
Abstract
Background:
As part of a curricular change, an academic medical center implemented a medical student telemedicine clinical experience for first-year medical students in October 2020. This research is a process evaluation of the implementation of a preclerkship medical student telemedicine clinical experience.
Methods:
Patients with two or more chronic diseases were recruited from affiliated primary care practices. We monitored the recruitment and retainment of patients throughout the curriculum. We used surveys to evaluate patient, student, and primary care overall experience with the program. We tracked referrals to higher levels of care and assessed skills students' felt they practice with each encounter. We followed progression of notes through chart review as the year progressed.
Results:
Of the 408 patients contacted, 150 agreed to participate in this program (36%). Of 1,053 scheduled visits, 686 (65%) were successfully completed. Seventy-five percent of patients were seen two or more times. Nearly 70% of surveyed patients felt that the clinical experience enhanced their communication with their primary care provider, and nearly 90% stated that students were “somewhat” or “extremely” professional. The majority (97%) of students reported an “excellent” or “good” view of the medical student telemedicine clinical experience. Qualitative measures of student performance, such as note writing, showed improvement over the course of the curriculum.
Conclusions:
Our data suggest that patients, students, and primary care providers were widely accepting of the curriculum, patients were successfully recruited and retained, and students successfully practiced key clinical skills on a telemedicine platform.
Introduction
As geographic health care disparities continue to widen and as access to and quality of technology continue to improve, telemedicine will play an increasingly prominent role in the provision of health care. As of 2017, eight counties in Georgia lacked a physician of any kind. Multiple counties lacked physicians specializing in various fields including family medicine in 11 counties, internal medicine in 37 counties, pediatrics in 63 counties, and obstetrics and gynecology in 75 counties. 1 Lack of accessible health care disproportionately affects rural populations who are often sicker and older on average than in urban areas. However, with wireless networks covering more than 90% of the world's population and smartphone penetration now exceeding 80% in the United States, telemedicine promises a powerful and cost-effective way to bridge this health care accessibility gap. 2 –4
Furthermore, the emergence of SARS-CoV-2 in 2019 has dramatically accelerated the adoption of telemedicine in clinical practice. In the first quarter of 2020, telemedicine visits increased by more than 50% compared with the previous year. 5 While some of these gains may be transient, the use of this treatment modality will remain as more providers and patients adopt telemedicine technology. In anticipation of the growing relevance of telemedicine in clinical practice and to address the lack of health care access across the state of Georgia, it is critical to train future health care providers to be competent in the use of telemedicine. 5
Telemedicine is an efficient, patient-centered treatment modality that provides patients with convenient access to specialists across geographical locations. Despite growing interest, a 2017 survey revealed that only 15% of nearly 5,000 physicians reported using telemedicine in their practice. Fifty-five percent of respondents stated lack of training as their reason for not utilizing these services. Telemedicine has been proposed to increase access to care and lower health care costs. For these reasons, the American Medical Association has requested that telemedicine becomes a core competency of medical education. 6
Despite this, few medical schools have incorporated telemedicine in their preclinical curricula. In 2016, the Liaison Committee on Medical Education's (LCME's) Annual Medical School Questionnaire found that only a quarter of allopathic medical schools had implemented telemedicine training in the preclinical phase, while nearly half had implemented it into the clerkship phase. 7 There is a large geographic disparity in preclinical telemedicine implementation, with states containing many rural communities that could benefit from telemedicine having little or no preclinical telemedicine exposure. 8
Curricula involving telemedicine skills have been well received by students. A simulation-based telemedicine course developed by the Weill Cornell Medical College found that 97% of their participating students were enthusiastic about the course, 72% thought about incorporating telemedicine into their future practices, and 92% observed improvements in their telemedicine skills and comfort. 9 A similar interactive module developed by the William Beaumont School of Medicine was also well received by participating students, with 93% reporting improved telemedicine communication skills and 95% reporting improved development of differential diagnoses. 10
In one study of 17 medical schools with preclinical telemedicine curricula, it was found that 71% implemented didactic learning, 53% used patient encounters, 59% used standardized patient (SP) encounters, and 29% incorporated scholarly projects. 8 In addition, some schools combined telemedicine with interprofessional training (40%) or rural medicine (50%), emphasizing the utility of telemedicine education in these environments. 8 However, the lack of transparency in educational efforts hinders implementation of telemedicine curricula by other programs. As of 2019, only 12 out of 81 allopathic schools with telemedicine curricula offered publicly available information regarding the contents or format of their telemedicine program. 8 In addition, only eight of these schools have systematically studied and published the impact of their telemedicine training on students in the form of peer-reviewed articles. 8
In this article, we aim to augment the implementation of preclinical telemedicine training in U.S. medical schools by systematically detailing the format, components, and integration of our telemedicine program into previously existing competencies. This study was IRB approved as exempt.
