
Abstract
Introduction:
Telepharmacy is widely known as the delivery of pharmacy care offered by registered pharmacists and pharmacies using telecommunication technologies to patients at a distance. We conducted a systematic review of the reported usages, benefits, and limitations of telepharmacy models worldwide to further clarify the pros and cons of a telepharmacy model.
Methods:
A total of 39 relevant articles was included after searching for articles with a fixed term on four databases, including PubMed, Virtual Health Library (VHL), Global Health Library (GHL), and Google Scholar, as of April 2021.
Results:
Our review suggested that telepharmacy has played an essential role in addressing pharmacist shortages and helping patients both safely and effectively administer medications in underserved areas. During the COVID-19 pandemic, remote dispensing and counseling are effective measures to avoid infection.
Conclusion:
Telepharmacy could potentially replace or complement pharmaceutical-related activities, facilitating future innovation in the health care industry.
Introduction
The application of information and communication technology can open new prospects in providing telemedicine services to help reduce the burden of the health sector. Telemedicine deals with many spheres of health care, consisting of telepharmacy. Telepharmacy is well known for the delivery of pharmaceutical-related services by registered pharmacists and pharmacies using telecommunications technology to patients at a distance. 1 Some telepharmacy services include clinical pharmacy services, patient consultation and monitoring, drug selection counseling, prescription check, dispensing, and intravenous drug preparation. 1,2
Telepharmacy has been seen as a potential alternative method in drug-related problem assessment for hospitals, pharmacy care for patients in underserved areas due to economic or geographic problems, and discomposure to risks related to patient data privacy and integrity. 3 We conducted a systematic review of the reported usages, benefits, and limitations of telepharmacy models to further clarify the pros and cons of a telepharmacy model.
Materials and Methods
SEARCH METHODS
The review followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (Supplementary data). 4 We did not register our review on PROSPERO.
We searched with the keyword “telepharmacy” on four databases: PubMed, Virtual Health Library (VHL), Global Health Library (GHL), and Google Scholar. All references of selected studies were used for manual search. The study selection procedure is represented in the PRISMA flow diagram (Fig. 1).
