
Abstract
Introduction:
The French Tele-Medical Assistance Service (TMAS) provides medical teleconsultation for any ship at sea. At the end of the consultation, the doctor decides whether the problem can be taken care of onboard or not. In this study, we determined the factors associated with the decision for disembarkation or evacuation in case of wounds.
Methods:
We conducted a retrospective epidemiological study between 2011 and 2019 from consultations with the French TMAS. The inclusion criterion was the presence of an acute wound.
Results:
One thousand six patients (n = 1,006) were analyzed and 586 (58%) patients were disembarked or evacuated. Factors associated with disembarkation or evacuation are wound characteristics (severity and location), the onboard staff's medical training, the availability of photography, and the ship's location. Wound severity is a risk factor for disembarkation or evacuation. The availability of photography, staff with advanced training, and being at >1 day of navigation from a harbor are protective factors against being disembarked or evacuated.
Conclusion:
The added value of photography and an update of medium medical training could increase the number of wounds taken care of onboard.
Introduction
The French Tele-Medical Assistance Service (TMAS) provides 24-h emergency teleconsultation for any ship at sea. Most consultations are conducted by phone and photography can be sent by email. Technological progress can complement clinical data, thanks to the transmission of electrocardiograms or videoconferences. 1,2 The French TMAS also plays an important role in medical training. In France, there are three levels of medical training based on the ship's gross tonnage and its maximum navigated distance.
Basic training (level 1), which comprises 11 h of training, is required for ships of a gauge <200 Universal Measurement System (UMS) not moving >20 nautical miles from the shore. Medium training (level 2), which comprises 50 h of training, is required for ships of a gauge between 200 and 500 UMS and that do not move >200 nautical miles from the shore. Finally, advanced training (level 3), which comprises 97 h of training, is required for ships of a gauge >500 UMS sailing farther than 200 miles from the shore.
Wound management is part of the medical training. Depending on the medical training received, the staff responsible for medical care on board can apply staples or give stitches. Most wounds require a medical evaluation, specific medical care, and sometimes surgical intervention. At the end of the teleconsultation, the doctor decides whether the problem can be taken care of onboard or not. If not, the patient can be disembarked or evacuated. The disembarkation can be performed at the planned harbor or a closer one. The evacuation can be realized by a medical team or not, and by any means, such as boat or helicopter.
The financial consequences of disembarkation or evacuation are important. There are costs associated with medical care and those arising from rerouting, delivery delays, or sailor replacement. Costs can reach several thousands of euros, depending on the pathology. 3
The objective of this study was to determine factors associated with the decision for disembarkation or evacuation in case of wounds.
Materials and Methods
STUDY DESIGN AND SETTINGS
We conducted a retrospective epidemiological study between 2011 and 2019 at the French TMAS (Toulouse University Hospital). During the inclusion period, 17,098 teleconsultations were registered at the French TMAS. All teleconsultations performed by the French TMAS are logged in a specific database (AppliCCMM®). For each teleconsultation file, the TMAS emergency physician describes his or her diagnosis and the therapeutics proposals.
PARTICIPANTS AND DATA SOURCES
The inclusion criterion was the presence of an acute wound. The exclusion criteria were missing data concerning the type of wound (location and severity), missing decision, and associated lesion requiring disembarkation or evacuation (e.g., scalp wound associated with severe head trauma).
Data were extracted from teleconsultation files that had a coded diagnosis of “wound,” “multiple superficial lesions,” “traumatic amputation,” “traumatic lesion,” or “crushing.”
VARIABLES AND OUTCOME
Variables were collected by the investigator and manually added in an anonymized Microsoft Excel® file (Microsoft, Redmond, WA). Collected data concerning the patient were gender, age, relevant medical history (diabetes, anticoagulant medication, or hemophilia), and occupation. Collected data concerning the wound were cause of the injury, location, and severity. Possible causes of injury were direct impact, fall, cut, accidental compression, and other. Possible wound locations were dorsal hand, palmar hand, limb, head, or other. We decided to choose a two-category scale for wound severity due to retrospective data that did not allow us to use a complex injury scale like the Abbreviate Injury Scale.
