
Abstract
Introduction:
Autonomic dysfunction has been implicated as a consequence of traumatic brain injury (TBI). Heart rate variability (HRV) may be a viable measure of autonomic dysfunction that could enhance rehabilitative interventions for individuals with TBI. This pilot study sought to assess the feasibility and validity of using the Zeriscope™ platform system in a real-world clinical setting to measure HRV in active-duty service members with TBI who were participating in an intensive outpatient program.
Methods:
Twenty-five service members with a history of mild, moderate, or severe TBI were recruited from a military treatment facility. A baseline assessment was conducted in the cardiology clinic where point validity data were obtained by comparing a 5-min recording of a standard 12-lead electrocardiogram (ECG) output against the Zeriscope platform data.
Results:
Compared with the ECG device, the Zeriscope device had a concordance coefficient (rc) of 0.16, falling below the standard deemed to represent acceptable accuracy in HR measurement (i.e., 0.80). Follow-up analyses excluding outliers did not significantly improve the concordance coefficient to an acceptable standard for the total participant sample. System Usability Survey responses showed that participants rated the Zeriscope system as easy to use and something that most people would learn to use quickly.
Conclusions:
This study demonstrated promise in ambulatory HRV measurement in a representative military TBI sample. Future research should include further refinement of such ambulatory devices to meet the specifications required for use in a military active-duty TBI population.
Introduction
According to worldwide data compiled by the Defense Medical Surveillance System (DMSS) and reported out by the Defense Health Agency (DHA) Traumatic Brain Injury Center of Excellence, 1 between 2000 and 2019 there have been recorded 417,593 traumatic brain injuries (TBIs) sustained by U.S. service members. The vast majority of these injuries fall in the mild TBI category (82.4%), with much fewer in the moderate (10.2%), severe (1.0%), and penetrating TBI (1.3%) categories.
Often differentiating civilian versus military-related TBI is the cause of injury, with blast exposure being more common in military service members. 2,3 Another important distinction is the common co-occurrence of mental health disorders such as post-traumatic stress disorder (PTSD) that are associated with military service, particularly if the injury occurred during combat. 4
In fact, Edwards-Stewart et al. found greater-than-additive effects of the interactions between mental health conditions and TBI on health care utilization in the military population. 5 In addition, autonomic dysfunction may be more common in this patient population, as evidence suggests that individuals with mild TBI and co-occurring PTSD and chronic pain have depressed heart rate variability (HRV). 6
It has long been clinically understood that abnormalities in the balance between sympathetic and parasympathetic nervous system responses are seen in military service members as far back as World War I. Fraser and Wilson described in 1918 7 the “irritable heart of soldiers” as consisting of dysregulated cardiovascular responses such as “…increased pulse rate, shortness of breath, palpitations, precordial pain, and dizziness…” (p. 27). Sometimes referred to as “soldier's heart,” these problems date back to Jacob Da Costa's 1871 description of this condition in Civil War soldiers. See Kuijpers 8 for a brief historical review of the concept of soldier's heart, and therefore, it is not surprising that HRV has been seen as an important characteristic of military-related TBIs and other co-occurring conditions.
Much of the symptomatology in TBI may be attributed to the dysfunction in the autonomic nervous system (ANS). In a systematic review by Pertab et al., 9 it was found that concussions are frequently associated with ANS abnormalities. Thus, ANS abnormalities may be common among those who experience concussion and co-occurring medical conditions, the latter of which may also be associated with such abnormalities. In the context of military TBI, Pyne et al. demonstrated that predeployment measurement of HRV (in this case, high-power frequency [HF]) interacted with the PTSD Checklist–Military Version (PCL) in Army National Guard service members in predicting postdeployment symptom scores on the PCL. 10
In a large cohort of active-duty Marines (N = 2,430), after controlling for the presence of TBI and depression symptoms, lower levels of HF were associated with a diagnosis of PTSD. 11 The investigators of this study concluded that predeployment HRV measurement may be beneficial in predicting risk and resilience for mental health and physical consequences of combat exposure.
We postulated that “real-time” ANS assessment by continuous HRV monitoring may be a valuable component in the treatment of individuals with TBI to assess and enhance response to therapy. Furthermore, by providing HRV biofeedback to patients, they may be able to modulate their own HR and ultimately improve their physical and psychological well-being. This was supported by prior published studies, including a systematic review by Morgan and Mora, 12 who found that HRV biofeedback was both a safe and effective method for guiding improvements in sports performance.
