
Abstract
Background:
We present an innovative care model for telehealth by creating a video conference group telemedicine program for patients with chronic disease and discuss findings from a post-program survey that was instrumental in understanding the response to telemedicine in a group setting.
Methods:
All patients who attended the group telemedicine program had a diagnosis of Hypermobile Ehlers-Danlos Syndrome or Hypermobility Spectrum Disorder and were requested to complete survey responses at the close of the program. Surveys were completed anonymously and electronically by REDCap. Elements of the Press Ganey, Consumer Assessment of Healthcare Providers and Systems, and Utah Telehealth Network patient satisfaction surveys were modified to construct the survey.
Results:
A total of 102 patients completed the post-telehealth program survey between August 20, 2021, and February 11, 2022. Around 93.1% stated that they gained a better understanding of the chronic condition, 88.3% stated that the program gave them the tools to improve, and 76.5% indicated the program addressed their specific needs. Approximately 92.1% found it easy to interact with the program facilitator and 79.4% found it easy to interact with program members. Around 93.1% said they would recommend the program to others.
Discussion:
We created a group telemedicine program for a complex chronic medical condition. The foundation of knowledge provided by the telemedicine program allowed more time during face-to-face encounters for individual assessment of the patient, and increased access to care. Overall, the program has improved the treatment process by reducing treatment burden and empowering patients with self-management skills to help reach our fundamental treatment goal of improving quality of life.
Introduction
Chronic noncommunicable diseases have devastating health consequences and socioeconomic costs. 1 Defined as diseases that persist for at least 1 year and require ongoing medical attention or limit daily activity, chronic diseases account for roughly 90% of the $4.1 trillion US annual health care expenditures. 2,3 With a growing aging population, this cost is expected to increase. Innovative tools to improve access to care are needed to meet the rising demand. Our general internal medicine practice has transformed methods that decrease the burden of care and serve patients with chronic disease that can be applied globally. This study came from experience treating patients suffering from chronic illness and multimorbidity arising from inherited disorders of the connective tissue, specifically, Ehlers-Danlos Syndrome (EDS).
EDS comprises a group of 13 genetically heterogenous connective tissue disorders. 4 The most common subtype and the only one without a known molecular etiology is hypermobile EDS (hEDS). There is significant overlap of hEDS with Hypermobility Spectrum Disorder (HSD). Because of similarity in symptoms and management of these two conditions, they will be addressed together here. In these two disorders, multiorgan comorbidities are common and often debilitating, yet frequently unaddressed by clinical care teams.
Thus, patients with hEDS/HSD shoulder a burdensome workload managing their comorbidities, coordinating care, and living with an often-misunderstood chronic condition. In addition to their usual daily roles, routine activities of an hEDS/HSD patient include managing treatment plans, attending frequent medical appointments, maintaining a healthy lifestyle, and performing self-care. Counseling on the lifestyle aspects of hEDS/HSD care is crucial to provide the basic level of understanding needed by the patient to improve treatment outcomes. These demands make hEDS/HSD a suitable model to provide a framework for the study of other multimorbid diseases.
For any multimorbid disease, quality of life depends on the patient's personal knowledge of their medical condition. If education is not sufficiently provided and/or the workload is exceedingly taxing, the workload-capacity imbalance may jeopardize patient-centric outcomes, including clinical, well-being, and quality of life. Our group telemedicine program was designed and implemented for this purpose—to reduce overall treatment burden.
There is a general scarcity of evidence in the literature on group-based telemedicine for chronic diseases. However, studies investigating this area have found positive results, 5 or little difference between telemedicine and non-telemedicine patient groups. 6 Virtual care and telemedicine, which were bolstered as a result of the COVID-19 pandemic, provide accessible health care to many social groups that differ in age and experience at the same time. 7 Patients may find commonalities, alignment, and social support through group activities.
