies to unite multidisciplinary teams for comprehensive assessment of work-related injuries. Numerous specialized practitioners were coordinated for complex assessments in rural locations using RPR and Zoom for Healthcare. Patient demographics, assessment findings, team composition, management recommendations, and travel implications were described. To the best of our knowledge, this research complements previously published data by Gross et al. 11 and adds information on team compensation and potential travel savings.
The injured workers in this sample were from rural (65%) or urban (32%) locations and had a rural multidisciplinary assessment for musculoskeletal conditions assisted by RPR or telehealth. The majority had chronic injuries, and 60% were not working at time of assessment. These findings are comparable to a recent large-scale study in the Canadian Province of Alberta. 7 Moreover, it was interesting to note that through the use of virtual assessments, 82% of patients had a recommendation for early TRTW during their comprehensive multidisciplinary programming. This highlights the care team's ability to assess and accurately recommend a patient to start work in some functional capacity at the onset of, or early in their rehabilitation.
The TRTW was in a part-time capacity with initial lifting loads recommended, and an expectation that most would return to their preinjury lifting loads following recommended treatment. As a reminder, 97% of cases had an overarching GRTW plan. Of the remaining 3% (four injured workers), three workers were already working full time, and the fourth worker was not employer attached. In this case, a worker would be assessed at the end of the recommended treatment programming and would need to progress into vocational retraining.
Another interesting finding was that 30% of the patients had depression or anxiety at the time of assessment, with only 18% of cases having a documented history of anxiety or depression. Possible explanations for this difference could include lack of formal diagnosis in some patients before being evaluated by a psychologist for their injured worker assessment, or perhaps a recent development of anxiety or depression occurred. Previous research indicates that rural citizens have higher rates of depression when compared with urban dwellers, and this can influence the RTW process, 18,50 so a finding of 30%, although high, is not unexpected. The importance of early access to psychology in this case cannot be understated.
This study appears to be the first to identify travel implications for workers who accessed virtual multidisciplinary assessments in rural locations. Surprisingly, 11% of the workers (n = 14) lost time to travel (i.e., they traveled farther for the virtual assessment in a rural location than a potential in-person urban assessment). It is possible that these cases may have traveled farther to access an earlier assessment team review as opposed to waiting for a later assessment time that would have been located closer to the injured worker.
One of the strengths of this study was that all data collection was done by one author to limit biases. An additional strength is consistency in assessment team members throughout the cohort. A weakness is that the novelty of this area of research means that few “gold standard” protocols for data extraction exist.
Conclusions
This novel research investigated the use of virtual technologies including RPR and telehealth to join an urban multidisciplinary team with a rural in-person team member or members (where available) and injured workers to evaluate complex musculoskeletal injuries and provide recommendations for management. We demonstrated that virtual care facilitated health care access to skilled multidisciplinary assessment teams for injured workers in rural areas and enabled complex treatment planning recommendations to be made.
We introduced preliminary evidence suggesting travel savings in this sample, or the potential for an earlier assessment for injured workers. Future research should compare this model of assessment with a fully in-person assessment to determine differences and similarities in assessment findings, recommendations, and costs incurred. Further investigation should also include evaluation of patient and provider experience with virtual assessment for chronic musculoskeletal injury assessment by a multidisciplinary team.
Footnotes
Authors' Contributions
S.A.B. was responsible for the data collection, statistical analyses, and article drafting. B.B. was a research methodology and statistical consultant on this project and reviewed article drafts. C.W. was the physiotherapist owner-operator for the rehabilitation clinic where the virtual consult records were kept and completed all assessments and written reports and assisted with early design and final article review. I.M. assisted with RPR management, research methodology, and article review. R.J. contributed to research methodology and article review. S.L. was the primary investigator for this project and was responsible the research design, team coordination, and general oversight of each phase of this project including data collection and article writing.
Acknowledgments
The authors would like to acknowledge the Department of Surgery and Virtual Care and Robotics Program at the University of Saskatchewan, Saskatoon, Canada, for the use of the Xpress V2 Remote Presence Robot in two locations for multidisciplinary assessment.
Disclosure Statement
No author reports any conflict of interest.
Funding Information
This project was internally funded for graduate student research work through the University of Saskatchewan College of Medicine's Department of Surgery, and the School of Rehabilitation Science.