If the wound was life threatening or put the functional prognosis at stake, the severity level was considered “high.” Otherwise, the severity level was considered “low.” Photography availability was also assessed. Collected data about the ship were ship type, onboard staff medical training, and ship location (estimated in days to reach the closest harbor). There are three levels of onboard staff medical training. Concerning wound management, disinfection and bandaging are taught in basic training, closure by staples is taught in medium training, and closure by stitches is taught in advanced training.
The outcome was the decision for disembarkation or evacuation made by the TMAS emergency physician.
ETHICS
After evaluation and validation by the data protection officer of our university hospital and pursuant to the General Data Protection Regulation, this study was registered in the Retrospective Study Register of Toulouse University Hospital (French National Commission for Informatics and Liberties [CNIL] No.: 2206723 v 0).
STATISTICAL ANALYSIS
Statistical analyses were performed using SAS 9.2 (SAS Institute, Cary, NC). Missing values were not imputed. Age was expressed as a median and its interquartile range (median [IQR]) and comparison were performed using a Mann–Whitney test. Categorical variables were expressed in terms of frequency and percentage (n [%]) and comparisons were performed using the chi-squared test. A logistic regression using a forward procedure was performed to identify the factors associated with the decision for disembarkation or evacuation. Multivariate analysis was performed on patients without missing data (n = 929). All variables with a p-value <0.2 in the univariate analysis were added to the regression model. Only the final model is shown in the article with its area under curve (AUC).
Results
One thousand six hundred sixty teleconsultation files were extracted and 1,006 were analyzed (Fig. 1). Four hundred twenty patients (42%) were taken care of onboard and 586 (58%) patients were disembarked or evacuated. Patient characteristics are shown in Table 1. Patients were mostly men (n = 919, 92%) with a median age of 39 (28–49) years old. Most of wounds were due to occupational injury (n = 714, 75%), were hand wound (n = 571, 57%), and were considered as severe (n = 719, 72%). Photography was available for less than half of them (n = 413, 41%).
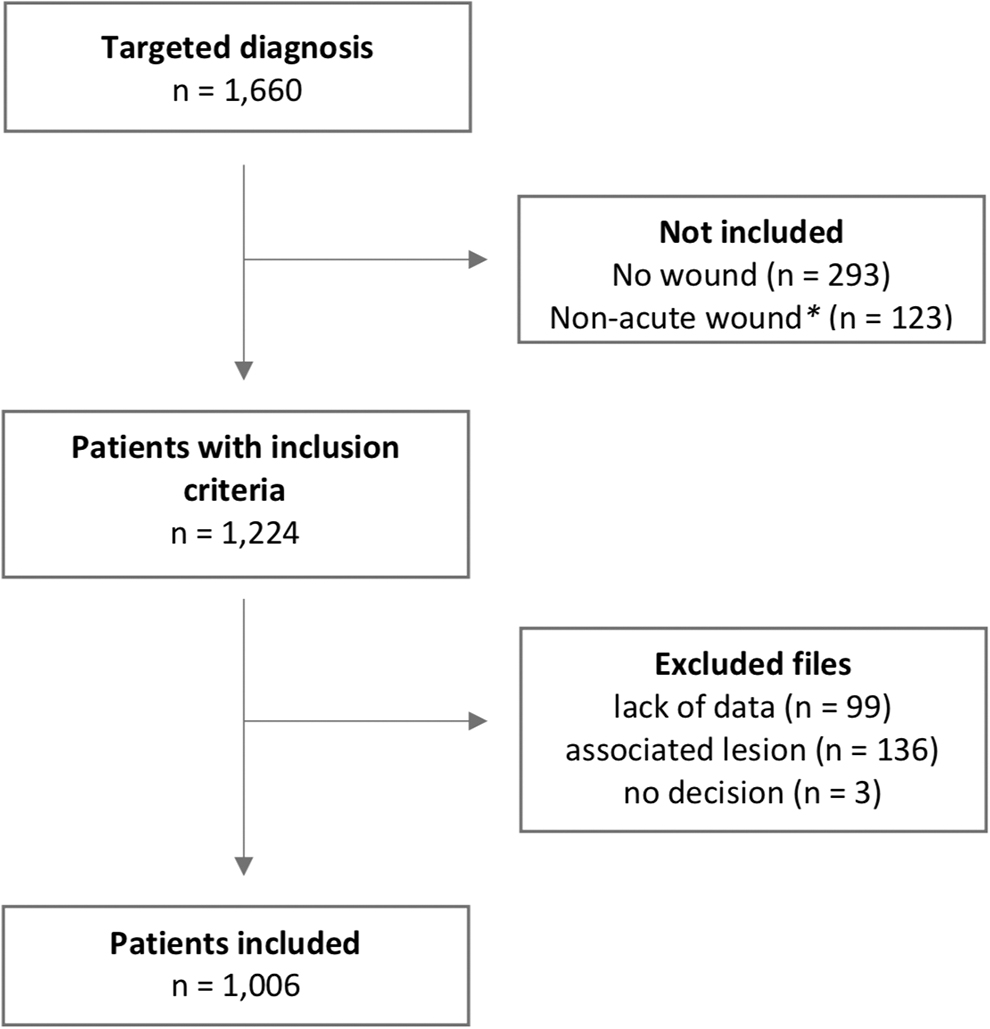
Flow chart. *Including chronic wounds and calls for follow-up.
