
Abstract
Background:
Infectious disease outbreaks disrupt inpatient clinical care and have an impact on staff and patients' ability to communicate with each other and with the wider community. Digital technology may offer opportunities for communication in the inpatient setting during infectious disease outbreaks.
Aim:
This scoping review aimed to investigate the use of digital technology in the inpatient setting to promote communication in the early stages of an infectious disease outbreak.
Methods:
There were three aspects to this scoping review: (1) a database search of Ovid MEDLINE (MEDLINE), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Association for Computing Machinery Digital Library (ACM) and IEEE Xplore (IEEE) exploring peer-reviewed articles, (2) a gray literature search, and (3) a media search.
Results:
Results focused on the early stages of the COVID-19 pandemic. Thirty-eight peer-reviewed articles were extracted from the database search. There were three main areas of investigation: study characteristics, technology features, and benefits and barriers. Forty-four websites were searched for the gray literature search focusing on policy and guidance. Eighteen media articles were retrieved focusing on patients' use of technology and community involvement.
Conclusion:
Results demonstrate the diverse use of digital technology in the inpatient setting to facilitate communication during the early stages of the COVID-19 pandemic. However, the articles provide limited data to allow readers to fully understand and reproduce described actions. Furthermore, there was limited guidance to support clinicians to communicate using digital technology to create trusting therapeutic relationships. Areas for future development include standard reporting process for technology hardware, software, and content; and structured reporting and evaluation of the implementation of technologies.
Introduction
Identifying new ways to respond to the challenges presented by infectious diseases can revolutionize health care. During the early stages of the COVID-19 pandemic, digital technologies were embraced to facilitate care in many ways, including tracking, screening for infection, contract tracing, quarantine, self-isolation, and clinical management. 1 Specifically, in the inpatient setting, telehealth was used by clinicians to consult with patients where physical attendance on the ward was limited, personal protective equipment (PPE) restricted, or health care workers required to stay home to shield or fulfill childcare responsibilities. 2
One of the key applications of digital technology during the pandemic was to facilitate communication. Digital technology was used by staff to facilitate communication between colleagues, between isolated patients and staff, 3,4 and to facilitate family meetings. 5 For inpatients, digital technologies have offered the possibility to keep in touch with loved ones during difficult circumstances. 6 These practices required extensive changes to practice by patients and health care staff, alongside amendments to infrastructure. In this regard, some existing notable barriers to telehealth, including regulatory, financial, cultural, technological, and workforce, 7 have been partially overcome.
A particular area of interest is the barriers perceived by patients. Before the COVID-19 pandemic, the main obstacles reported by patients to the use of digital technologies for health were acceptance and trust in the technology, and trust in the clinician. 8 –10 While guidelines exist to assist health care workers to transition to the physical and technical aspects of using digital technologies such as telehealth, these guidelines do not address how to engender trust or build relationships using this medium. 11 –14 Consequently, even when health care workers have embraced telehealth as a response to the COVID-19 pandemic, there is the potential that nurturing trusting interpersonal relationships may not be prioritized by health care workers and be secondary to clinical, technological, and privacy concerns.
Research indicates that effective care is centered on quality communication and patient-centered services, with trust at the center of the fundamental care relationship. 15 –17 In their discussion of telehealth during the COVID-19 pandemic, Sansom-Daly and Bradford 18 articulate their concerns about telehealth being insufficient to transmit the “human-ness” necessary to support and facilitate interpersonal interactions. However, others outline how this transition to telehealth offers the possibility to promote “personal empowerment” on the part of the patient 19 and a more “person-centered approach” by the health care professional. 20,21
Considering the rapid changes in practice in response to the COVID-19 pandemic, it is evident that innovative technologies can be used to support care. Consequently, it is imperative that clear and informative information concerning the use and implementation of technologies is disseminated appropriately.
Aim
This review aimed to investigate the use of digital technology in the inpatient setting to promote communication in the early stages of an infectious disease outbreak. The research questions were as follows: - What types of digital technologies are used by staff and patients in hospitals to aid communication during the early stages of an infectious disease outbreak? - What are the perceptions of these digital technologies by patients and staff? - How are digital technologies integrated into clinical care? - What barriers or enablers affect the use of digital technologies during infectious disease outbreaks? - What guidance exists to support the use of digital technologies in clinical care, in the context of an infectious disease outbreak?