Given the multifaceted and sometimes “invisible” nature of TBI symptomology, there is a need to develop and implement more objective and quantifiable physiological measures that are cost-effective, portable, and easily deployable in clinical settings. One such device that shows promise for the measurement of HRV is the Zeriscope™ platform, which was developed as a collaboration between Zeriscope, Inc., the Medical University of South Carolina (MUSC), and the Ralph H. Johnson VA Medical Center in Charleston, SC.
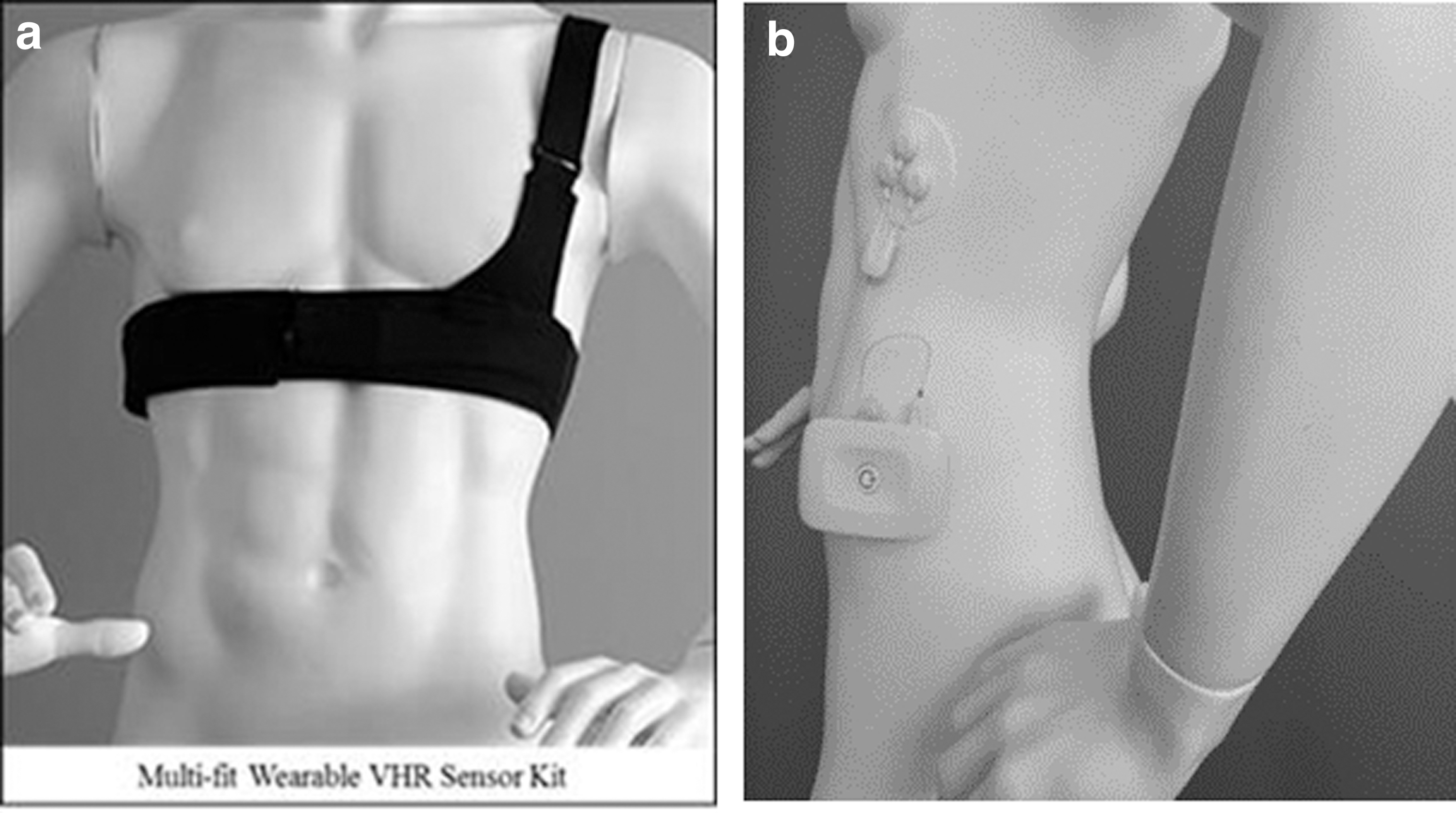
The Zeriscope platform was designed to be a means of obtaining ambulatory human physiological data that could be deployed in a telehealth environment, including service members in an austere environment. In the current application, the platform was developed to record HRV data in a wearable device to be utilized in a TBI treatment clinic (Fig. 1).