Patient Characteristics
Missing data n = 29.
Missing data n = 2.
Missing data n = 41.
Missing data n = 37.
Missing data n = 79.
Most of ships were at <24 h away from a harbor (n = 642, 69%) and 166 (17%) did not have any medical trained staff onboard. In the univariate analysis, seafarers' occupation, cause of injury, wound location and severity, availability of a photography, type of ship and its location, and onboard staff medical training seem to influence the medical decision for disembarkation or evacuation.
The final regression model with variables and odds ratio (OR) are presented in Table 2. Compared with dorsal hand wound (reference), palmar hand wound (OR = 3.74; confidence interval [CI] 95% = [2.23 to 6.27]), limb wound (OR = 2.49; CI 95% = [1.30 to 4.77]), and other wound location (OR = 166.9; CI 95% = [2.47 to >999]) were more likely to be disembarked or evacuated. High-severity wounds were more likely to be disembarked or evacuated than low-severity wounds (OR = 6.44; CI 95% = [3.41 to 12.17]).
Factors Associated with Decision for Evacuation or Disembarkation (n = 929) (AUC = 0.91)
CI, confidence interval; OR, odds ratio; AUC, area under curve.
Files that include photography were less likely to be disembarked or evacuated (OR = 0.20; CI 95% = [0.13 to 0.31]) compared with files that do not have any photography available. Compared with ships located at <1 day of sailing to reach a harbor (reference), ships that were at 24–72 h from a harbor (OR = 0.35; CI 95% = [0.21 to 0.58]), 3 to 10 days from a harbor (OR = 0.15; CI 95% = [0.07 to 0.29]), and >10 days from a harbor (OR = 0.01; CI 95% = [0.01 to 0.11]) were less likely to be disembarked or evacuated. When there was staff with advanced training on board, patients were less likely to be disembarked or evacuated (OR = 0.25; CI 95% = [0.13 to 0.47]).
Discussion
The objective of this study was to determine factors associated with the decision for disembarkation or evacuation of wounds. Seafarers' working conditions are rough, and risks to their health are higher than the national average. Several studies show that severe or fatal traumatic injuries are more frequent in seafarers than in other working areas. 4,5 In France, in 2019, 60 work-related accidents per 1,000 seafarers were reported versus 33.5 work-related accidents per 1,000 employees onshore. 6 Onboard, many occupations are manual and physical, and thus responsible for a high risk of injuries, in addition to the sea conditions, which can be difficult: rough sea, stress, and fatigue. 7
Wound management, which sometimes requires medical or surgical advice, is a major issue in maritime telehealth. Trauma, which represents up to 20% of medical problems onboard, 8 is a frequent subject, but most studies focus on a certain type of ships: merchant ship, fishing boats, or passenger ships. 9 –11 Risks factors of trauma are well described. 12,13 The repatriation rate (i.e., disembarkation or evacuation followed by return to home country) for trauma is high, up to 21% in some studies. 14 Our study, which focuses on a large population, introduces a variable that has never been studied before: staff medical training. The disembarkation/evacuation rate was 58% in our study. In comparison, during the same period of time, 36% of patients, overall files, were disembarked or evacuated.