Methods
A scoping review was selected as the most appropriate methodology since it explores the breadth of a topic 22 and is known to be helpful where evidence is emerging. 23 For this review, digital technologies were defined as electronic tools, systems, devices, and resources that generate, store, or process data. Examples include mobile phones, tablet devices, computers, social media, video games, and multimedia. In addition, an inpatient was described as a person who is in a hospital to receive treatment. This description includes skilled nursing facilities/intermediate care, which come under a hospital's remit and do not include “hospital at home” or “hospital in the home” or aged care facilities. This scoping review was informed using the Joanna Briggs Institute Scoping Review Framework. 23
INCLUSION AND EXCLUSION CRITERIA
Articles were included if they met the following intentionally broad criteria: described peer-reviewed research of any design; explained the use of digital technology, of any kind, to facilitate interpersonal communication between patients and their health care staff or patients and their relatives or friends; and related to the hospital inpatient setting. Articles were excluded for the following reasons: if they were editorial, opinion, or discussion pieces; gray literature such as scholarly reports, working papers, or government documents, digital technology related to only monitoring patients' condition or administration; protocols or review articles; and those not published in English.
SEARCH STRATEGY
A university research librarian was engaged to assist with the search strategy. Four academic databases were searched: Ovid MEDLINE (MEDLINE), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Association for Computing Machinery Digital Library (ACM), and IEEE Xplore (IEEE).
Search terms related to three distinct areas of interest: the inpatient setting, the presence of infectious disease, and the use of digital technology. These terms were generated with consultation of the wider multidisciplinary research team. Full details of the search terms are outlined in Supplementary File S1. The search was conducted during 1 week of September 2020. The investigation was not restricted by year of publication or via the English language. Articles were only reviewed if the specific search strategy returned them; reference lists were not scanned for further resources, and authors were not contacted to identify the additional source.
The search results were exported into Endnote (version X9.3.3), where duplicates were removed before being imported into Covidence. Reviewers took part in a moderation exercise to ensure consistent application of inclusion and exclusion criteria before the proper review was commenced.
First, titles and abstracts were reviewed. Any discrepancies between the reviewers were resolved by discussion and consensus between the two team members. A third team member was consulted if an agreement could not be reached. Two team members then reviewed full texts, consulting a third team member if an agreement could not be reached. A data extraction template was created in Excel with input from all the reviewing teams.
A second moderation process ensured that all reviewers understood the data extraction template and interpreted and responded uniformly. The data extraction template contained four main areas: basic study characteristics (title, author, year, and country of origin), methodological considerations (study design, aim, clinical location, infectious disease involved, number of cases, and participants involved), technology features (technology use, software used, hardware used, requisite training or other requirements, and safety features), and results (benefits, barriers, participant feedback, and future directions). Given the heterogeneity of study aims, methods, and reporting of findings, data were extracted by two researchers and then themed.
A critical appraisal of included articles was not undertaken, primarily because many articles were written promptly in response to the developing and uncertain COVID-19 pandemic. It was acknowledged that certain knowledge gaps are not amenable to randomized controlled trials and quantification. 24 Consequently, articles that were peer reviewed and were retrospective descriptions of clinical practice, akin to a case study, were included. Cognizant of the fast pace of innovation occurring during the COVID-19 pandemic, alongside this review of academic articles, we also sought a broader perspective exploring gray literature and media articles.
MEDIA SEARCH
An expedited media review was undertaken. This step was necessary to investigate any further aspects of technology use in the inpatient setting that the existing sources may not cover. It involved a search of ProQuest database and Factiva database using the following search terms: (Pandemics OR epidemics OR outbreaks OR “infectious diseases” OR COVID-19 OR SARS OR isolation OR quarantine OR MERS)) AND (Hospital OR Inpatient OR “acute care”)) AND ((All Metadata: Internet OR “smart phone” OR iPad OR “video consult” OR mhealth OR telehealth OR “digital health” OR “digital technolog*”). Results were limited to those in English and published in 2020, which reduced the results sharply.
GRAY LITERATURE ANALYSIS
Websites of health provider organizations, specialist medical colleges, consumer organizations, government agencies, research organizations, and other relevant peak bodies were searched to identify documents that guided health care providers and/or patients on using digital technologies. The research team developed the initial list of organizations, and further resources were identified during the data collection and were subsequently included in the analysis. The search scope was limited to Australian organizations.
The key questions that informed the analysis of documents were as follows:
Type of organization?
Does the organization have a policy/guidance material to support professionals and/or patients communicating during an infectious disease outbreak where social distancing or infection prevention/control is necessary?
Does this policy/guidance material include the use of digital technology to support communication?
Does the policy/guidance material link to training or support for health care professionals or patients to use these technologies?
Does the policy/guidance material refer to creating and sustaining relationships with patients or between patients and their relatives?
Results
The first part of this section presents the findings from the review of academic literature, outlining the scope of key descriptors, reviewing findings regarding the integration of digital technologies into clinical practice, and identifying the benefits and barriers. Thereafter, findings are presented from the media search and gray literature search.
