
Abstract
Background:
Telemedicine has emerged as a feasible adjunct to in-person care in multiple clinical contexts, and its role has expanded in the context of the COVID-19 pandemic. However, there exists a general paucity of information surrounding best practice recommendations for conducting specialty or disease-specific virtual care. The purpose of this study was to systematically review existing best practice guidelines for conducting telemedicine encounters.
Methods:
A systematic review of MEDLINE, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) of existing guidelines for the provision of virtual care was performed. Data were synthesized using the Synthesis Without Meta-Analysis (SWiM) guideline, and the Appraisal of Guidelines for Research & Evaluation Instrument (AGREE II) tool was used to evaluate the quality of evidence.
Results:
A total of 60 guidelines for virtual care encounters were included; 52% of these were published in the context of the COVID-19 pandemic. The majority (95%) of provider guidelines specified a type of virtual encounter to which their guidelines applied. Of included guidelines, 65% provided guidance regarding confidentiality/security, 58% discussed technology/setup, and 56% commented on patient consent. Thirty-one guidelines also provided guidance to patients or caregivers. Overall guideline quality was poor.
Discussion:
General best practices for successful telemedicine encounters include ensuring confidentiality and consent, preparation before a visit, and clear patient communication. Future studies should aim to objectively assess the efficacy of existing clinician practices and guidelines on patient attitudes and outcomes to further optimize the provision of virtual care for specific patient populations.
Introduction
Telemedicine is a subset of virtual care defined as the use of information technology for the provision of health care through remote patient–provider interactions. 1 It has emerged as not only a feasible and safe adjunct to in-person care in multiple clinical contexts but also a modality with numerous benefits for patient care. Indeed, telemedicine has been shown to improve patient financial burden, quality of life, and overall patient-important outcomes, including adherence to therapy, health care utilization, and disease activity, 2 as well as reduce overall health care costs. 3
Despite these benefits, barriers such as a lack of infrastructure surrounding physician licensing and reimbursement, issues with the implementation of appropriate technology, privacy concerns, and patient and provider acceptance have limited the widespread integration of virtual care into regular practice. 1,4
The COVID-19 pandemic created unprecedented changes across numerous domains, including accelerated implementation and use of virtual care in multiple disease contexts. 5 Indeed, telemedicine encounters made up 77% of ambulatory visits in Ontario, Canada, 6 and up to 42% of visits in the United States in April 2020. 7 Although studies of patient and provider satisfaction with telemedicine have generally been favorable, 8 one survey of gastroenterology providers identified that 50% felt abandoned with the heightened responsibilities associated with telemedicine visits, suggesting a need for best practice guidelines. 9
Although guidance has been provided surrounding medicolegal principles and considerations for the general provision of virtual care by various medical regulatory bodies, 10 there exists a paucity of information surrounding best practices for conducting specialty and disease-specific virtual care. Such recommendations are important for ensuring the provision of safe and high-quality telemedicine. 11 Therefore, the purpose of this study was to systematically review existing best practice guidelines for conducting telemedicine encounters, synthesize available evidence, and highlight strategies to optimize virtual care.
Methods
SEARCH STRATEGY
We comprehensively searched MEDLINE, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) from January 1, 2000, to January 1, 2021. This limitation was implemented to streamline the screening process, as guidelines published before 2000 were less likely to be relevant to modern telemedicine practices and technology. The search was designed and conducted with input from a medical research librarian (complete search strategy is available in Supplementary Fig. S1). We also manually searched the references of published studies, websites of scientific societies cited in published guidelines, and gray literature (e.g., conference proceedings, unpublished trial data) to ensure that relevant articles were not missed. We did not discriminate full texts by language.
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Fig. 1).