Five factors were identified as being associated with the decision for disembarkation or evacuation: wound severity, wound location, ship location, photography availability, and staff medical training. As expected, a wound with a functional or vital prognosis at stake is more likely to be disembarked or evacuated. Almost half of the wounds in this study were hand wounds, and these represented >63% of the disembarkation/evacuation group. Several studies show that the hand and the upper limb are the most common locations for trauma onboard. 15
Those locations may require an X-ray to assess an associated fracture, which may influence the decision of disembarkation or evacuation. In the multivariate analysis, every wound location except the head was more likely to be disembarked or evacuated than a dorsal hand wound. It would have been interesting to assess whether individual protective equipment, especially gloves, was worn at the time of the accident.
The availability of individual protective equipment is a major predictive factor of trauma. It is a key point in prevention. Regarding staff medical training, we decided to analyze wounds that occurred in all types of ships, including pleasure boats. With some exceptions, there is no medically trained staff on pleasure boats. For any other ship, medical training is mandatory. Our study shows that only advanced medical training was a protective factor against disembarkation or evacuation. Wound management is part of every level of medical training. Closure by staples is taught in medium training and closure by stitches is taught in advanced training.
As most wounds are hand wounds, stitches are more likely to be used. As such, it would be advisable to include stitches in medium training. Ships characterized by basic training are not far from harbors, and a medical evaluation seems preferable. Medical supply was not included in our model because of its correlation with medical training. An improvement in medical training would have to be associated with an improvement in medical supplies.
Concerning ship location, we decided to use a temporal unit of measure because the exact location was not always available and time to reach a harbor depends on the ship, weather conditions, and distance to the closest harbor. Being at >1 day of navigation was a protective factor against being disembarked or evacuated. It is important to notice that it is more difficult to disembark or evacuate a patient from a ship that is far away from a harbor. This seems to influence the medical decision of disembarkation or evacuation. Wounds are supposed to be taken care of within 6 h, which is almost impossible unless taken care of onboard. Photography availability was a protective factor against being disembarked or evacuated.
It allows for a better evaluation of wound severity, control of the closure method, and the evolution of the wound and its healing. 16 Less than half of all files included photography. This might be due to transmission difficulty, which is the main reason for the lack of use of telehealth in a recent study. 17
The use of telemedicine is mandatory in acute wound management onboard. We were able to determine factors associated with the decision of disembarkation or evacuation. Some of these factors cannot be modified and are related directly to the wound. We showed that photography and medical training may increase onboard management of acute wounds. Those two factors have already been described as barriers to the use of telemedicine in injury management. 18 Goh 19 shows that telemedicine management seems effective in wound management, however, most studies focus on chronic wounds. Further studies need to be done to assess the relevance of telemedicine management of acute wound.
LIMITATIONS
Our study determined the factors associated with the decision for disembarkation or evacuation but does not consider the human factor. As in any medical regulation, the appellant's panic, the doctor's experience, and the quality of communication are factors that can affect the decision. As a retrospective study, 8% of our cohort had missing values, leading to a final model with only 929 patients. An important bias was that a correlation between ship location and medical training may exist. Indeed, the further is the ship, the higher is the medical training required.
There was no collinearity between those two variables allowing us to perform the logistic regression, which considers the two variables independently. Moreover, our study focuses on initial management and not the evolution of the patient. We lack data concerning work incapacity or secondary disembarkation, and an impossibility to work for a seafarer would lead to a work overload for their colleagues.
Conclusion
Wounds are a serious concern in telehealth. Our study shows that wound characteristics (location, severity), staff medical training, photography availability, and ship location are associated with the decision for disembarkation or evacuation.
Ship location is not a factor on which we can act to reduce disembarkation or evacuation. In contrast, preventive medicine measures could emphasize the need to use individual protective equipment, in particular gloves. In the same way, staff medical training, especially medium training, could be updated. Photography, which allows a better evaluation of wound severity and follow-up, is a valuable asset in wound management.
Footnotes
Authors' Contributions
All authors helped to draft the article and to critically review its intellectual content. They have approved the final version to be submitted.
Disclosure Statement
No competing financial interest exist.
Funding Information
No funding was received.