Herein, we describe the creation of a group telemedicine teaching program termed EDS Living conducted in groups to allow experts to meet multiple patients simultaneously and in a virtual setting—improving access to care. We hypothesized that this program would positively influence patient understanding of hEDS/HSD and we tested our hypothesis with patient-reported feedback. Treatment for hEDS/HSD and many chronic diseases is focused on self-management. For hypermobility, these include conservative pain control modalities, exercise, mind-body interventions, and nutrition. If the results of this program yield evidence of an improved understanding of how to manage living with a chronic disease, it will be an important additional resource in helping patients living with chronically debilitating conditions.
Methods
VIRTUAL GROUP EDUCATION PROGRAM
To serve the needs of patients with suspected or confirmed hEDS/HSD, a de novo EDS clinic was established in the fall of 2019 at our site. It was routinely observed that after evaluation by one or more providers, patients continued to have a high volume of questions about their condition. This provided insight and recognition of the amount of time needed to grasp common concepts of hEDS/HSD, which was limited by the amount of time available during scheduled visits. The group telemedicine program was designed to proactively educate patients on common topics and answer questions unique to patients with hEDS/HSD.
As the COVID-19 pandemic changed the face of health care, and with our widespread geographic reach, it was decided to create the EDS Living as a virtual experience. 7,8 In designing the program, specific personnel and technology were required, including administrative support, a physician with expertise on inherited disorders of the connective tissue, a full-time nurse as a program coordinator, and videoconferencing technology. Patients were eligible to attend EDS Living if they were diagnosed with hEDS/HSD and had at least one prior in-person visit to the EDS Clinic. The setting for the study was a large academic medical center in Florida.
The program was launched on June 4, 2021, and consisted of a total session time of 7 h. Total face-to-face time with a physician at each session was 1.5 h. Figure 1 exhibits the core learning methods applied to the teaching course. On average, seven patients attended each group session, with a range from 2 to 12. The full EDS Living program consisted of two physicians, three therapists (physical, occupational, and pelvic floor), a mind-body counselor, and a clinical nutritionist, with each providing an interactive 30-min to 1-h live session. A 1:1 counseling session was scheduled with the internal medicine physician to address individual needs. Full structure of program content is shown in Figure 2. Regular 15-min breaks were given between sessions with a full hour for lunch. See Supplementary Appendix S1 for the full program curriculum.
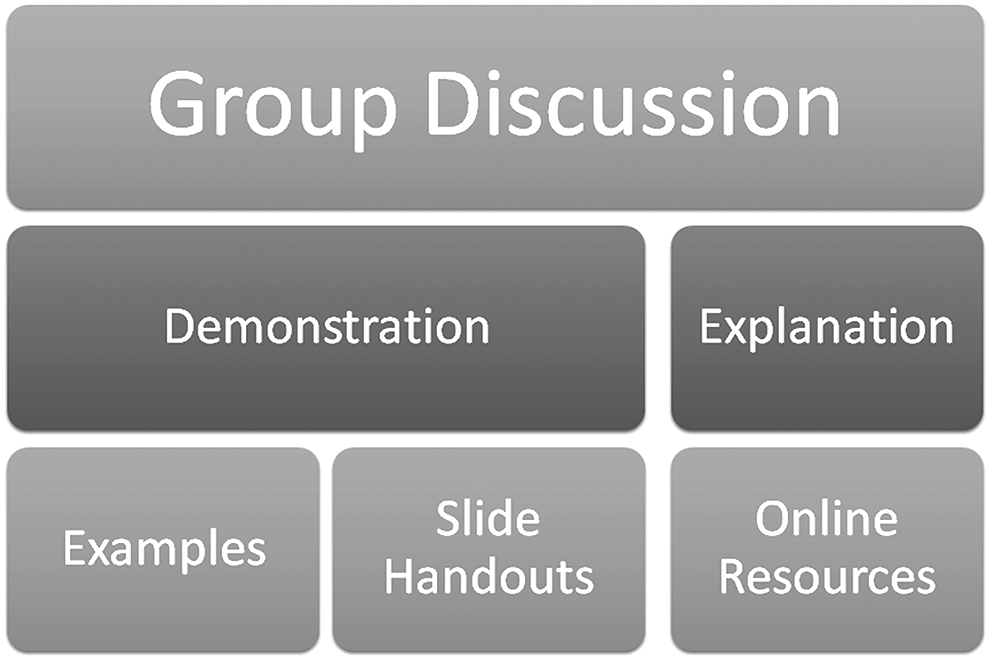
Methods of learning.