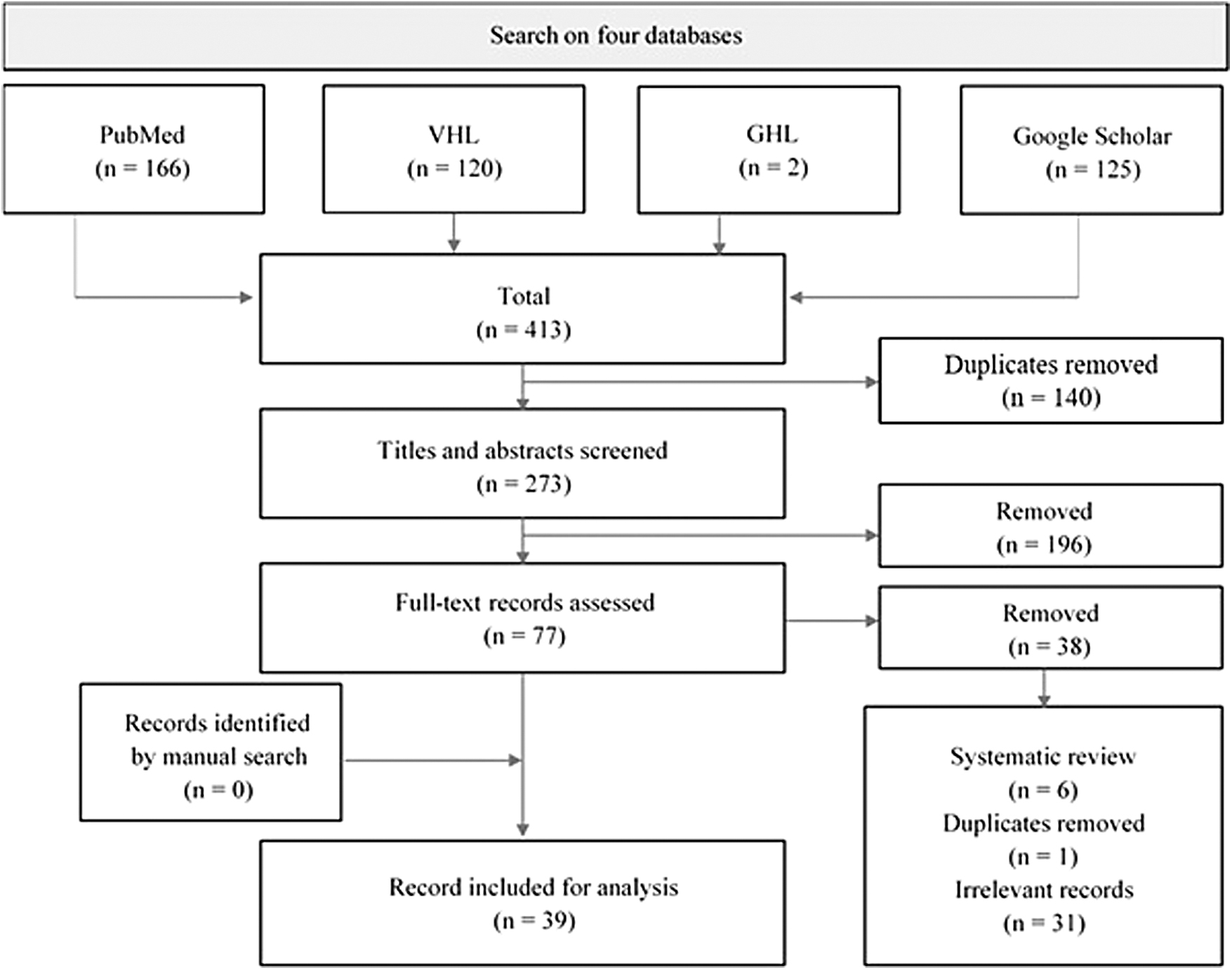
The PRISMA flow diagram of study selection. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
SELECTION CRITERIA
We included all original studies and clinical reports published through April 2021 and selected all articles with reported data on the application, benefits, and limitations of telepharmacy models in health care practice.
We excluded irrelevant articles, which are studies in the field of telepharmacy, but the results do not evaluate the effects on the study subjects' health. Other unreliable sources were also excluded, including book chapters, abstract-only articles, conference reports, reviews, dissertations, posters, discussions, and letters.
RESEARCH SELECTION
We included articles through a two-stage process: first screening the title and abstract, and then scanning the full text. The screened articles were chosen based on inclusion and exclusion criteria; any duplicated articles were excluded. Two independent reviewers independently screened all titles and abstracts. Two senior reviewers independently evaluated the full texts of all included articles. Disagreement was solved by discussion. All relevant articles were used in qualitative data extraction. Data synthesis was conducted following textual descriptions and summarized in a Table 1.
Advantages and Disadvantages of Telepharmacy
ICU, intensive care unit.
DATA EXTRACTION
We extracted data on primary outcomes, including fields of use, benefits, and limitations of telepharmacy models. Secondary outcomes, including requirements for building an effective telepharmacy model and current regulations governing telepharmacy, were also discussed.
Results
A total of 413 articles were found. After the selection process, we used 39 articles for data extraction, all of which were written in English (Fig. 1).
Thirty-nine selected articles reported the application of telepharmacy in eight countries, including the United States, Canada, Spain, Germany, Denmark, the United Arab Emirates, the Kingdom of Saudi Arabia, and Australia. The application of telepharmacy included three main areas: (1) checking prescriptions and dispensing drugs, (2) clinical pharmacy, and (3) patient consulting and monitoring. In addition, telepharmacy was also applied for aseptic preparation and emergencies (tele-emergency) to a lesser extent (Fig. 2).