The primary objective of the current study was to evaluate the feasibility of introducing a wearable system within a military TBI clinical setting, utilizing the Zeriscope platform to measure consistent and reliable data readings of HRV in an effort to provide meaningful physiological biofeedback to patients and assess response to therapy.
Methods
PARTICIPANTS
Active-duty service members who were participating in an interdisciplinary intensive outpatient program (IOP) at a military treatment facility for postacute rehabilitation of TBI and associated common comorbid conditions were eligible for enrollment. The IOP is a 5-week, 5-day/week, 8-h/day program for those who had sustained TBI and co-occurring conditions, such as PTSD, chronic musculoskeletal pain, and/or chronic headaches. Participants were recruited from the program between June 2018 and January 2020.
The composition of the military service members who participated in this study is summarized in Table 1. Those who were screened (N = 25) were predominantly male (92%), married (92%), enlisted (88%), served in the army (80%) and were between the ages of 23 and 48. All but one participant had been deployed to a combat environment, with the average number of deployments across all participants being three.
Summary of Participant Demographics
SD, standard deviation.
The most recent TBI reported by participants, fell into the categories of closed head injury (44%), blast exposure injury (48%), penetrating head injury (4%), or crushing head injury (4%). The TBI severity was predominantly mild (80%), with mixed symptoms of loss of consciousness (52%), presence of post-traumatic amnesia (40%), and alteration of consciousness (96%). Of the 25 enrolled participants, 3 dropped out before baseline testing. Two additional participants were unable to complete validation testing for both devices at baseline (Table 1).
STUDY METHODOLOGY
The study obtained approval through the Regional Health Command–Pacific Region/Madigan Army Medical Center Institutional Review Board. To check the validity of the Zeriscope against the standard, at the baseline assessment, trained staff within the cardiology clinic placed a 3-channel Holter monitor (SEER Light) to obtain a standard-of-care electrocardiogram (ECG), and the Zeriscope device on each participant.
Heart rate data from both devices were captured concurrently and measured for at least 5 min while participants remained in a seated position with limited movement and normal breathing. Because recordings on the ECG monitor had an idle state that would be on but not always collecting data, the recordings were extended for 15 min. Since the ECG monitor was connected and idle for a variable amount of time before capturing data, the data could not be synced at the beginning of either recording. The last 5 min of the ECG recordings were selected for use as a known time point. Time-stamped raw device data were captured and extracted from the ECG Holter monitor and Zeriscope devices.
To assess the feasibility of utilizing the Zeriscope device in a clinical setting, participants were asked to wear the device during one yoga session per week, ∼1 h for each session during the 5-week IOP. Each yoga session was led by a certified yoga instructor. An ECG signal was taken by the Zeriscope device ∼5 min before and 5 min after each yoga group session while in a seated position. Continuous measurement of heart rate data was captured during each yoga session.
Upon completion of the program, participants were then asked to complete the System Usability Scale (SUS) 13 to assess their satisfaction and perceptions of the wearable device.
STATISTICAL METHODS
To understand the correspondence between Zeriscope-obtained HRV and standard ECG monitoring data, the following statistical approaches were used.
Instantaneous heart rate calculation
The Pan and Tompkins algorithm 14 was used by the Zeriscope to calculate the elapsed time for each heartbeat. The RR interval (or R wave to R wave time interval) is calculated as the difference in elapsed time between each beat. Instantaneous heart rate (IHR) is then calculated as the RR interval divided into 60.
Paired differences
The commonality between recordings on the two devices is the endpoint, and so, IHR data were joined pairwise starting at the end of the Zeriscope recordings, with leftover unpaired IHR data from the Zeriscope device (IHRdevice) discarded from the analysis. Using the ECG-determined HR (IHRecg) as the standard, each of the HR monitoring systems was assessed for accuracy by calculating the difference between the measures and comparing. The paired differences were calculated as (IHRecg − IHRdevice) for each device under the various conditions. Absolute values of the paired differences were also summarized to better assess the magnitude of difference irrespective of direction. Percent differences were calculated as [(IHRecg − IHRdevice)/IHRecg] × 100.