ACADEMIC LITERATURE REVIEW
An outline of the search process is provided in Figure 1.
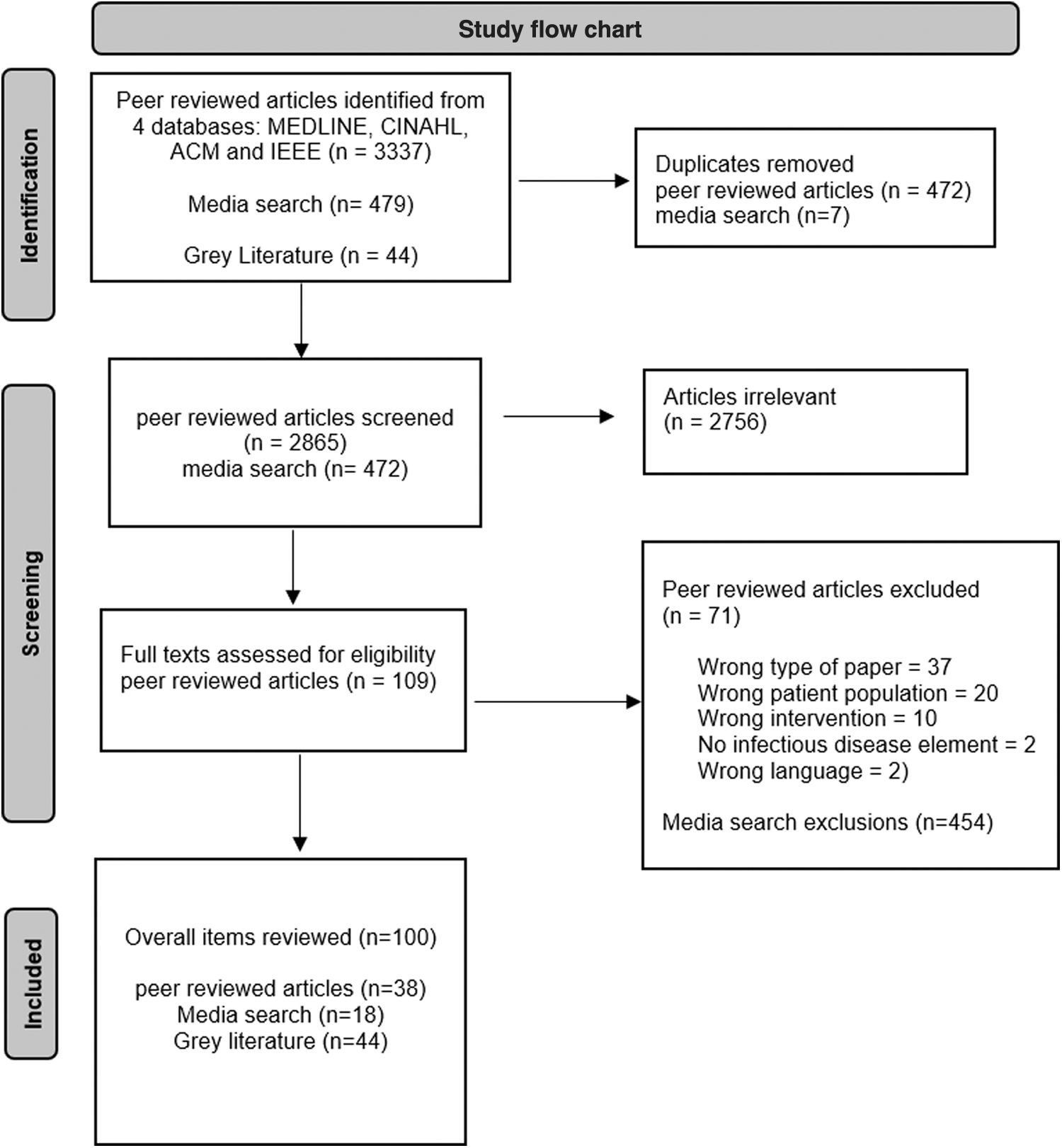
Study flow chart.
Key descriptors
In total, 38 articles were included for full-text review and all studies were published in 2020. Basic details about these articles are outlined in Table 1. Most originated from the United States (n = 28), followed by countries in Europe (Italy n = 2, France n = 2, and Spain n = 1), Asia (Singapore n = 1, Iran n = 1, China n = 1, and India n = 1), and South America (Brazil n = 1). Most articles were retrospective descriptions of clinical practice (n = 27), one included clinical feedback (Hron et al. 36 ), one included an evaluation survey, 45 and one included an evaluation survey and interview. 60
Key Descriptors of the Reviewed Articles
ED, Emergency Department; ICU, intensive care unit.