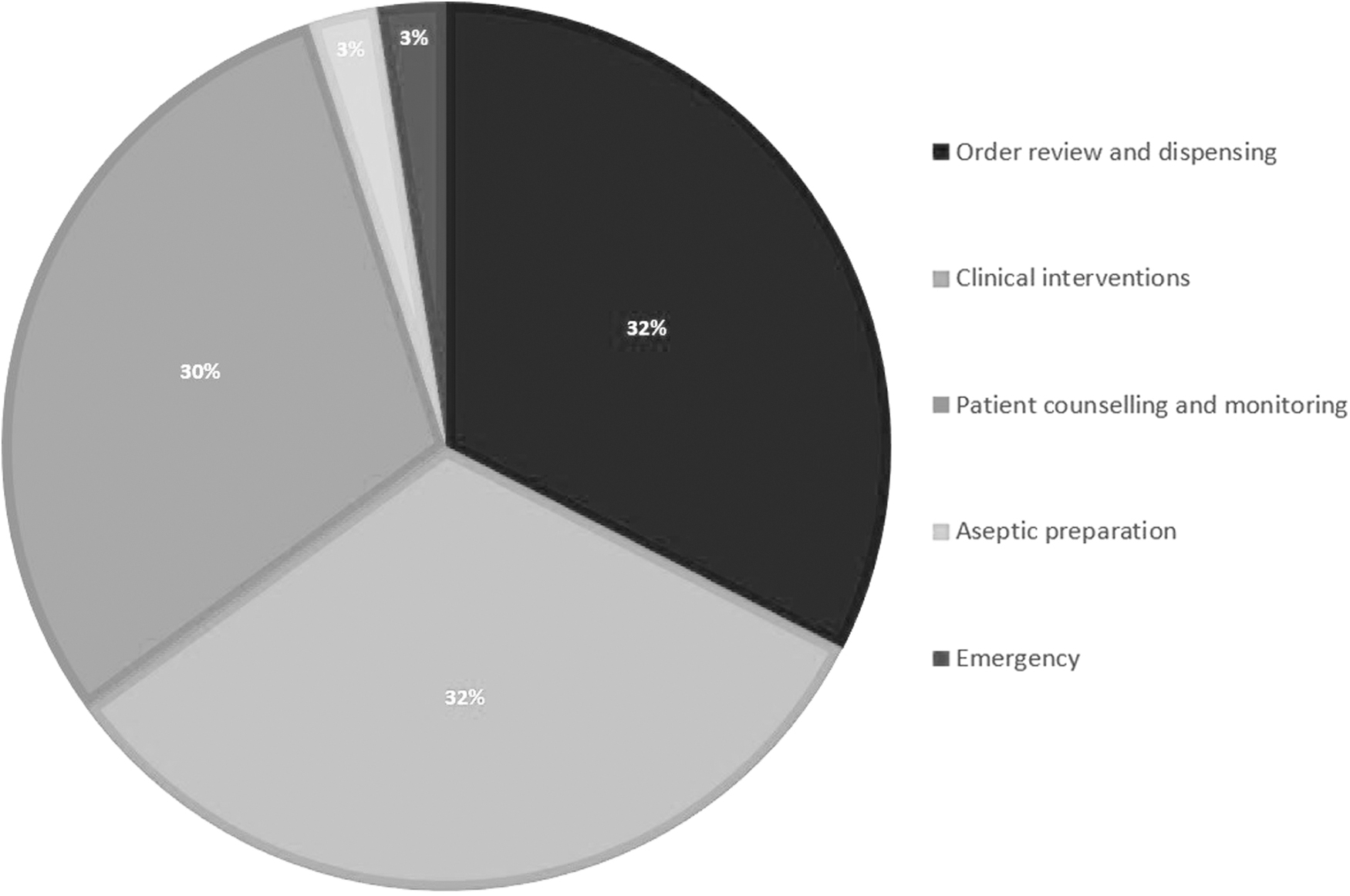
Fields for application of telepharmacy.
Based on the telepharmacy application fields shown in Figure 2, data on the actual advantages and disadvantages of telepharmacy in each area were extracted. The results are shown in Table 1.
The pharmaceutical supply chain is a crucial application of telepharmacy, especially in remote or underserved regions. The models of remote drug distribution by telepharmacy have developed widely in a lot of countries, and several randomized pilot studies have shown that these models work. Telepharmacy helps improve patient medicines availability during hospital night shifts, 5 patients in remote areas, and creates favorable conditions to support remote drug delivery by courier companies. 6 –9 The quality of drug dispensing and medication errors of telepharmacy might be a significant concern to ensure safety and effectiveness.