Agreement
The Bland/Altman analysis was performed to assess agreement for each device with ECG. In addition, Lin's concordance correlation coefficients (rc) and the associated 95% confidence intervals were calculated to provide a measure of agreement for each device with ECG. The concordance correlation coefficient (rc) measures the degree to which the paired observations fall on the identity line. An rc > 0.8 was deemed to represent acceptable accuracy in HR measurement. 15
Results
Out of 6,546 paired HR measurements, 6,534 were recorded (99.8%). Missing data were attributed to the failure of the ECG monitor to record HR for only one participant. Measured HR for the ECG monitor ranged from 49 to 187 beats per minute (bpm; mean 74.9 ± 12.1). Measured HR for the Zeriscope device ranged from 3 to 298 bpm (mean 79.8 ± 30.7). Participants with a maximum above 200 bpm were considered outliers as denoted in Table 2. The average absolute difference from the ECG monitor was 3.7 bpm.
Individual Participant Instantaneous Heart Rate Findings
N = 20 with complete data.
Asterisks (*) denote maximum instantaneous heart rates exceeding 200 bpm, the determined threshold to assist in determining outliers.
ECG, electrocardiogram.
The Bland/Altman analysis was performed and data were plotted to assess agreement against the mean values (Fig. 2). The rationale for plotting the data was to uncover any tendency for the variation to change with the magnitude of the measurement. Results suggest that large differences were not linked to specific HR values, meaning that variability was not linked to HR magnitude. Here, 95% of differences between the Zeriscope and standard ECG fell between −62 and +56 bpm.
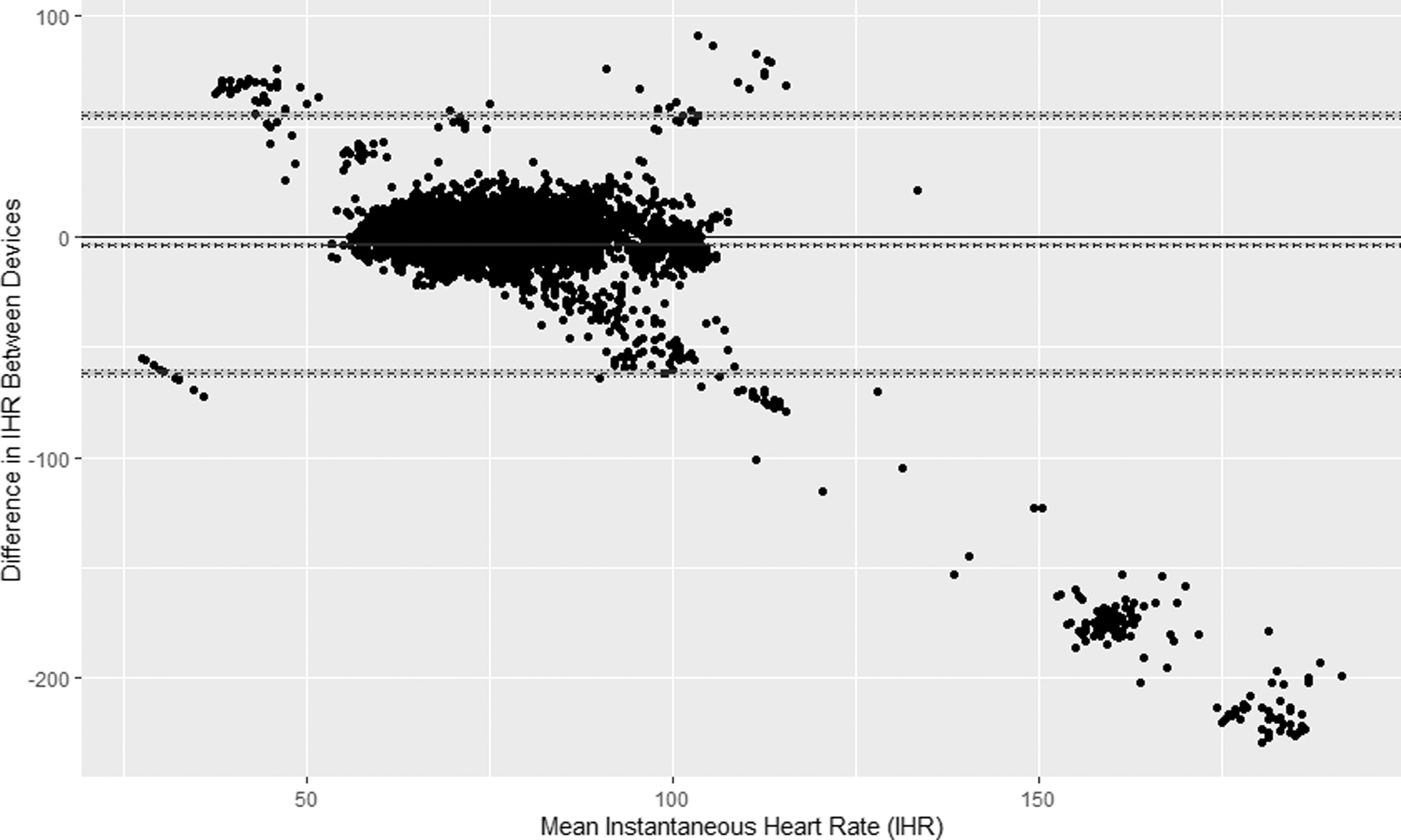
Bland/Altman plot for heart rate comparison between standard ECG- and Zeriscope-acquired data. ECG, electrocardiogram.