12
The protocol of this study was registered a priori at the Open Science Framework and is available at
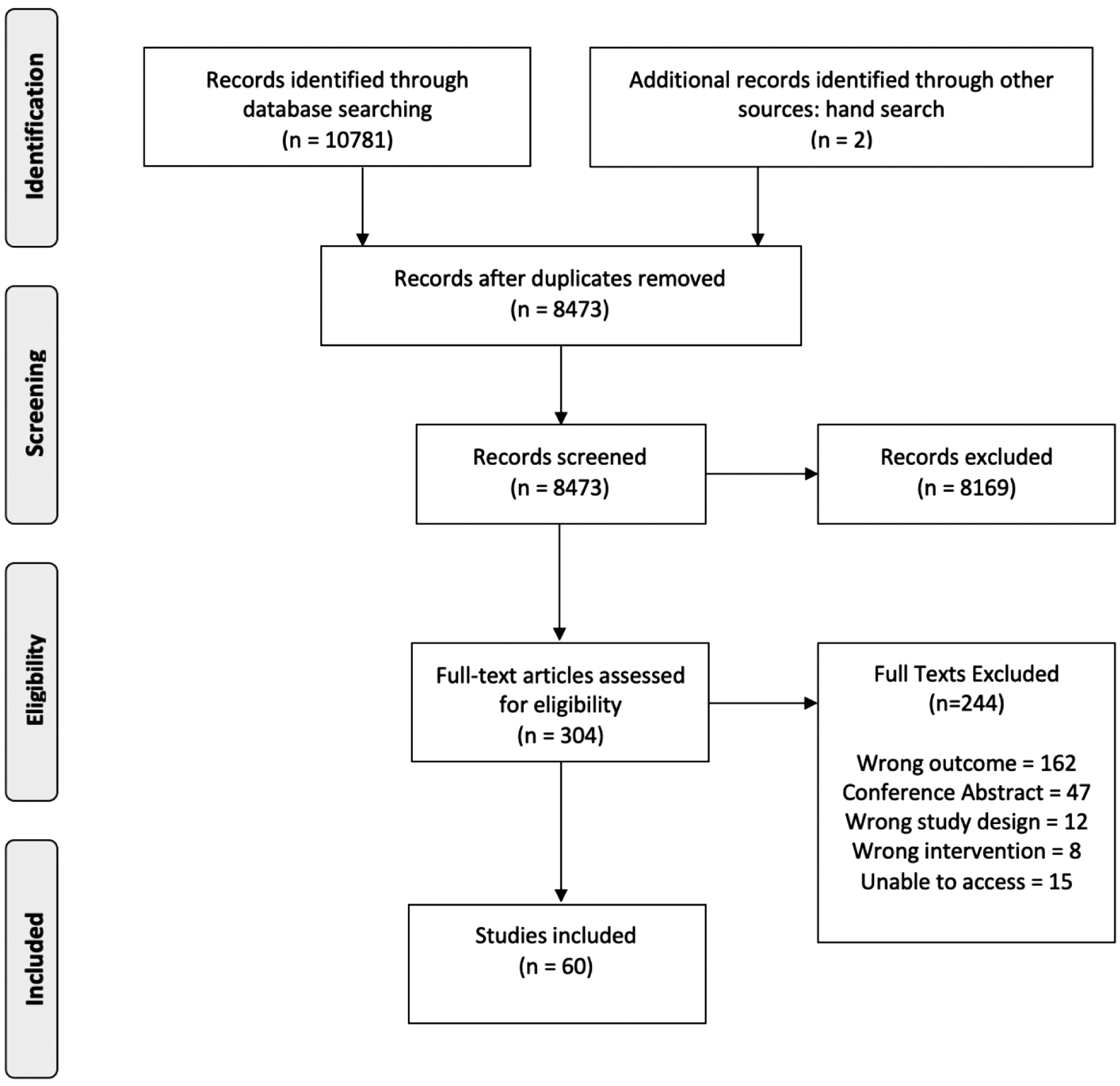
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
FINDINGS
The primary finding of interest was the description of guidelines or best practices for the provision of telemedicine encounters. We also recorded whether guidelines were drafted in the context of the COVID-19 pandemic. Secondary findings of interest included the description of best practices for patients or caregivers, as well as reported limitations of telemedicine encounters.
ELIGIBILITY CRITERIA AND DATA ABSTRACTION
We included guidelines that described best practices or guidance for conducting telemedicine encounters (either telephone or video/web-based medical encounters) in human participants. We defined telemedicine as the use of information technology for the provision of clinical care through remote patient–provider interactions. 1 Studies were eligible for inclusion if they reported guidelines or best practices for telemedicine encounters in human patients, were targeted toward health care practitioners (e.g., physicians, nurses, nurse practitioners, clinical psychologists), and, if applicable, included >5 participants. Guidelines developed by a professional society were classified as “society recommendations,” whereas guidelines developed by individual authors were labeled as “independent recommendations.”