Many studies have compared the quality between telepharmacy and traditional pharmacies; however, the results were inconsistent. Some suggested amelioration, but others showed no significant differences in drug dispensing safety and efficacy between the two models. 10 –12 For example, in a cross-sectional pilot study by Friesner et al., the error rate in areas using telepharmacy was even higher than that of the control. 13 A greater level of errors reached the patient at the central sites than at the remote sites. 14 However, these error rates were still lower than the average nationally reported. 13,14
Despite the near-average sales growth, telepharmacy models are expected to face the challenge of a lower-than-average inventory turnover ratio. When it comes to a reasonable number of customers, the host should focus on scaling up and expanding the telepharmacy model to be profitable. 15
Consulting and managing patient treatment remotely with telepharmacy is a method to save travel costs 16 and receive higher patient satisfaction. 17 –22 Telepharmacy helped enhance pharmacy service to ensure drug safety and effectiveness for patients and avoid preventable adverse reactions. 23 The management of patients with chronic diseases is one of the most crucial concerns for telepharmacy, 16,24 such as HIV infection, 21 asthma, 17,22,25 diabetes mellitus, 26 and cancer. 18 These models help patients monitor and improve personal clinical indicators, hence improving quality of life. Telepharmacy also allowed to effectively collect medication history to provide adequate medication reconciliation. 27
Clinical pharmacists have an essential role in ensuring safe and effective drug use, providing drug warnings, and improving health care quality. The health system faces a barrier in providing this service in rural or distant places. Telepharmacy helps clinical pharmacists remotely intervene and support hospitals and replace onsite clinical pharmacy services. 18,28,29 Various studies have shown that telepharmacy increases not only the number of clinical warning interventions, 30,31 but also the number of warnings about potential side effects in prescriptions, 23 especially at night, 32 and improves the speed of doctors' prescribing 30 while optimizing cost-effectiveness. 33
A study of efficacy comparison showed no significant differences in the pharmaceutical activity rates in the two models: weekly visits or remotely reviews by pharmacists. 34 In the intensive care unit, telepharmacy is mandatory for providing expert consultations in pharmacovigilance and dose adjustment in special cases. 35,36
In addition, telepharmacy has proven its value in telemedicine for rural locations with limited resources. A case of volatile alcohol (ethylene glycol/methanol) ingestion in a rural critical access hospital, who was cared for by tele-emergency pharmacy and medicine, was described. The patient was diagnosed, and the remote pharmacists calculated the ethanol concentration required to neutralize poison. 37
Another application field for telepharmacy is the isolated inspection of sterile products. A study in the United States demonstrated the accuracy and safety of telepharmacy while checking sterile products, which showed no statistically significant differences in error levels with direct work procedures (p = 0.177). However, the mean time required for direct collecting workflow is significantly lower (p < 0.001); telepharmacy cost savings are estimated at $23,770.08/year. 38
During the COVID-19 pandemic, when infection control requirements are necessary, telepharmacy models have been applied to drug distribution and counseling to foster remote clinical warnings and relieve several burdens in a straightforward manner. This model has shown effectiveness in helping patients access medicine early during home isolation 39,40 and received a high level of patient satisfaction. 40 Comparative studies using parallel drug dispensing by telepharmacy and other distribution methods have shown no difference in drug error rates between the two procedures, 10,11 despite a higher number of patient information errors in the telepharmacy group, which suggested the need for a stricter operational process for telepharmacy. 11
Telepharmacy helps intervene in medication-related problems warnings to patients 41 ; it also addressed concerns and questions related to COVID-19 to provide necessary recommendations. 11
QUALITY ASSESSMENT
The included studies were evaluated for study quality. We used Study Quality Assessment Tools (SQAT) of National Institute of Health 42 to assess the quality of each research method separately, including (1) observation cohort/cross-sectional studies, (2) case-control studies, and (3) case report/case series.
Each item was rated as 1 for good practice or 0 for potential flaws. In addition, if the grading is ambiguous, we followed the guidance of SQAT to place “NA” (not applicable), “NR” (not reported), or “CD” (cannot determine). These categories represent potential flaws that we should be cautious of. The final score would be calculated as a percentage with an equal point for each item. The scoring threshold is those at least 75% to be assessed as “good” quality, those between 75% and 43% as “fair,” and below 43% as “poor” quality. Two reviewers independently extracted the assessment. Discrepancies were resolved by discussion and agreement.
Ten articles were designed as observation cohort and cross-sectional studies (Table 2), 12 articles were case-control studies (Table 3), and 6 were case report/case series (Table 4). Eleven articles were unable to be categorized to apply the SQAT. Those articles carried a high risk of bias. Thus, it should be interpreted with care.
Quality Assessment for Cohort and Cross-Sectional Studies
NA, not applicable.
Quality Assessment of Case-Control Studies
Quality Assessment for Case Report and Case Series Studies
Among 10 observation cohort/cross-sectional studies, the overall rating indicated that none of the studies was of “good” quality. Nine studies were of “fair,” and only one was of “poor” quality. However, none of these studies was excluded from our systematic review. In the case-control group, the overall quality was “fair” in terms of bias, except two studies that were evaluated as “good.” Four out of six case reports/case series had “good” quality, indicating a potentially low bias level.
Discussion
The use of communication and information technology in pharmacy practice has attracted attention in many countries worldwide. The United States has the most experience, with the first telepharmacy service in the early 2000s. 17,22 Telepharmacy is a new approach to providing care from pharmacists in multidisciplinary health care that is becoming more and more popular. 43 Our review shows that telepharmacy has been widely applied in drug dispensing, patient counseling and management, clinical pharmacy, aseptic product preparation, and emergency interventions. Telepharmacy serves as a new ecosystem to communicate with patients or provide online pharmacy support to other health care workers in remote medical facilities. 29,37 The obtained results suggest the importance and enormous potential of the telepharmacy service in the future, which we will discuss next.