When compared with the standard ECG Holter monitor, the Zeriscope device had a concordance correlation coefficient (rc) of 0.16, below the 0.8 standard deemed to represent acceptable accuracy in HR measurement. Figure 3 shows the IHR and ECG heart rate measurements plotted with a 45° line representing perfect equivalence between the two devices. Visual inspection of this figure shows a substantial number of outliers near the top of the chart with heart rate readings on the Zeriscope device between 200 and 300, much higher than their paired heart rate from the ECG monitor.
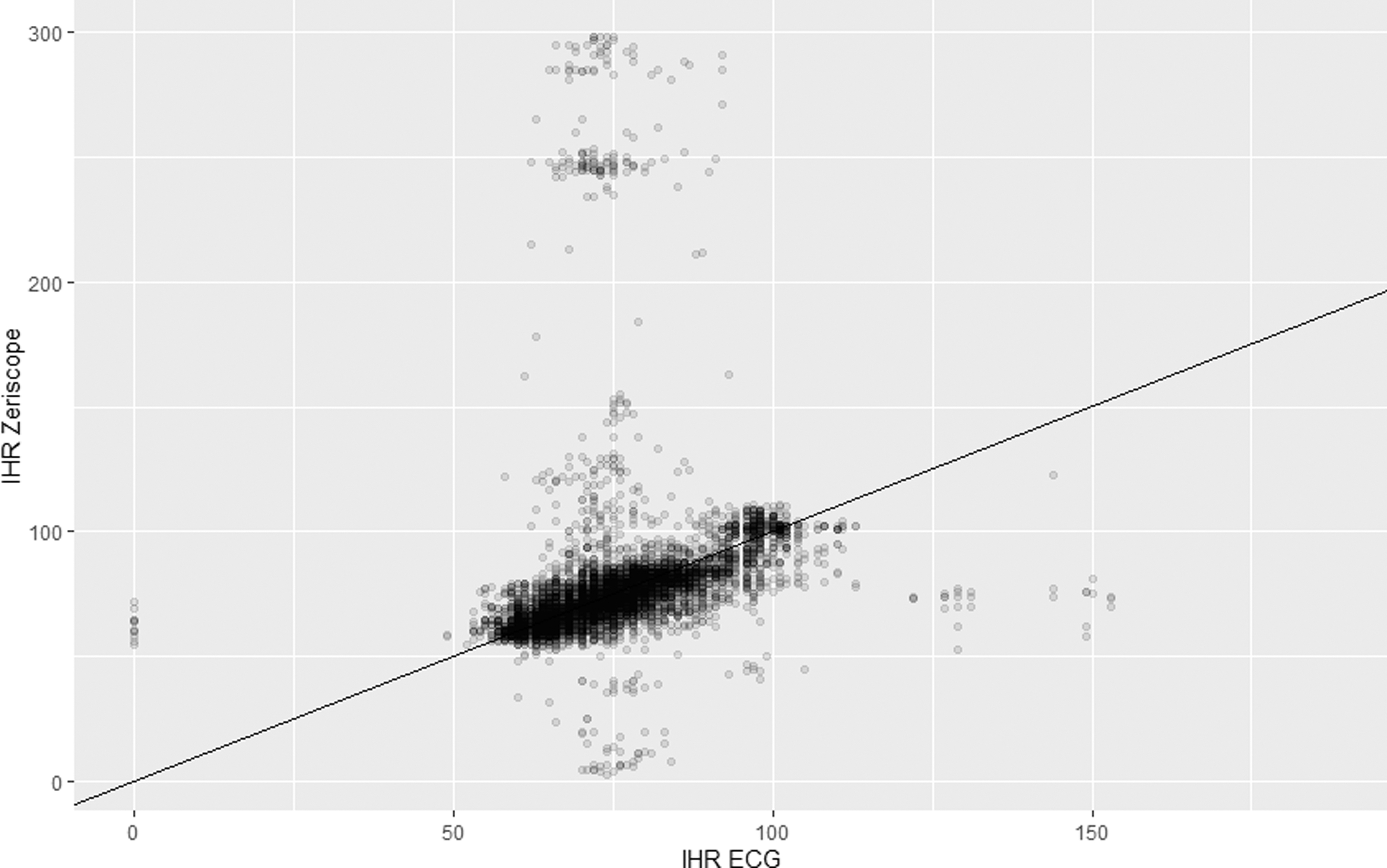
Comparison of standard ECG data- versus Zeriscope-acquired IHR with 45° line reference. IHR, instantaneous heart rate.
OUTLIER ANALYSIS
To understand whether or not specific outliers contributed to the lowered concordance rate, we conducted a subanalysis to investigate individual high IHR readings. We wished to understand if outliers were distributed across all participants or were isolated to a few participants. Using a maximum of 200 bpm as a reasonable threshold to identify outliers, we found five participants' Zeriscope data that met this threshold in Table 2 corresponding to five participant ID numbers 3, 6, 13, 14, and 25.
We then examined each of the individual plot points for these five participants (Fig. 3). The overwhelming majority of the heart rate measurements exceeding the 200 bpm threshold are isolated to one participant, participant ID number 14. Excluding this participant from the sample, the concordance correlation coefficient (rc) improved from 0.16 to 0.50, yet continuing to fall below the desired 0.8 standard of acceptable accuracy.