There were a small number of other types of articles: case studies (n = 4, Bettini, 27 Mohseni et al., 47 Ritchey et al., 3 and Umoren et al. 55 ); letters to the editor (n = 2, Goulabchan et al., 34 Kanellopoulos et al. 39 ); cross-sectional survey (n = 1, Sacco et al. 52 ); cross-sectional interview and survey (n = 1, Valley et al. 56 ); a descriptive retrospective study (n = 1, Lopez-Villegas et al. 44 ); pre–post survey (n = 1, Nardo et al. 48 ); and a retrospective chart review (n = 1, Rosen et al. 51 ). All articles described the clinical practice in response to the COVID-19 pandemic.
The articles described clinical practice in a range of clinical locations. A substantial number (n = 16) related to care provided either exclusively or partially in the emergency department (ED), 25, 28,29,32,35,38,41,43,44,46,47,49,57 –59 including one in pediatric ED. 30 A considerable number of articles (n = 10) described palliative care services, 3,5,27,32,37,38,41,45,53,58 including one specific pediatric palliative care unit. 27 Eight studies described care provided exclusively or partially in intensive care units (ICUs), 31,34,42,49,53,55,56,58 including one specifically located in neonatal/pediatric ICU. 55
A small number of articles (n = 4) described care at more than two locations within the hospital setting. 38,42,57,58 There was one article from each of the following clinical areas: general medicine 26 ; pediatrics 36 ; inpatient mental health 39 ; pharmacy services 40 ; surgical oncology 48 ; inpatient dermatology 50 ; inpatient rehabilitation 51 ; care of the older person 52 ; diabetes 54 ; and psychiatric inpatients and outpatients. 60
Twenty-eight articles described the use of technology as a response to the patient either being diagnosed with or suspected to be infected with COVID-19. 25,26,28,29,31 –37,39,41 –44,46,47,49 –51,54,57 –60 The remaining articles described the use of technology to adhere to restrictions on physical interactions and prevent the transmission of COVID-19 within the broader population. 5,27,30,38,40,45,48,52,55,56
The articles were not always explicit about the hardware and/or software that were used for communication. The vast majority (n = 37) of included articles described the technology-facilitated audio-visual communication. The remaining articles simply used the descriptor “telemedicine,” which was not clearly defined or described (Israilov et al. 38 ). The most used hardware was a tablet used to facilitate communication (n = 27). 3,5,25,26,28,32 –37,39,41,42,45 –47,49,51,53 –60 Of these, 14 articles described using a tablet only. 3,5,26,34 –37,39,41,45,49,50,51,54 Eight studies utilized a tablet and a mobile phone, 28,32,42,46,56,58 –60 and one study used only a mobile phone. 48 A small number of articles (n = 3) outlined the use of a computer, 40,43,44 and seven studies did not provide a specific description of the hardware used. 3,27,29 –31,38,52 Humphreys et al. 37 highlighted that the use of well-known digital technologies is important since they are commercially available, and patients and staff may already have access to them.
In terms of software, a range of different types of videoconferencing software were used, including Zoom (n = 7) 5,27,30,36,37,51,53 ; WhatsApp (n = 4) 45,46,48,49 ; Microsoft Teams (n = 2) 28,35 ; Skype (n = 1) 34 ; and FaceTime (n = 1). 3 Three articles described a combination of multiple videoconferencing software applications including Zoom (n = 3), 33,54,57 while others described different specialized platforms (n = 9), for example, Sickbay, InTouch Health. 25,26,31,40,42,47,50,55,59 Eleven articles did not provide a specific description or adequate details of the software. 29,32,38,39,41,43,44,52,56,58,60
Integration of digital technologies into clinical care
Integration of digital technologies into clinical settings requires that technology is authorized for use by the organization and that staff are competent and confident to use the technology. Discussion of compliance and staff training within the articles is outlined in Tables 2 and 3 , respectively. In terms of compliance, over half of the articles (n = 20) referred to compliance with legal or organizational policies. 3,26,28,30 –33,35 –38,40,41,44,48,50,52,57 –59 Of these, 16 articles referred to alignment of digital technology with national policy or standards for the use of digital technology in health care. 3,26,28,30,31,33,35 –37,40,44,50,52,57 –59 Only Ritchey et al. 3 explicitly referred to compliance with local organizational requirements.