Two reviewers independently evaluated titles and abstracts using a standardized pilot-tested form. Discrepancies that occurred at the title and abstract screening stages were resolved by automatic inclusion to ensure that relevant articles were not missed. Discrepancies at the full-text stage were resolved by consensus between two reviewers, and if disagreement persisted, a third reviewer was consulted. Two reviewers independently performed data abstraction onto a data collection manual designed a priori.
Abstracted data included guideline characteristics (author, year of publication, country, design), whether the guideline was published in the context of the COVID-19 pandemic, target population demographics (disease/area of health care, health care specialist of interest), guideline characteristics (including type of encounter studied), and best practice recommendations by domain (patient selection, confidentiality, consent, technology, preparation, training, physical environment, verbal communication, nonverbal communication, documentation, and prescribing). These domains were created from common themes identified through a review of the literature. Secondary findings of interest such as recommendations for patients/caregivers and outcomes (provider benefits, patient benefits, reported limitations and challenges) were also recorded.
DATA SYNTHESIS AND QUALITY ASSESSMENT
Data were synthesized according to the Synthesis Without Meta-Analysis (SWiM) guideline. 13 Data were synthesized according to the type of telemedicine encounter and, if applicable, by disease category. The Appraisal of Guidelines for Research & Evaluation Instrument (AGREE II) tool was used to assess quality and risk of bias for included guidelines. 14 The AGREE II tool assesses the methodological rigor and transparency with which clinical practice guidelines are developed, grading guidelines over six domains: scope and purpose, stakeholder involvement, rigor of development, clarity of presentation, applicability, and editorial independence. Guidelines are then assessed based on overall quality and whether they would be recommended for use in practice.
Per the AGREE II User's Manual, domains that were not reported were rated as 1 (absence of information). Domain scores were then calculated by summating the scores of the individual items in a domain and by scaling the total as a percentage of the maximum possible score for that domain. Using findings from prior publications, domain and overall reported percentages <50% were designated as low quality. 15 –17
Results
GUIDELINE CHARACTERISTICS
Our initial search identified a total of 8,473 potentially relevant citations. Following screening, a total of 60 guidelines were eligible for inclusion. Patient and guideline characteristics are summarized in Table 1. Included guidelines were published between 2005 and 2021, and 52% (31/60) were published in the context of the COVID-19 pandemic. Of included guidelines, 43 provided guidance for videoconference encounters, 18 –60 2 for telephone, 61,62 10 for both, 63 –72 and 5 for unspecified 73 –77 telemedicine encounters.
Guideline Characteristics
AHRQ PCOR, Agency for Healthcare Research and Quality and the Patient-Centered Outcomes Research; APA, American Psychiatric Association; ATA, American Telemedicine Association; HCP, health care provider; HRSA NRSA, Health Resources & Services Administration National Research Service Award; NIH, National Institutes of Health.
Areas of health care for which guidance was provided included general medicine (10/60), 21,24,35,37,38,41,42,62,63,71 dermatology (3/60), 26,33,64 mental health care including psychiatry and psychology (17/60), 18 –20,22,23,29,30,32,46,48,49,53,57,67,72,75,76 neurology (including stroke, traumatic brain injury, epilepsy, and general neurology) (8/60), 27,28,31,40,45,52,65,73 pediatrics and pediatric subspecialties (5/60), 25,36,39,61,66 ophthalmology (3/60), 34,44,69 cardiology (1/60), 50 physiotherapy/rehabilitation (2/60), 59,70 surgery (including general surgery, plastic surgery, otolaryngology, urology, and orthopedic surgery) (8/60), 43,51,54 –56,68,74,77 medical education (1/60), 58 and general virtual care (2/60). 47,60
Included guidelines were predominantly independent recommendations (45/60), with the remainder being society recommendations. Of the independent recommendations, only one was endorsed by a professional society. 20
OVERVIEW OF GUIDELINE DOMAINS
Included guidelines were assessed for inclusion of relevant domains of guidance for providers of virtual care, which are summarized in Table 2, and for patients and caregivers (Table 3). Provider domains included type of encounter, patient selection, confidentiality/security, consent, technology/setup, preparation, training/competence, virtual communication/rapport, nonverbal communication, documentation, prescribing, and other guidance. Patient/caregiver domains included pre-appointment preparation, appearance/physical environment, identification, consent, technological consideration, communication (verbal/nonverbal), and other guidance.