SYSTEM USABILITY SURVEY
Participant responses to the SUS are shown in Figure 4 in the order of strength of agreement with each item. Positively worded questions (1, 3, 5, 7, 9) scored at very high levels of agreement. Negatively worded questions (2, 4, 6, 8, 10) scored at very low levels of agreement. These finding suggest that from a usability standpoint, the Zeriscope device is fairly easily incorporated into the clinical environment and is associated with a reasonable level of effort to set up, record, and capture data. In addition, responses suggest that participants were favorable toward the idea of receiving greater objective physiological measures when receiving treatment.
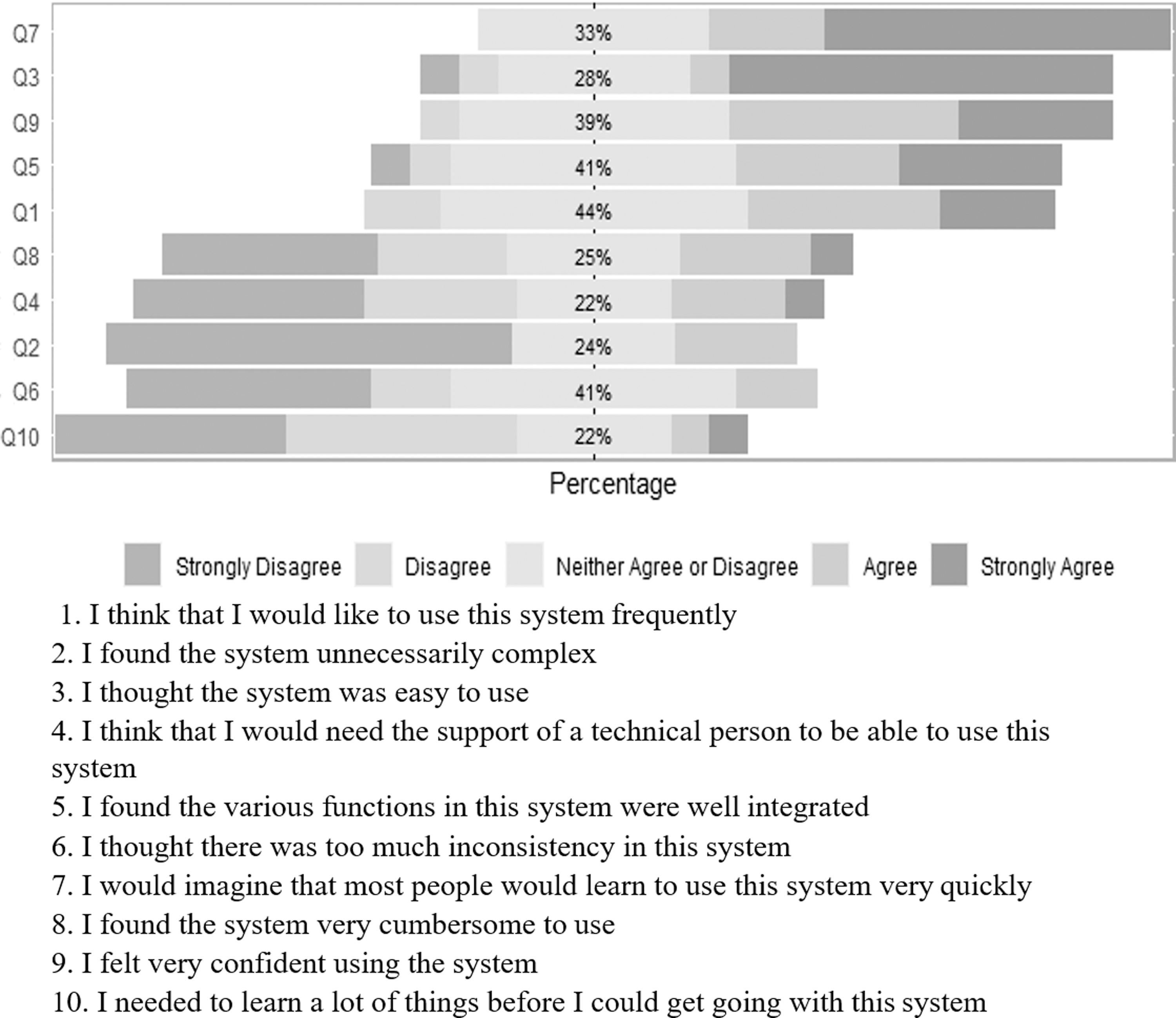
Item content and results of the SUS. SUS, System Usability Scale.
Discussion
Previous reports consistently demonstrate an association between ANS dysfunction, as measured by HRV, and the diagnosis of PTSD and TBI in military populations. 16,17 Moreover, the effects on the ANS may be even further magnified if these diagnoses (i.e., TBI and PTSD) coexist in the same individual, which is often the case for military service members, especially those with combat-related injuries. 18
Further evidence to support a strong association between HRV and PTSD are published reports that demonstrate that individuals with lower HRV are likely at a greater risk of developing PTSD. 19 Therefore, the implications of ANS dysfunction, as manifested by changes in HRV, for injured service members with commonly occurring conditions such as TBI and PTSD, compel military clinicians and researchers to identify practical methods for accurately measuring and monitoring HRV in patients. Such devices could be of meaningful clinical utility to help identify individuals at risk for PTSD, help further classify different phenotypes of PTSD and TBI, as well as to better measure patient responses to therapeutic interventions.
The Zeriscope platform was designed to be used as a wearable device to obtaining HRV data in an ambulatory and remote environment for such purposes.
This study sought to obtain validity evidence and test the feasibility of implementing the Zeriscope device to measure HRV in an ambulatory clinical setting for patients with TBI and PTSD. Our results suggest that the system currently falls short of reaching an acceptable level of accuracy when compared with a standard ECG Holter monitor for injured service members in interdisciplinary care for TBI. Therefore, further refinements may be necessary to uniformly obtain accurate data capture on the Zeriscope platform at a level commensurate with what can be obtained using a standard ECG Holter monitor. Doing so would allow for ambulatory recording and transfer of HRV data in settings outside of a cardiology clinic and thus being a platform that is adaptable for use in an array of clinical settings or other military environments.
The findings of this study, however, do demonstrate the user acceptability of wearing a device during clinical treatment sessions as a means of objectively monitoring physiological data, such as HRV.