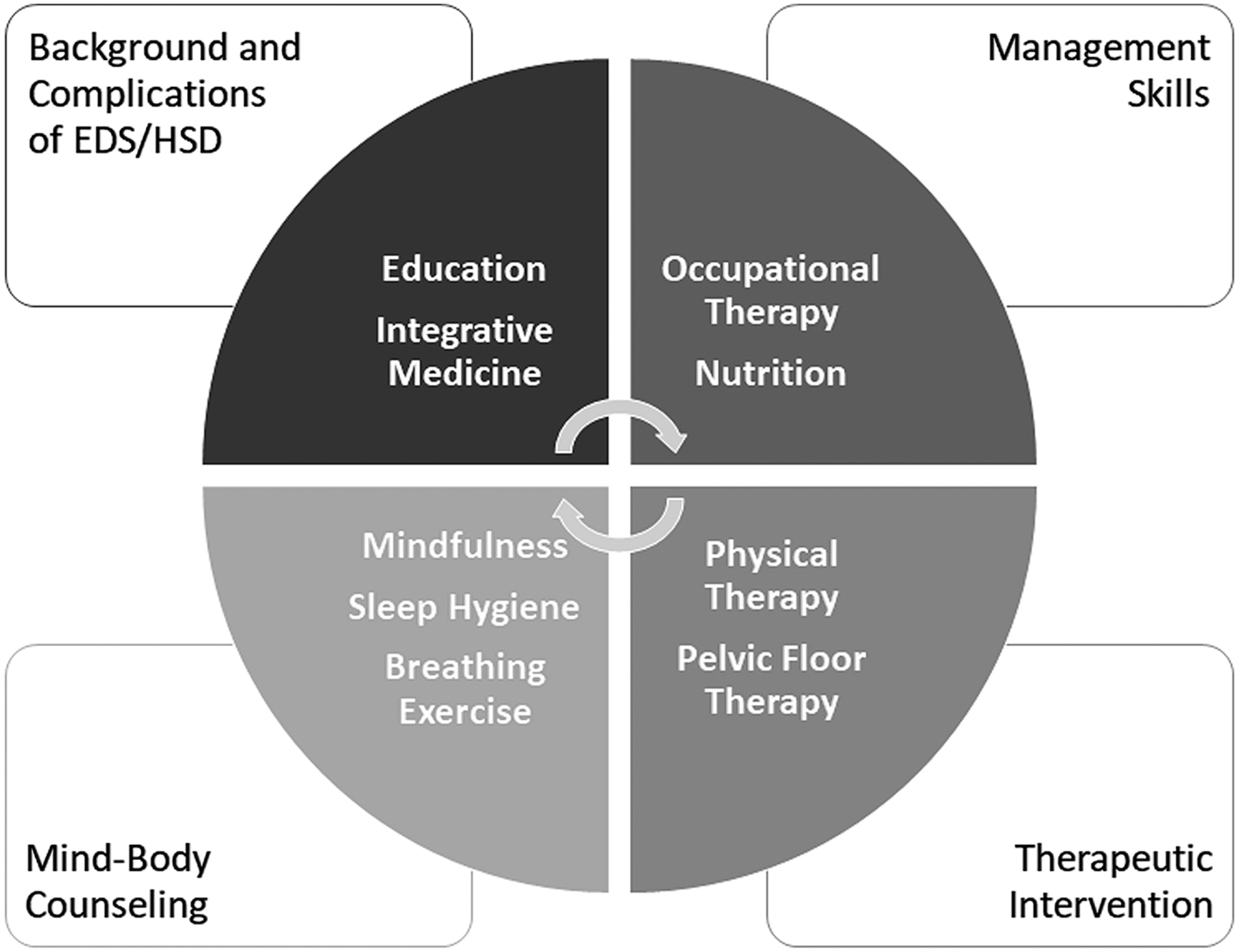
Class content.