Telehealth Curriculum Overview
We designed a telehealth curriculum for preclinical medical students incorporating both didactic and real patient experiences to build telemedicine competencies over 12 blocks spanning over 18 months before starting clerkship rotations. The goal of this telemedicine curriculum is to allow preclinical medical students to develop clinical and technical skills, both general and specific to telemedicine. General skills include history-taking, review of systems, physical examination techniques, electronic medical record (EMR) competency, primary care and outpatient management, assessment and plan development, note-writing, patient communication, and recognizing psychosocial factors affecting patient care. Telemedicine-specific skills include navigating the technology, virtual communication, and recognizing common complaints that can be managed through telemedicine.
These competencies were incorporated into an existing curriculum that included SP encounters, problem-based learning, and ultrasound components, allowing for a more seamless transition into the improved curriculum. Didactic materials were delivered in the form of instructional videos assigned as prework, and patient experiences were provided through a newly formed medical student telemedicine clinical experience. In the last 6 months of the curriculum, there was an overlap of medical student classes that allowed for a mentorship role to be established between entry level and second-year students that will continue for future classes.
The medical student telemedicine clinical experience was created solely for the purposes of this curriculum. We sought to identify patients with multiple chronic diseases who were willing to work with medical students and participate in a telemedicine continuity clinical experience. Patients were recruited by contacting family medicine and internal medicine providers affiliated with our institution to identify suitable candidates. A flyer was distributed to these providers to share with patients, providing background on the program and a link to enroll ( Appendix Fig. A1). Patients were informed that the clinical experience served as an educational tool for students and that the students would collaborate with their primary care physician to provide improved care. Patients received instruction before their visit on how to connect to the telemedicine platform.
Before each session, students were provided prework in the form of instructional videos highlighting a particular telemedicine competency, such as use of EMR and primary care (Table 1). Topics included scheduling and conducting a telemedicine visit, documenting a patient visit, forwarding notes to attending physicians, and performing a medical reconciliation. Asynchronous educational material covering preventative medicine and management of chronic conditions was provided for students' reference. Students were also instructed on how to perform specific examinations over telemedicine such as a spine examination, knee examination, skin examination, cardiopulmonary examination, and upper respiratory tract examination.
Curriculum Blocks and Objectives
EKG, electrocardiogram; EMR, electronic medical record; GU, genitourinary; IO, intra-osseous vascular access; IV, intravenous vascular access; POCUS, point of care ultrasound.
Students then attended an in-person session once a month to apply these competencies in practice through the medical student telemedicine clinical experience. Students were assigned specific patients 2 weeks in advance to provide students with time to review the patient's chart. Students worked in pairs to interview these patients through telemedicine, documented their interactions in the EMR, and submitted their documentation to both the patients' primary care providers and to the curriculum facilitators for review. Students were asked to focus on specific aspects of the history to complement the preclinical curriculum. Should the student's scheduled patient be unable to join the appointment, SPs were available for students to complete their encounters.
This curriculum is rooted in a compilation of standards known to effectively prepare students for residency and practice. Each week's activities are correlated with the 13 Core Entrustable Professional Activities (EPAs), guidelines established by the Association of American Medical Colleges (AAMC) detailing activities medical students should be able to perform for a successful transition to residency. 11 In addition, this curriculum meets the LCME established standards for accreditation, namely Standards 6–8, which detail the characteristics of an effective curriculum. 12 Each block is directly correlated with specific components of Standard 7, Curricular Content. By utilizing telemedicine in conjunction with existing components to satisfy these requirements, this curriculum trains preclinical medical students with versatile patient-care skills that will be effective in both clinical and virtual settings.
Perceived Barriers
Patient recruitment and retainment were the greatest perceived barrier while designing this curriculum. The use of SPs in medical education has been well established. 13,14 To provide an objective assessment of students' clinical skills, SPs are trained to behave identically during each session; however, variation is inevitable. As such, SP encounters are subjective and hinder standardization of assessments. In addition, SPs are given very narrow histories with only pertinent findings disclosed to the students. Their history and presenting symptoms may only include classic signs, which is not representative of what students will experience in practice. For these reasons, we recruited real patients from our affiliated hospitals.