Guideline Domains Reported (Provider)
Present within a guideline.
Guideline Domains Reported (Patient/Caregiver)
Present within a guideline.
The majority (95%) of provider guidelines specified a type of virtual encounter to which their guidelines applied. Although specifications within guidelines varied, 65% provided guidance regarding confidentiality/security, 58% discussed technology/setup, and 56% commented on patient consent. Conversely, guidance on patient selection (31%), documentation (27%), and prescribing (12%) was infrequent. Of included guidelines, 52% (31/60) provided guidance for patients or caregivers with respect to telemedicine encounters. Of these, the most common guidance was provided around appearance and physical environment (included in 87% of guidelines), whereas patient identification was least frequently discussed (5/31 guidelines).
LIMITATIONS
Limitations were inconsistently reported and, where available, are summarized in Supplementary Table S3. With respect to the telemedicine encounter itself, commonly reported challenges included providing clinical care without a conventional physical examination, high degrees of resource allocation required to develop telemedicine infrastructure, and lack of provider experience with virtual care. With respect to the creation of telemedicine guidelines, reported challenges identified included a lack of evidence on optimum strategies and difficulties with generalizing suggestions to other providers.
QUALITY OF EVIDENCE
Quality of evidence was evaluated using the AGREE II tool, and findings are summarized in Supplementary Table S4. The majority of included guidelines were rated as having poor overall quality, with a mean overall quality score of 3.05. Of the 60 included guidelines, 13/60 (22%) 18,27 –31,33,36,57,68,74,75,77 had a mean score of ≥50% across all 5 domains, suggesting fair overall guideline quality. Of these, only 1 was scored as recommended for use, 27 and the other 12 were scored as recommended with modifications.
Recommendations for telemedicine encounters by domain (providers)
A full summary of provider recommendations for conducting telemedicine encounters by domain is provided in Supplementary Table S1.
PATIENT SELECTION
Recommendations were given in 20 guidelines. Common themes included determining the appropriateness of a patient case for a virtual consultation and ensuring that a patient was able to complete a virtual visit (such as the ability to sit still, sufficient cognitive capacity) a priori. Most guidelines reporting this domain suggested that clinicians should use their discretion to evaluate the appropriateness of a telemedicine encounter on a case-by-case basis, with consideration of patient characteristics and the clinical case, to optimize patient care.
CONFIDENTIALITY/SECURITY
Guidance regarding confidentiality was provided in 39 guidelines and could be broadly categorized as (1) recommendations on the physical environment, (2) recommendations for the technology used to conduct a telemedicine encounter, or (3) communication with a patient regarding the potential for a breach in confidentiality.
Common themes included ensuring that the encounter was conducted in a secure environment with minimal disruptions (e.g., with doors and windows closed), confirming that technology used was appropriately secured and in compliance with HIPAA laws, communicating with patients regarding the security of the environment as well as the potential for breaches in confidentiality depending on the software used, limiting access to patient data from virtual appointments to relevant personnel, and ensuring that all individuals participating in a virtual encounter are appropriately identified and approved by the patient.
CONSENT
Thirty-four guidelines provided recommendations for eliciting patient consent in a telemedicine encounter. Of these, all recommended obtaining written consent from a patient to participate in telemedicine encounters in advance of or at the beginning of an encounter and ensuring that this was documented within the patient's chart. Obtaining verbal consent at the start of an encounter was also recommended.
TECHNOLOGY/SETUP
Thirty-eight guidelines provided guidance regarding telemedicine setup. Common themes included confirming that telemedicine equipment and technology was functional and met appropriate standards before a visit, ensuring that providers had a backup plan in place in the event of technology failure, and suggesting that providers familiarize themselves with the telemedicine modality in advance of an appointment. With respect to videoconferencing specifically, several included guidelines recommended that providers ensure that camera setups had sufficient bandwidth/resolution and were placed at eye level, that a split screen mode be used if available, and that a waiting room feature be used if available. Providers were also encouraged to seek feedback from patients to confirm that they were appropriately visualized.
PHYSICIAN PREPARATION
Thirty-one guidelines made recommendations for physician preparation before a telemedicine encounter. Common suggestions included ensuring that providers were familiar with the telemedicine modality used and had a backup plan available in the event of technological failure, confirming consent for a virtual care visit, minimizing distractions in the virtual care environment, and providing patients with a virtual visit checklist with any required preparation before the visit.