Key Factors Highlighted in the Articles Relating to Safety
Summary of Training Described in the Articles
Some articles referred to specific health care legal requirements being eased in different jurisdictions during the initial stages of the COVID-19 pandemic. In the United States, the Department of Health and Human Services waived sanctions and penalties under the Health Insurance Portability and Accountability Act 1996 (HIPAA) to allow health care organizations to respond efficiently to the COVID-19 pandemic (Department for Health and Human Services of the USA, 2020). One article advocated for legal compliance; however, the wording was unclear whether the specific use of technology discussed was compliant. 32 Lau et al. 41 outlined how legal compliance had been sought by an appropriate body, although no indication of the outcome was provided in the article. In addition, Nardo et al. 48 described the use of compliance in terms of compliance with the software's terms and conditions.
Out of all the articles, a small number of articles (n = 5) explicitly stated their decision to choose a particular technology because of its specific data protection and privacy features. 35,37,43,49,62 Although the motivating factor for using these technologies were linked to the control and prevention of the spread of COVID-19, only one article actively discussed the measures taken to ensure that the technology abided by infection control policies and practices. 5
A large number of articles (n = 26) did not specify whether staff or patients in their organizations required any training to utilize the technology during the infectious disease outbreak. 26,28 –34,36,40 –42,44 –46,48 –50,52,53,55,56,58 –60 Seven articles stated that training was provided internally to staff, a form of peer-to-peer training including training by clinicians, managers, or IT personnel. 25,35,37,38,47,51,57 Two articles described situations where staff received training and were then asked to train colleagues. 5,25 None of the articles described how external staff were required to provide training, although there were two studies where it was unclear whether the training was provided by internal or external trainers. 5,25 Two articles described written instructions on use of the technology that were provided to staff. 35,54
Regarding patients and their families, only three articles referred to training patients or their families on the use of digital technology, 5,27,37 and three articles described providing written instructions to them 35,37,39 although the details of this were unclear. Heslin et al. 35 described providing a video for staff (and possibly patients, although this was unclear) alongside written information and training. Bettini 27 suggested assessing patient/family capacity to use technology and suggested that clinicians can offer some training in advance to patients and families by phone or e-mail. Goulabchan et al. 34 stressed the potential time implications involved when patients require assistance from staff members to talk with their families when using digital technology.
Benefits
Two main themes emerged from the articles: benefits for the organization, including staff members, and benefits for patients and their families. At times, benefits were not clearly stated, and on many occasions, since the articles were written from an organizational or staff perspective, the feedback or opinions of patients and families were not always included. An overview of the main benefits noted in the articles is provided in Table 4. Five articles did not specify the specific benefits of technology use. 33,39,56,58,60
Main Benefits of Using Technology as Outlined in the Articles
PPE, personal protective equipment.
Benefits for the organization including staff
The main benefits stressed by 13 articles were the benefits of technology in reducing the need for PPE. 5,25,28,35,37,42 –44,47,50,54,55,57 Many articles (n = 12) highlighted the role of technology in facilitating the streamlining of clinical services 3,25,28,36,38,44,46,50,51,53,57 and improved services (n = 6). 25,31,32,36,49,50 Two articles referred to reduction in staff workload, 25,31 and three referred to technology facilitating staff member's ability to assist (e.g., removing logistical issues). 37,38,41 While none of the articles conducted included an economic analysis of the use of technology, two gave examples of how inexpensive the technology was for the benefits gained. 28,57
Benefits for the patient and their families
The most frequently reported benefit for patients and their families (n = 13) was the ability to provide a connection between these two groups. 5,25,27,30 –32,34,45,48,49,53,55,56 These included examples relating to the ability of dying patients to say goodbye, family members being informed of the patient's progress, and allowing prayer rituals to continue. Furthermore, 4 additional articles (to the previously mentioned 13) described circumstances where patients had received additional support from staff or volunteers using technology, 32,37,38,41 such as clarifying patients' goals and improving existing care. Only a relatively small number of articles (n = 7) explicitly stated that technology increased the communication between health care staff and patients, 25,31,32,35 –37,40 and of these, just one article went further explaining that technology enabled staff and patients to build a rapport. 36 Notably, very few articles (n = 2) explicitly highlighted patient safety as a benefit. 3,26
Barriers
Table 5 provides full details of the main barriers related to using technology for communication in the inpatient setting. Many of the articles (n = 11) did not specify any barriers associated with using technology in the inpatient setting to promote communication. 29,46,48,49,52 –54,57,58,60,62 The identified barriers correspond to the following four themes: technology, time, resources or infrastructure, and others. Technology issues were identified as the most common barriers. These barriers included technical difficulties (n = 9, 5,28,30,37 Li et al., 42 Lin et al., 43 Rismiller et al., 50 Schoenherr et al., 53 and Wittbold et al. 59 ), including difficulty hearing due to other devices in the ICU or storage issues. Bains et al. 25 described difficulties when the technology was unplugged or moved.