This study is the first of its kind to implement the use of a wearable device to measure more than 6,500 HRs during the clinical care of U.S. Service Members with TBI/PTSD. Despite this, there were a number of shortcomings of the study and lessons learned for further research. During the study, there were incidents when the Zeriscope devices were disconnected from participants at different times than the ECG monitor, resulting in the misalignment of paired HR data. This underscores the necessity to have precise and reliable placement of ECG electrodes in synchrony between monitoring platforms to ensure accurate comparison of continuous ECG monitoring.
Furthermore, we found numerous incidents of outlier data for the Zeriscope device, which will require further refinement of the signal acquisition protocol, before it is ready for clinical use. There is also the need to filter the stream of data before the examination of HRV data. In our study, the unfiltered Zeriscope device data were compared against filtered data that are generated through a standard ECG Holter monitor. Our pilot does exceed related studies in reducing error by using raw, exported device data rather than visually observed HR data. 20 More importantly, the results of this pilot study highlight the importance of testing the validity, reliability, and usability of monitoring devices before large-scale investigational clinical trials that examine HRV in service members with TBI/PTSD.
Since the start of this study, many new options for acquiring real-time heart rate data are rapidly being marketed. 21 This raises the need to test the validity, reliability, and usability of each of these devices, and to understand the need for consistency of measurement across each new device. Moreover, it suggests further challenges in adequately assessing the clinical utility of these devices, as the technology may be perceived as “outdated” by the time a clinical study has been completed. Timely testing of new devices is essential before clinical deployment and requires careful planning to ensure efficient patient recruitment and accuracy of data collection.
Conclusions
Monitoring HRV as a measure of ANS function likely has a significant role in enhancing the diagnosis and care of service members with TBI, including those with comorbid PTSD. 22 Although this pilot study suggests the clinical feasibility and patient acceptance of utilizing wearable devices to measure HRV in a clinical setting, further work is needed to develop and test more accurate and reliable wearable devices before deploying them within larger clinical settings. In addition, the findings from this study demonstrate the challenges with conducting real-time physiological monitoring of HRV during therapeutic interventions, and the importance of using raw data, rather visually observed HR data, to enhance accuracy. 20
Although this pilot study suggests that the Zeriscope device did not reach the desired standard of accuracy comparable with an ECG monitor among our sample of TBI patients, it does highlight what next steps may be beneficial for further development. From a technology readiness level (TRL) perspective, 23 we believe our findings can be represented as having achieved experimental proof-of-concept (TRL 3), with movement toward this technology being validated in the relevant context of military TBI (TRL 5).
We recognize that in a future study, a larger sample of military service members would be desirable to more comprehensively test the accuracy of this device in those who have a history of TBI. Also required will be further laboratory validation and refinement of data capture and filtering strategies to more precisely align ambulatory HRV data with standard ECG monitoring in order for the device to be ready for clinical use in a broader military deployed environment.
Footnotes
Acknowledgments
The authors thank Kalyn Jannace, MPH, Dylan Scarton, MS, Christopher Kim, MS, from the Uniformed Services University and Laura Crews, RN, CRC, for their coordination and organization of research efforts for this study.
Authors' Contributions
Dr. Pasquina developed the study protocol and data management. Drs. Uomoto, Skopp, Jenkins, Pasquina, Adams, Miller, and Scott contributed to the development of the study and content of the article. Dr. Adams also provided technical assistance as one of the collaborators at Zeriscope, Inc. Mr. Reini provided statistical analysis and writing content for this article and Mr. Thomas assisted with the development and execution of the study protocol. Ms. Tsui contributed to article content and research coordination for the study.
Disclosure Statement
The views expressed in this article are those of the authors and do not necessarily represent the official policy or position of the Defense Health Agency, Department of Defense, Department of Veterans Affairs, any other U.S. government agency, the U.S. government, or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. This work was prepared under Contract HT0014-21-C-0012 with the DHA Contracting Office (CO-NCR) HT0014 and, therefore, is defined as U.S. government work under Title 17 U.S.C.§101. Per Title 17 U.S.C.§105, copyright protection is not available for any work of the U.S. government. The investigators have adhered to the policies for protection of human subjects as prescribed in 45 CFR 46. For more information, please contact
Funding Information
This material is based on work supported by the Advanced Medical Technology Initiative (AMTI) Program Award Number 64520 to the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., and HU0001-17-2-0011 to the Center for Rehabilitation Science Research, Department of Physical Medicine & Rehabilitation, and the Uniformed Services University. This material is the result of work supported, in part, by resources at the Robley Rex VA Medical Center, Louisville, KY.