COMPETENCY/TRAINING
Recommendations regarding provider competency or training were made in 22 included guidelines. Common themes included ensuring that all providers and support staff were trained in the use of equipment and software before a virtual visit. Some guidelines also suggested that providers receive specific training in conducting virtual care in their area of expertise and engage in ongoing professional development in this domain to develop and maintain skills specific to the provision of virtual care.
VERBAL COMMUNICATION/RAPPORT
Twenty-two guidelines provided guidance on verbal communication and building rapport in the virtual environment. Recommendations were made with respect to both the manner and content of provider communication with patients and caregivers. Common suggestions included ensuring that speech was slow, deliberate, and clearly enunciated, taking frequent pauses to allow patients the opportunity to speak up, and allowing the patient the opportunity to open the conversation. With respect to content, several guidelines suggested clearly verbalizing throughout any virtual physical examination, requesting permission to take notes, and communicating a fail-safe option in the event of technological difficulty.
NONVERBAL COMMUNICATION
Guidance for nonverbal communication in telemedicine encounters was provided in 21 included guidelines and was primarily relevant to videoconferencing encounters. Common recommendations included having providers look directly into the camera or position the patient's video directly below the camera to simulate eye contact, exaggerating nonverbal signs of encouragement such as head nodding and facial expressions, ensuring that providers were centered in the screen, avoid multitasking during an encounter, and ensuring that hand gestures were made in full view of the camera by positioning the hands at mid-chest.
DOCUMENTATION
Seventeen guidelines made recommendations for documentation during telemedicine encounters. Suggestions included ensuring that the patient encounter, modality of appointment, individuals present, consent for telemedicine encounter, and content of visit were appropriately documented. Some guidelines also suggested that providers use a template to ensure that these key elements of documentation were maintained.
PRESCRIBING
Seven guidelines provided guidance for medication prescribing in telemedicine encounters. Guidelines recommended following the same recommendations as would be made for in-person prescribing. However, one guideline did recommend adding a disclaimer to a prescription that the treatment was advised based on history alone.
OTHER RECOMMENDATIONS
Other recommendations for telemedicine encounters included taking written notes in lieu of typed notes to minimize distractions, offering group videoconferencing depending on the nature of the encounter, and involving a caretaker at the appointment where appropriate.
Recommendations by domain (patient/caregiver)
Of included guidelines, 31 provided recommendations for telemedicine encounters aimed at patients and/or caregivers, which are summarized in Supplementary Table S2.
PRE-APPOINTMENT PREPARATION
Seven guidelines provided patient recommendations for preparation before a telemedicine encounter. Recommendations included completing any designated pre-appointment checklists, checking internet connection before the appointment, having materials available for note-taking, and ensuring that the appointment environment was appropriate.
APPEARANCE AND PHYSICAL ENVIRONMENT
Twenty-seven guidelines provided guidance for patients with respect to their appearance and physical environment before a telemedicine encounter. Common areas of guidance included patient attire (e.g., wearing clothing that allows for physical examination and can be easily adjusted/removed) and positioning (e.g., ensuring camera is at eye level). Suggestions for physical environment included conducting the encounter in a private quiet space with minimal distractions, choosing a blank backdrop when possible, and using earbuds to optimize audio. Several guidelines also suggested that patients with special needs (such as elderly patients, children, or those with disabilities) have a caregiver nearby to assist as needed.
IDENTIFICATION
Four guidelines provided guidance for patients with respect to identification. Recommendations included ensuring that patients had photo ID available and clearly identified themselves and any other individuals in the room by full name.
TECHNOLOGICAL CONSIDERATIONS
Seventeen included guidelines provided patient or caregiver recommendations for technology use. Common recommendations included ensuring that patients confirm their technological setup in advance and share their video when appropriate. Some guidelines also encouraged patients to communicate any technological difficulties or anticipated challenges with their provider in advance when able.
COMMUNICATION
Six guidelines provided guidance to patients or caregivers with respect to communication in a telemedicine encounter. Suggestions included positioning the camera to maintain eye contact, refraining from multitasking during an appointment, speaking slowly and clearly, and clearly communicating any symptoms or complaints to the provider.
Discussion
In this systematic review, we identified several common best practice recommendations across a broad range of disciplines and modalities for the provision of telemedicine, as well as 10 domains that may provide a framework for future guidelines. A summary of recommendations is provided in Table 4.