Main Barriers to Using Technology Highlighted in the Articles
A smaller number of articles (n = 6) reported that staff or patients had difficulties using the technology. 27,39,41,42,46,54 This included digital literacy issues, user-friendliness of the technology, and patients' clinical condition. Two articles identified scheduling and coordination as limiting factors, 30,40 while two different articles noted that the use of technology was sometimes time-consuming for the staff. 34,42 Some articles (n = 5) reported staffing issues as a barrier. 31,36,41,49,50 This was not always well defined but did include staff shortages and the ability to engage volunteers.
Resources and infrastructure were significant limiting factors. Wi-Fi issues were specifically highlighted in seven articles, 28,32,37,49,53,54,57 while two articles recounted a lack of sufficient numbers of devices 50,54 and Becker et al. 26 documented patients' recreational use of the technology impacting upon clinical use. Six studies reported a lack of support, 5,35,41,43,46,49 which was not always clearly defined but included lack of technical support and “institutional support.” In two articles, 41,42 there was a direct reference to the lack of appropriate policy to support the use of technology in the desired manner.
Similarly, authors (n = 3) raised concerns about health care staff member's liability for litigation due to using technology in this innovative manner. 33,40,54 Concerns surrounding patient privacy arose in three articles 32,38,42 ; of which two discussed compatibility with HIPAA legislation in the United States. Three articles noted the presence of language barriers, which appeared to be exacerbated using technology. 44,57,59 Despite the evident infection control issues present in these clinical areas, only two articles directly identified cleaning the technology as a barrier. 39,44
MEDIA SEARCH
In total, 204 article titles were reviewed from ProQuest and 259 from Factiva. From these, only six from ProQuest and five from Factiva were deemed relevant to the scoping review aims. In addition, a small number of primary international media websites were searched manually, including BBC, CNN, Fox News, The Guardian, and The New York Times. A total of 16 articles were selected from these sources, of which, upon review, 7 were found to be relevant to the scoping review aims. The results of the 18 media articles are collated in Table 6. The results centered around two major themes as follows: the ability of patients to communicate with their families while in hospital and the positive benefits this brings; and the ability of the community to contribute to communication within the hospital setting by donating digital technology for patient or clinician use.
Types of Organizations Examined in Gray Literature Analysis
NGO, Non Governmental Organization.
GRAY LITERATURE
Websites of 44 organizations were examined, of which the majority were professional bodies, consumer bodies, government agencies, plus various others. Details of organization types and numbers thereof are in Table 7. Of the websites searched and resources identified, generic telehealth information was the most common, with professional bodies as the most common source of information, either in terms of generic telehealth resources, infection control resources, or resources to guide telehealth use in the context of infection control and/or the COVID-19 pandemic. Of the resources relating to telehealth (either generic or about infection control), 18 related to the community context, and 18 were not specific or could apply to either the community or inpatient. Only one resource related mainly to the inpatient setting (but could also be applied to the community context) and concerned palliative care delivery.
Results from the Media Search
In several cases, the guidance related to a specific aspect of telehealth, relevant to the professionals in question. For example, pharmacists conducting medication reviews via telehealth, teleophthalmology, teleradiology, or early, pre-COVID telehealth models through which the patients alongside their General Practitioner (GP) communicated with a specialist in another location. Others related only to communication between health care providers, for example, from radiologists to other medical practitioners. Four organizations included links to telehealth webinars, which were informal information sessions rather than training. Two organizations included online learning modules for health care professionals. Several others encouraged providers to undertake training, but did not provide links or suggestions of where that could be accessed.
Overall, there was limited material that addressed creating and sustaining relationships between telehealth participants. There was minimal guidance on communication and etiquette aspects of telehealth consultations in seven of the documents, such as acknowledging that rapport can be compromised with telehealth, and that video is preferable to telephone, as well as privacy considerations such as establishing who is speaking and present and ensuring that doors are closed. Several offered more guidance in relation to communication aspects, such as “listen actively and demonstrate empathy” and six offered slightly more comprehensive guidance on “patient-centered care” or provider–patient relationships. Across the documents, there was greater emphasis on basic technical requirements, billing rules regarding Medicare Benefits Schedule items, and medicolegal risk management issues such as privacy and documentation.
Discussion
This scoping review has demonstrated how globally digital technology has been used to assist with providing health care in the context of COVID-19 as an emerging infectious disease. This discussion focuses on the following four key areas: (1) the widespread and diverse use of technology to support clinical care in the inpatient setting; (2) lack of detail regarding technology application; (3) integration of technology into care; and (4) recommendations for the structure of future articles on digital technology in the inpatient setting.