ETHICS STATEMENT
Patient data reported in this article were approved by the Mayo Clinic Institutional Review Board (IRB) (IRB no. 19-011260) and informed consent was waived by the IRB for all patients. The research conformed to the principles outlined in the Declaration of Helsinki. Patient data were collected between August 20, 2021, and February 11, 2022.
PATIENT SURVEY
All patients who attended EDS Living were requested to complete survey responses at the close of the program (Supplementary Appendix S2). Surveys were completed anonymously and electronically by REDCap. Elements of the Press Ganey, Consumer Assessment of Healthcare Providers and Systems (CAHPS), and Utah Telehealth Network patient satisfaction surveys were modified to construct the survey. Domains of interest included individual: education, satisfaction, compatibility, and attitude; technological: perceived usefulness and ease of use; and program structure: interaction, duration, and setting—virtual versus in-person. Assessment performed was based on the intention-to-treat principle.
STATISTICAL ANALYSIS
Continuous variables were summarized as mean (average) or range (minimum and maximum) where appropriate and categorical variables were reported as frequency (%). The analyses were conducted using Prism.
Results
PATIENT SURVEY DATA
A total of 102 patients completed the post-telehealth program survey between August 20, 2021, and February 11, 2022, with an EDS Living survey completion rate of 100%. The full patient questionnaire for the telehealth program is found in Supplementary Appendix S2 as a PDF version of the online form, including response options to each question or blank spaces for open-ended questions.
The patients who attended the telehealth program were mostly women (93.1%) with a mean age of 35.9 for women and 28.0 for men (Table 1). Most patients were white (84.3%), non-Hispanic (89.2%) with varying levels of higher education (Table 1). The program was conducted virtually through a secured zoom account, which allowed patients to attend from various states of primary residency. Around 59.8% of patients were from Florida with 9.8% from Georgia, 3.9% from Alabama, 5.9% from South Carolina, and 17.6% from other states (Table 1).