Patient encounters with those who have chronic conditions provide students with a better opportunity to navigate complex histories and foster communication skills. However, the recruitment process is laborious. In addition, patients may not see the value in participating in a clinical experience that does not provide direct medical value to them. Ensuring that patients who were successfully recruited are retained is essential to reduce the resources required to continuously recruit new patients.
Another barrier was aligning the systems and diseases covered at a specific time in the preclinical curriculum to the actual complaint of the patient. Students were encouraged to focus their patient encounter on systems that aligned with the preclinical curriculum, however, this was not always possible if the patients had a specific concern they wanted to address.
A final barrier was securing primary care provider buy-in to the program, navigating concerns such as time commitment and medical liability.
Results
Data were collected between August 2020 and December 2021 with the objective of describing the initial success and challenges of implementing a preclerkship medical student telemedicine clinical experience. Endpoints included patient recruitment rates, patient retainment, patient attitudes, encounter completion and duration, skills practiced by students, and student attitudes.
Of the 408 patients contacted, 105 agreed to participate in this program (36%). Of the 1,053 scheduled visits, 686 (65%) were successfully completed. Fifteen percent of patients were removed from the curriculum due to multiple visit cancellations, challenges navigating the technology, or severe illness and death. A majority (75%) of patients seen in our medical student telemedicine clinical experience were seen two or more times ( Figs. 1 and 2 ). A small portion (10%) were new patients only seen once during the data collection period. Fifteen percent of encounters required faculty intervention due to increased acuity and complexity: 4 patients were sent to the emergency department, 13 patients were scheduled for an urgent specialty consult, and 26 patients required a 24-h primary care provider (PCP) follow-up (Fig. 3).

Patient recruitment.

Patient retainment.
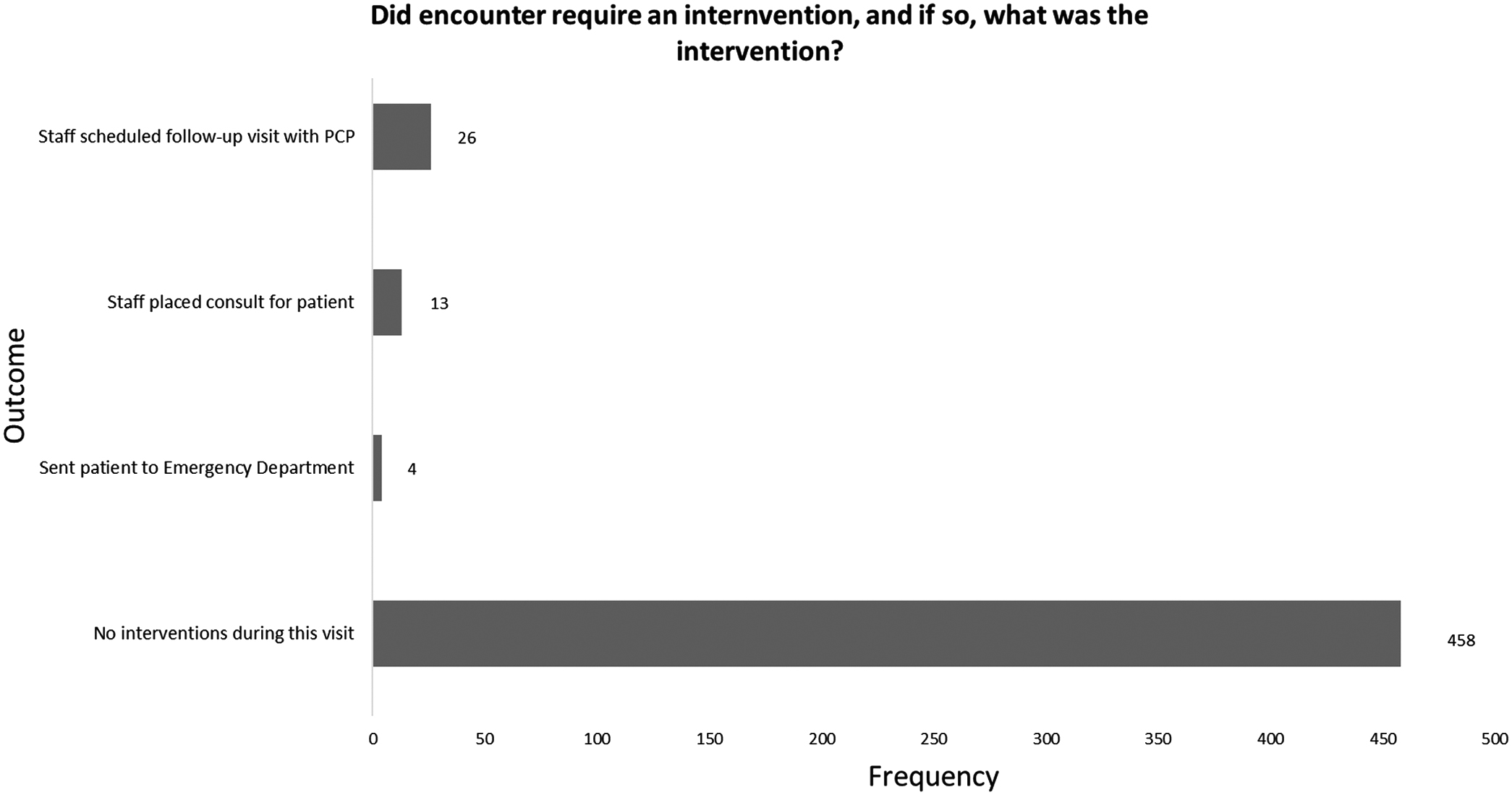
Outcomes of patient visits.