First, telepharmacy could be the solution to help reduce the shortage of pharmacists. Patients living in rural or separated areas may have difficulty accessing pharmacy services. 44 The uneven distribution of the industry structure causes a shortage of pharmacist care services in rural or hard-to-access areas, especially clinical pharmacy services. 45,46 A common term for these communities is pharmacy deserts. 47,48 Telepharmacy helps ensure proper pharmaceutical support in underserved areas 6 –9 or facilitates remote pharmacist intervention to support hospitals in providing inpatient clinical pharmacy care. 18,28,29 These technological advancements contribute to reducing inequalities in health care delivery.
Second, telepharmacy can help improve the quality of drug use. The quality of telepharmacy delivery was reported and compared with the control group through the quality-related events (QREs) index. 10 –14 Telepharmacy is generally considered to have no adverse effects on public health, patient safety, and quality of health care, 10 –12 and it is not inferior to pharmacies. 13,14 The Hawthorne effect (i.e., the tendency of some people to work harder and perform better when they are experimental participants) may have become a potential factor influencing the results of the studies.
Long-term studies of the Hawthorne effect will have a less pronounced impact (which cannot be wholly reduced). 49 Further, within 45 months of data collection, the study by Friesner et al. showed a decreasing trend in QRE, which suggested that error rates will decrease as pharmacists and their technicians get used to them. The regulations, protocols, and standards of practice are inherent in the telepharmacy model. 13 In hospitals, telepharmacy has created an environment that facilitates pharmacists to remotely intervene on drug-related issues, 30,31 expand the scope of 24-h hospital pharmacies, 32 help speed up prescription processing, 30 and reduce order processing time, freeing pharmacists for money-saving or quality-improvement initiatives. 33
Remote pharmacist interventions in the telepharmacy service model coordinate patient-centered pharmaceutical care and facilitate the meaningful use of electronic health records. 9
Third, several studies examining the effectiveness of telepharmacy services in the era of COVID-19 have shown that telepharmacy improves drug-dispensing practices, helping to increase a patient's access to pharmaceutical care. 10,11 In response to the health crisis caused by the COVID-19 pandemic, hospitals have adapted their outpatient counseling and dispensing services to telepharmacy to reduce the risk of infection. 39,40 Telepharmacy offers a more comfortable environment for pharmacists to consult with patients without the risk of viral transmission.
Last but not least, education about telapharmacy is essential, not only for pharmacists but also for patients, to reinforce its use. 6 Formal continuing education programs will keep pharmacists up to date with current telepharmacy practices. Today, people need greater access to medicines due to an increased proportion of the aging population and comorbidities, 7,8 leading to a higher need for pharmacists to meet these new needs. 33 However, not all patients have the exact needs. Further action is needed to determine which groups of patients need more intensive pharmaceutical care and, therefore, who can benefit most from telepathy, not just delivery. The goal is to continue to provide high-quality care.
LIMITATIONS
Our review had some limitations. Regardless of following the PRISMA statement, we did not register our review on PROSPERO. We have not yet made a comparison between the telepharmacy model in the studies and each other because of different backgrounds and the miscellaneous type of models when it comes to reality. Also, data on the limitations of telepharmacy were not fully understood. We suggest further clarification of these data in the future.
Conclusions
Telepharmacy has shown certain benefits in providing an alternative solution to the problem of lack of pharmacists and also contributing toward ensuring patient access to medicines in underserved areas. Despite the variation in models and some limitations requiring a higher capacity of the pharmacist in the application of technology and a higher concentration, telepharmacy is effective in providing clinical pharmacovigilance related to drugs and managing patients in treatment, thereby helping to increase the ability to use resources, as well as to save costs.
During the COVID-19 pandemic, some telepharmacy models have been shown to be effective in ensuring drug dispensing, in enhancing drugs' safety and effectiveness, and in coping with the disease in general. These data suggest the potential of telepharmacy to replace or complement pharmaceutical-related activities and facilitate future innovation in the health care industry.
Footnotes
Authors' Contributions
T.V.D. and V.L.T. were responsible for the idea and supervision. All authors did screening and extraction under the supervision of N.T.H. All authors extracted data, and N.T.H. contributed toward interpreting the results. T.V.D., V.L.T., and N.K.Q. took the lead in writing the article. All authors contributed to the article writing and approved the final version.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Ho Chi Minh City Department of Science and Technology (DOST HCMC to Truong Van Dat: under Decision 1362/QD-SKHCN and Grant 99/2020/HD-QPTKHCN).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.