Patient Demographics in the Ehlers-Danlos Syndrome Living Program
For the 102 patients, who completed the program survey, the patient feedback showed an overall positive experience with the EDS Living program. Patient survey response options were “strongly disagree, disagree, neutral, agree, or strongly agree.” Patients indicated that 93.1% gained a better understanding of the chronic condition (strongly agree or agree, Fig. 3a and Table 2), 89.2% reported the program provided hope for improving (strongly agree or agree, Fig. 3b and Table 2), 88.3% stated that the program gave them the tools to improve (strongly agree or agree, Fig. 3c and Table 2), 76.5% indicated that the program addressed their specific needs (strongly agree or agree, Fig. 3d and Table 2), and 93.1% would recommend the program to others (strongly agree or agree, Fig. 3e and Table 2).
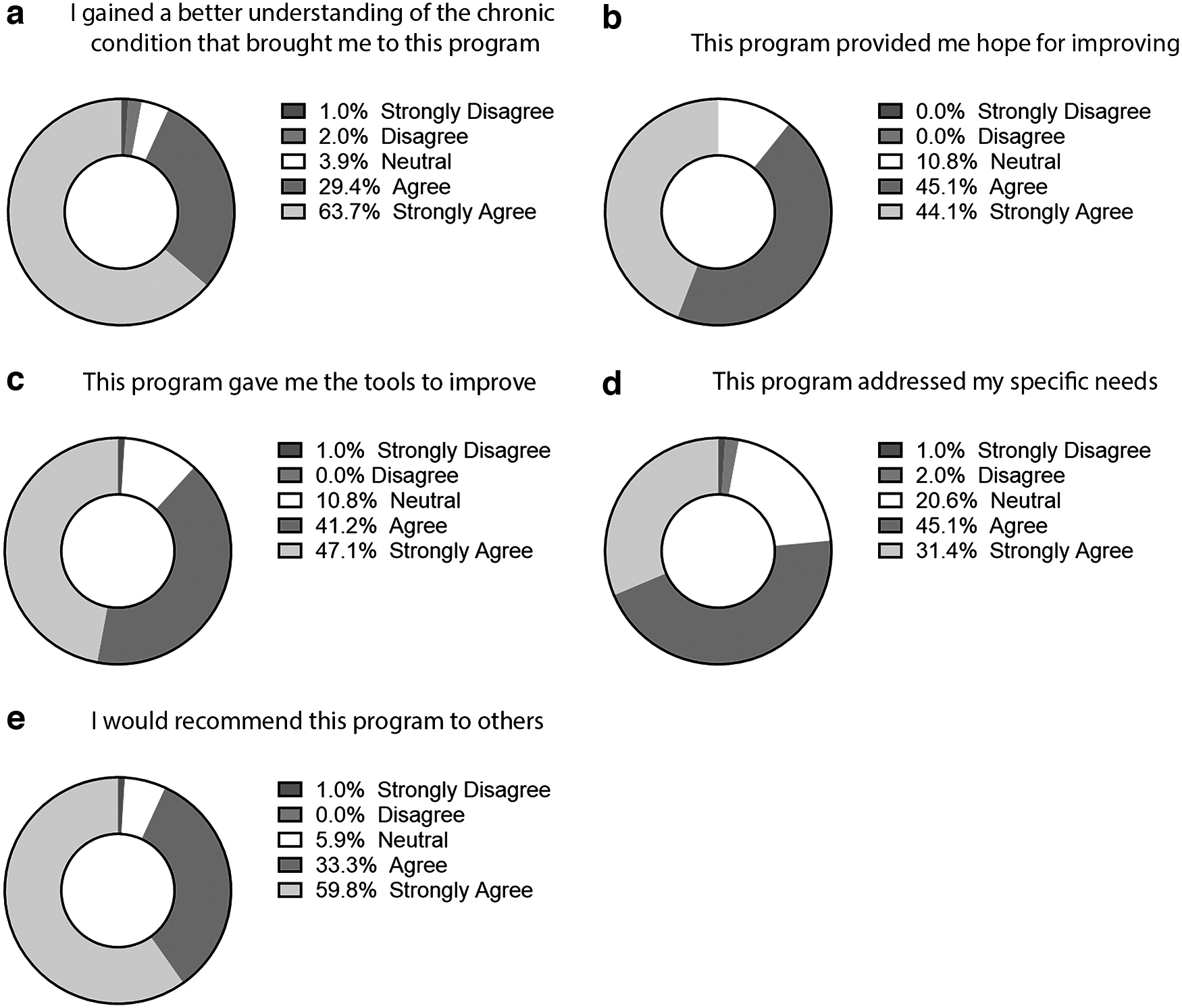
EDS Living program feedback. Patient survey responses were summarized in pie chart for each program feedback question and displayed as a % for strongly disagree, disagree, neutral, agree, and strongly agree. Questions in the survey included
Program Feedback
In addition, 92.1% found it easy to interact with the program facilitator (strongly agree or agree, Fig. 4a and Table 3), and 79.4% found it easy to interact with program members (strongly agree or agree, Fig. 4b and Table 3). Survey respondents provided additional feedback on the structure of the EDS Living Program. Most patients did not want the program to be longer (25.5%, strongly agree or agree or neutral Fig. 4c and Table 3), indicating that nearly 75% thought the program was the appropriate length. Responses indicated that 18.7% would prefer to participate in this program in-person, rather than virtually (strongly agree or agree, Fig. 4d and Table 3).