Nearly 70% of the surveyed patients felt that the clinical experience enhanced their communication with their primary care provider, and nearly 90% stated that students were “somewhat” or “extremely” professional.
The majority of patient encounters lasted between 10 and 20 min. The most frequently practiced skills by students during encounters included taking an history of present illness (HPI), reviewing medical history, performing a review of systems, and providing education to the patient (Fig. 4). Ninety-seven percent of students reported an “excellent” or “good” view of the medical student telemedicine clinical experience. Qualitative measures of student performance, such as note writing, showed improvement over the course of the curriculum, particularly in the ability to form an assessment and plan (Appendix Figs. A2 and A3).

Student skills completed during patient encounter.
Discussion
A major concern when forming the medical student telemedicine clinical experience was whether patients would agree to participate in an educational initiative that provided limited medical value, and whether we would be able to recruit and retain patients in sufficient numbers to make this intervention sustainable. Our results show that for every three patients contacted, one will agree to participate. However, patients who did participate largely found value in the medical student telemedicine clinical experience, and most of these patients were retained for multiple visits. This reduced the cost and effort associated with continued patient recruitment and use of SPs. Our data suggest that patients were largely accepting of the medical student telemedicine clinical experience.
Another concern was whether this telemedicine curriculum could be integrated with the preclinical curriculum. Patient complaints rarely aligned perfectly with specific session objectives. Students were encouraged to remain flexible and incorporate session objectives into their histories and examinations where possible. Should the patient have a complaint not related to the session's curriculum focus, students continued to refine their history taking and examination skills. This supported curriculum aims to integrate early clinical experiences and telemedicine skills. In addition, students were provided with supplemental online resources that matched their preclinical schedule, such as instructions on completing system-specific histories and examinations, interpreting common tests, and performing certain procedures. Students found value in this new curriculum, and our results show that they were able to practice a wide range of clinical skills in addition to learning how to conduct a telemedicine visit, navigate an EMR, and synthesize a concise and pertinent note.
Issues such as medical condition liability were resolved by training students to use our hospital's EMR, document a note in the chart, and send a note to the PCP for review. This allowed primary care providers to review each patient encounter at the medical student telemedicine clinical experience and follow-up with patients if necessary, further increasing communication and access to care for their patients. In addition, faculty were available on-site to assist students with immediate questions or concerns. No primary care providers terminated their participation in the medical student telemedicine clinical experience, indicating PCP acceptance of this format.
Conclusions
We implemented a preclinical telemedicine curriculum using both didactic instruction and real-patient encounters. Our data suggest that patients, students, and primary care providers were widely accepting of the curriculum, patients were successfully recruited and retained, and students successfully practiced key clinical skills on a telemedicine platform. In addition, this curriculum provided a safe way for preclinical students to interact with patients during the COVID-19 pandemic. We believe that this model can be reproduced in other preclinical medical curricula across the country creating a lasting positive impact.
Footnotes
Authors' Contributions
D.A.: Investigation and writing (original draft). L.A.: Investigation and writing (original draft). L.B.: Investigation and writing (original draft). R.B.: Conceptualization, investigation, and writing (review and editing). C.J.: Methodology and investigation. A.M.: Investigation and writing (original draft). M.L.: Supervision, conceptualization, and writing (review and editing).
Acknowledgments
We thank the staff of the Medical College of Georgia Center for Ultrasound Education for all their help and support.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.