Summary of Best Practice Recommendations for Providers of Virtual Care
Telemedicine provides a unique opportunity for clinicians to meet increasing care demands and overcome patient barriers to in-person care. Although telemedicine has existed since the 1960s, its expansion into routine clinical practice has been limited by a variety of barriers, including the cost of implementation and infrastructure, concerns regarding financial reimbursement and patient privacy, and resistance to change. 4,78 However, constraints on in-person health care caused by the COVID-19 pandemic have led to an unprecedented expansion in the provision of virtual care, 79 necessitating rapid implementation of new technology and clinical practices. Given telemedicine's convenience and cost-effectiveness, 3 its use has persisted throughout the COVID-19 pandemic, 80 highlighting a need for provider competence in conducting successful telemedicine encounters.
Although the response to telemedicine has generally been favorable, 81 –83 providers have cited maneuvering technology and difficulties building rapport as potential challenges. Similarly, while patient perceptions of virtual care have generally been positive, 84 previous surveys have revealed challenges such as difficulty establishing a provider–patient relationship, privacy concerns, and perceptions of feeling neglected during electronic visits that are amenable to quality improvement. 85,86
Studies of perceived physician empathy in telemedicine encounters in several disease contexts have also identified strategies to improve telemedicine communication that may not be widely incorporated into patient care. 87 To address these challenges, guidelines for conducting telemedicine encounters have been published by several societies, such as the American Telemedicine Association, 30,73,74 for a variety of disease contexts. 21,35,40 While provider and patient satisfaction with telemedicine as a whole has been well studied in several disease contexts, 88 there is a paucity of literature examining the impact of adherence to specific best practice guidelines and whether they actually impact the quality of virtual care. As the role of virtual care continues to expand, this will represent an important area of future study.
Our review identified several common themes across existing guidelines, which may be used as a checklist by individual providers and modified based on specific disease contexts. This study, however, is not without limitations. While we were able to synthesize existing recommendations across a broad range of clinical practitioners and diseases, a major limitation of this work is a paucity of evidence-based guidelines for the provision of virtual care and the overall poor quality of existing guidelines.
Indeed, many included guidelines were based primarily on provider experience and anecdotal practice as opposed to more robust assessments of efficacy, a limitation that has been identified in other evaluations of telemedicine guidelines. 89 Furthermore, given the relatively recent expansion of telemedicine during the COVID-19 pandemic, 5 many older guidelines were developed with a lower quantity of telemedicine users and less overall evidence to inform a systematic evaluation of virtual care practices.
Similarly, opportunities to include stakeholders and evaluate the impact on virtual care were limited. As such, despite a rigorous development process, many included guidelines did not address the specific domains graded by the AGREE II tool, resulting in lower domain scores. However, when reported, robust methodology was considered when determining the overall quality score awarded to individual guidelines.
Although the AGREE II tool is currently the standard for evaluating the quality of evidence for guidelines in health and disease, future studies addressing its appropriateness for evaluating guidelines in telemedicine may be beneficial given the unique challenges of conducting research in this area. This study also highlights an important need for updated high-quality guidelines for the provision of virtual care.
As telemedicine becomes a routine element of health care, there is a growing need for clinical trials to assess best practices within a telemedicine encounter to provide clinicians with evidence-based guidance. As in-person visits resume, future studies should aim to identify successful provider behaviors and patient-important outcomes from virtual encounters to further streamline and delineate the role of telemedicine. Evaluating the impact of existing guidelines on patient experiences and outcomes is another important area of research that warrants future study.
Conclusions
Telemedicine has become a routine element of clinical care in a variety of disease contexts. Best practices for successful telemedicine encounters include ensuring confidentiality and consent, preparation before a visit, and clear patient communication. Future studies should aim to objectively assess the efficacy of existing clinician practices and guidelines on patient attitudes and outcomes to further optimize the provision of virtual care for specific patient populations.
Footnotes
Authors' Contributions
S.A., S.N., R.J., A.S., and T.X. contributed to the conception and design of the study. S.A., S.N., R.J., and K.P. were involved in the acquisition, analysis, and interpretation of data. All authors contributed to the drafting, revision, and final approval of the article.
Acknowledgments
Thank you to Dr. Sarah Neil-Stztramko and the National Collaborating Centre for Methods and Tools team for their assistance with the conception of this review.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.