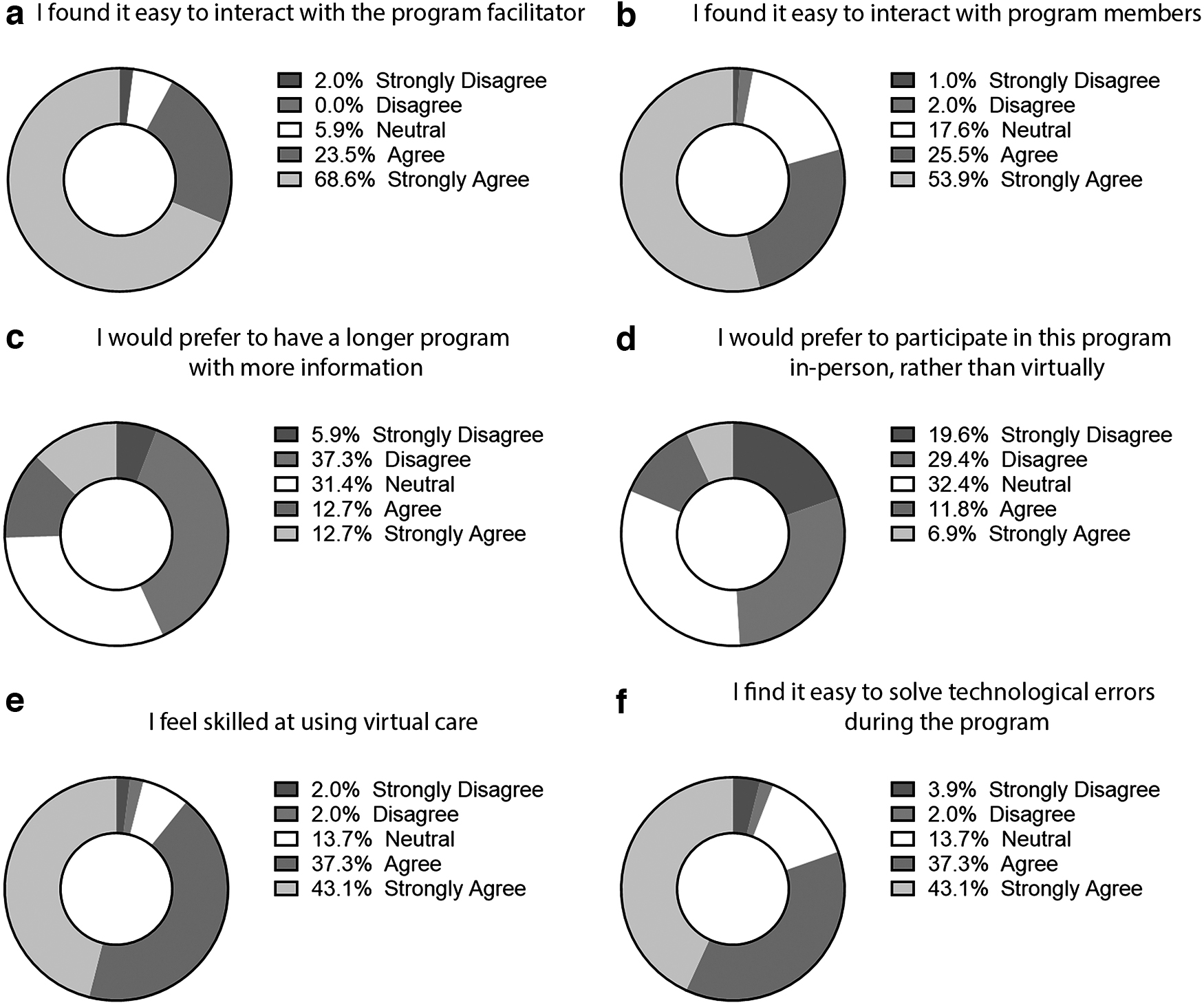
EDS Living program setup feedback. Patient survey responses were summarized in pie chart for each program feedback question and displayed as a % for strongly disagree, disagree, neutral, agree, and strongly agree. Questions in the survey included
Program Setting Feedback
The survey outlined that 81.3% of patients enjoyed the telehealth version of the program and 89.2% felt skilled at using virtual care (strongly agree or agree, Fig. 4e and Table 3) with 80.4% finding it easy to solve technological errors/challenges during the program (strongly agree or agree, Fig. 4f and Table 3). The patient-reported findings indicate that the EDS Living program provided useful knowledge and management tools for patients, fulfilling the program's objectives.