THE WIDESPREAD AND DIVERSE USE OF TECHNOLOGY TO SUPPORT CLINICAL CARE IN THE INPATIENT SETTING
It is perhaps predictable that the COVID-19 pandemic dominates the results of this scoping review about technology use in the inpatient setting during the early stages of an infectious disease outbreak. Previously, infectious disease outbreaks occurred more frequently in countries with less wealth and thus access to technology in health care. 61
It was noteworthy that tablets were the most frequently used type of hardware in the articles, and the media search results demonstrated the importance of community donations to help meet the demand. Potentially, the use of “high street” products allows surge capacity during an infectious disease outbreak, in contrast to specialist hardware that may be more difficult to locate and purchase rapidly (this was inferred in one of the articles by Humphreys et al. 37 ). It was also noted that there were cases where tablets were adapted for the clinical environment, for example, tablets attached to intravenous fluid drip stands on wheels, which may reduce costs and increase the ability to redeploy technology after the outbreak has subsided. In addition, the use of widespread commercially available products that individuals may already be familiar with or exposed to may impact usability and training requirements.
There were a vast number of different software programs outlined in the articles. Many of these are commercially available and already in widespread use socially. It has been noted elsewhere that there is a certain degree of unofficial use of technology in the hospital setting by hospital staff often using their own devices (e.g., doctors communicating with each other via WhatsApp and other similar applications 62 ). Perhaps during the COVID-19 pandemic, this “unofficial” use has been condoned and, to a degree, validated.
The use of digital technology in the inpatient setting to promote communication requires an appropriate context and supportive environment. One of the main barriers to technology use in health care is privacy. 63 Several articles referred to the relaxation of HIPAA legislation in the United States and how this facilitated prompt technology use. 33,36 A discussion on the specific legislation and regulatory requirements necessary to facilitate technology use in the inpatient setting is beyond the core aims of this scoping review. However, the articles do note that a flexible environment allows for action in times of need. Recognizing the extraordinary nature of infectious disease outbreaks and their impact on health systems and care provision means that a one-size-fits-all regulation may not be appropriate during a time that demands an urgent but temporary change in practice.
These findings raise a set of questions relevant to the discussion about technology being used innovatively: Who were the agents of change in these situations? Did this originate from the organization and its management structure, or were clinicians or patients the drivers? These questions are outside the scope of this review but are vital to understanding whether health care was catching up on the use of technology elsewhere in the community. To an extent, the use of technology in the inpatient setting is not surprising given the use of technology in modern daily life. However, the difficulty for clinicians is understanding how technology can be used efficiently and sensitively. Herein lies the difficulty. This scoping review has highlighted that the included articles did not provide sufficient details about what technology was used and how (and indeed whether) it was used effectively.
LACK OF DETAIL REGARDING TECHNOLOGY APPLICATION
The descriptive nature of most of the academic literature, rather than traditional prospective research, provided challenges for reviewers. The quality and rigor of the articles were mixed, and many provided only very limited information. It is acknowledged that the emergency experienced at the beginning of the COVID-19 pandemic created pressure to publish and disseminate innovations in practice; however, an essential aspect of publication is to share knowledge and to allow others to replicate clinical practice to obtain similar results. In many cases, the articles did not provide sufficient details to allow the reader to understand clinical practice or attempt to replicate it themselves comprehensively.
There were specific areas where lack of detail was particularly noteworthy. The first was concerning infection control. Limiting the spread of an infectious disease was the primary rationale for using technology in all the articles. However, very few articles described the process for cleaning this equipment. Perhaps this was considered by the authors to be covered by standard practices within the hospital. However, it leaves the reader devoid of information. Potentially it suggests a lack of value attached to cleaning. When there is existing research about technology as a fomite for the transfer of pathogens, 64,65 this lack of detail is concerning.
Second, there was limited information regarding training. For staff and patients to use technology appropriately and efficiently, it is likely that training of some form may be necessary. The analysis of gray literature identified a lack of resources regarding the use of telehealth in the inpatient setting, either generically or in the context of infection control required in an infectious disease pandemic. There is limited understanding of staff and patients' current levels of digital literacy in inpatient settings and thus the starting point for training. Considering the potential for technology to impact time (either staff experiencing time pressures or patients' crucial time and energy), it is important that systems are as user friendly as possible. 66,67 Aspects of the literature did highlight the practice of peer-to-peer training, which could perhaps link to the ability for surge capacity; however, details were scarce.
Third, details concerning barriers were difficult to decipher. Often barriers were described in general terms, which could be interpreted broadly, and there were few descriptions of how these barriers were overcome.
INTEGRATION OF DIGITAL TECHNOLOGY INTO CARE
The articles primarily outlined benefits for health care staff or from an organizational perspective, particularly around PPE use and staff workload. This is unsurprising given the context of the first few months of the COVID-19 pandemic and the worldwide PPE shortages experienced. The considerable benefits to patients communicating with their families were partially demonstrated in the articles, but more clearly in the media search. The importance of this was not quantified; however, should not be undervalued. Further research on patients' and family perspectives of the use of digital technology would help optimize practice.
The literature shows the importance of therapeutic relationships between health care professionals, patients, and their families. 17,68 However, the articles provided little information on how digital technology was integrated into clinical care, including creating and sustaining therapeutic relationships. One aim of our gray literature analysis was to examine the availability of guidance or support for health care professionals to utilize technology in this manner. Our analysis identified limited written guidance or support, which may mean that practice is ad hoc, specific to the individual and focused on task completion rather than on more profound, more trusting relationships. Further exploration of how health care professionals make and sustain therapeutic relationships using digital technology is warranted.
The lack of guidance regarding the inpatient setting may reflect the limited use of digital technology for communication in inpatient settings. At the time of analysis, Australia had not experienced the high rates of COVID-19 incidence and hospitalizations (and deaths) seen in other countries, and so, there may not have been a pressing need for digital communication with inpatients (either with clinicians or with family/friends), and little requirement for health care practice and policy guidance relating to such scenarios. Instead, our research suggests that guidance on technical capability, billing, and medicolegal risk presented more pressing priorities where the need for telehealth services in community settings has surged since the onset of the COVID-19 pandemic.
A limitation of our analysis is that it included only publicly available documents. There may be internal policy, procedure, and guidance documents within public and private hospitals that could not be accessed for this research, which would provide more comprehensive guidance on the use of digital technologies to support communication in inpatient settings.
RECOMMENDATIONS FOR THE STRUCTURE OF FUTURE ARTICLES ON DIGITAL TECHNOLOGY IN THE INPATIENT SETTING
The aim of the scoping review was to investigate the use of digital technology in the inpatient setting to promote communication in the early stages of an infectious disease outbreak. However, the type of articles retrieved and their content created difficulties in fully addressing this issue and suggest that clinicians too would encounter difficulties in applying these results and insights. Overall, there was a lack of specific detail that meant that readers might not have a clear and complete understanding. The authors of this review suggest that a framework for reporting technology use in health care would be helpful in the future.
This scoping review has highlighted that some vital areas were at risk of being underexplored and maybe aspects for inclusion on such a reporting guideline. These aspects include specific hardware, specific software, training needs, compatibility with local and national guidance, infection control requirements, ability to upscale rapidly, clinician experience and feedback, and patient and family experience and feedback. Consideration of these will ensure that when clinicians report experiences of using technology in care for public dissemination, they describe adequately to support successful implementation in other settings.
Conclusion
This scoping review investigated the use of digital technology in the inpatient setting to promote communication in the early stages of an infectious disease outbreak. The results demonstrated that globally staff in different clinical departments utilized technology to communicate with patients and facilitate patient communication with their families. The articles described benefits to health care organizations (mainly in terms of reduced PPE use and staff workload), alongside benefits to patients by having more contact with their family members. Thus, digital technologies appeared to improve the completion of clinical tasks and allow for communication; however, the extent to which they were utilized to create therapeutic professional relationships was difficult to assess and, therefore, an area of interest for future studies.
There were barriers to technology use and enablers; yet the language and details around these areas were not always consistent, making aggregation difficult. The media search reiterated the importance of technology to enhance patient communication with their families and the potential role of the community in contributing to generating solutions at challenging times. The gray literature search demonstrated that even when technology is used in clinical care and within the sights of professional bodies, there was limited guidance to optimize implementation in clinical practice.
Several areas for future research were identified. The most significant of which is the importance of including critical elements within articles published within this field, possibly triggering the generation of reporting guidelines.
Footnotes
Authors' Contributions
All team members were involved in the development of the research questions. A.M., B.L., and R.F. were involved in developing the search terms. A.M., M.T., J.C., R.F., and B.L. led the abstract and full article screening. All team members were involved in data extraction and checking. M.T., S.Y.P., and A.W. led the media search. A.M., B.L., M.T., A.W., and S.Y.P. contributed to the first draft of the article. All authors reviewed and edited the article.
Acknowledgment
The authors thank Josephine McGill at Flinders University Library Services for her assistance with the scoping review search string and her insight into the search strategy.
Disclosure Statement
The authors have no perceived or actual conflicts to disclose related to this research.
Funding Information
The authors would like to acknowledge and thank the Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, for funding this work.
Supplementary Material
Supplementary File S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.