PATIENT RESPONSES
Two questions on the survey gave the opportunity for open-ended responses to provide personalized feedback about the telehealth program (Supplementary Appendix S3). The first question was “What additional topics would you like to see added to the EDS Living Program?” Many of the responses to this question included that patients wanted more information on how to coordinate care long term when they completed the program. Also, there were suggestions for specific departments/topics such as gastrointestinal issues and nutrition. The second open-ended question in the survey was “Please offer any comment/suggestion you might have for the EDS Living Program.” Most of the feedback included positive suggestions on how to help other patients and improve the program with one patient expressing a negative experience in their comments.
Discussion
According to patient responses to questionnaires, this telemedicine group treatment program is a valuable resource for patients. The indication of improved outcomes at the individual level demonstrates the role of medical knowledge and literacy for maintaining an optimistic view on handling complex chronic medical conditions. Communication from physician to patients in all forms is the basis for this transfer of knowledge. Training in communication for medical literacy has seen improvement over recent years, but has room for further improvement. 9 –11
Despite the novelty of telemedicine platforms, our results show an acceptable level of technological access for this model of communication and care. Telemedicine research is a rapidly growing field since the pandemic, and as of 2022, systematic review has revealed promising similar outcomes for the use of video telehealth compared to usual care for the treatment of chronic pain. 12 Our study supports that finding—overall patients reported improved understanding of their condition from the program.
Our cohort of patients diagnosed with hEDS/HSD serves well as a model for virtual care of chronic illnesses. Patients experience a high disease burden from hEDS/HSD, which is a chronic, complex, and limiting disease. The wide symptomatic profile leads to challenges such as obtaining a proper diagnosis, remaining functional, pain management, behavioral and mental health complications, and considerations related to risks and challenges associated with parenting as it is an inherited condition.
Therefore, the critical role of education in the treatment process cannot be overstated. When the patient has a familiarity with their condition, only then can expert care be focused at the level of the individual. As it is a multiorgan disease, requiring a multidisciplinary approach and a high level of provider experience, optimal treatment also requires patient buy-in to act on the given recommendations. For this reason, EDS Living was developed primarily as a “live” virtual program to allow real-time feedback, rather than printed or recorded material. Progress has been made through the years of implementing minimally disruptive medicine in this manner and is important to reduce treatment burden for patients with chronic disease of all types. 13 Programs such as EDS Living are able to help reduce this load.
To our knowledge, this is the first study to assess patient response to single-session treatment in a group telemedicine setting for a complex chronic disease. Prior studies with participants suffering from depression and anxiety found general improvement in patients' moods, perceived stress, and quality of life following virtual group sessions. 8 We have advanced this model to include physical illnesses as well. Other studies that addressed telemedicine and physical illnesses were smaller, education based, and without 1:1 physician counseling. 14 As this is the first study of its kind and inspired by the demands of the patients during the recent pandemic, innovation of virtual group conferencing allowed us to reach many patients, without increasing costs of travel or risk of infection, and still utilize a well-received platform of care. 10
The results provide clear implications for clinicians and policymakers. Telemedicine offered in group settings can improve accessibility for patients who seek treatment with expert providers limited in number, particularly for those who live in underdeveloped areas or have limited mobility. Telemedicine group treatment programs appear to recreate a similar bonding experience and trust as professional-led face-to-face groups. This is especially promising for chronic disease management. Other review studies conclude that telemedicine in group settings can feasibly produce outcomes similar to in-person groups, being noninferior to usual care. 5,12 Furthermore, participants still report high satisfaction rates, despite possible technological difficulties. 6 The biggest possible problem in telemedicine is the change in group dynamics that prevents the same level of engagement with professionals compared to in-person sessions.
EDS Living offers a good archetype of chronic health treatment as nurturing the group dynamism for patient bonding and recognition of associated mental illness can improve the management of physical symptom multimorbidity connected to mental health difficulties. 6,15 Described as a “hero's journey” where EDS patients have met complications in working with clinicians, multiplying symptoms, and negative psychosocial consequences, patient bonding and group dynamism are crucial. 16 Anxiety and associated somatic symptoms are the core of hEDS/HSD psychopathology. 17 This association is so strong, in fact, that there has been suggestion for refined psychiatric nosology to develop inclusive phenotypes like a neuroconnective phenotype that includes both somatic and psychological manifestations. 17
Findings from this study may promote better guidance for patients who are uncertain about embarking on group education or telemedicine treatment programs. The cause for uncertainty is justified as the effectiveness of group-based telemedicine sessions often varies from disease to disease. Results of some studies found no significant improvement for post-traumatic stress disorder (PTSD) patients, which did not significantly reduce PTSD symptoms, 18 but those suffering from type 2 diabetes showed a great improvement compared to conventional clinical care. 8,19 Group education has also demonstrated success for providers in the video conference “EDS ECHO” mentoring program, which is an online education program offered to all providers in the field of EDS through the EDS Society that aims to “move knowledge instead of people through telementoring and collaborative care with the philosophy of ‘all teach, and all learn’.” 20
A recent study of this program reported increased levels of knowledge and confidence in providing care (93% and 95%, respectively), with 59% reporting a decrease in feeling overwhelmed by hEDS/HSD, and nearly half reported a decrease in the level of frustration. 21 Clinicians participating in EDS ECHO programs know more, have more confidence in their ability to provide care, and feel energized by their participation. 21 Every patient with EDS, or any other disease, is unique so while we structured the EDS Living to be conducted in a group setting, we also recognized the need for individual counseling during the program as well. Our hEDS/HSD patients often require multidisciplinary management and referrals to specialists depending on their needs, so a 1:1 physician counseling session links education and care. This has been a great draw for our patients to have a group-coordinated, yet individualized approach in the telemedicine setting.
There are several strengths and weaknesses to our study. The strengths include high response rates to survey questions providing both quantitative and qualitative data. In relation to other studies, there is an additional strength by research focus to include both the telemedicine platform—utility thereof, combined with the impact of the material within the program itself. Study weaknesses include limited sample size, less diversity, and absence of randomization. Conclusions that can be drawn from the study are limited due to lack of control groups and pre- versus post-program patient symptom and function data.
While generally telemedicine in a group setting appears to result in positive clinical outcomes, 5,6,10 more research on a larger scale is needed to maximize the benefits of disease treatment and management through online support groups led by professionals. This can and should continue along the global coordinated efforts that have already amplified many experiences and voices of patients with chronic illnesses like hEDS and HSD. 22
Conclusion
Because of the growing health care pressure of chronic disease, we applied a virtual care model tailored to the needs of the patient as an integrated, embedded telemedicine program within a general internal medicine practice. The innovative use of virtual group counseling has been a successful model to improve care for patients with hEDS/HSD. The foundation of knowledge gained during the education session allows more time during 1:1 encounters to address individual needs and counseling equips patients to navigate adversity and treatment burden of comorbid illness.
Our survey results show that the education program has improved access and elevated the knowledge and resources for this population overall to achieve a fundamental treatment goal of improving their quality of life. As a model for group telemedicine, the program can and should be formatted for other chronic diseases. Until curative therapeutics are available, it is essential to create multidimensional, minimally disruptive, and meaningful strategies for patients living with chronic disease.
Footnotes
Authors' Contributions
D.R.T.K., J.M.G., K.A.L., J.L., A.L.L., L.M., L.S.M., A.M.S.-S., and N.J.D administered and ran the EDS Clinic and EDSLiving Program. K.A.B. and D.F. built and managed the electronic database of patient data. K.A.B. analyzed the patient data. D.R.T.K., K.A.B., and L.S.M. wrote the article. D.R.T.K., K.A.B., J.E.M., K.A.L., J.L., A.L.L., L.M., L.S.M., A.M.S.-S., N.L.D., and D.F. edited and revised the article.
Ethical Approval
Mayo Clinic IRB, except study approval (IRB no. 19-010260, approval date: November 11, 2019).
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by funding from the Mayo Clinic RACER Award to D.R.T.K., Mayo Clinic's Division of General Internal Medicine to D.R.T.K., K.A.B., D.F., and A.M.S.-S., and the Ralph E. Pounds and Kathy Olesker Pounds Fund in Research Related to Chronic Pain to D.F.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.