
Abstract
Introduction:
Pancreatic cancer requires a multidisciplinary approach in a high-volume center for all the steps of the diagnostic-therapeutic course. However, the most experienced centers are not evenly distributed throughout the country causing a real “health migration” that involves patients and families with relevant economic, time, and energy costs to bear. The COVID-19 pandemic had a deep impact on surgical and oncological care and the travel limits due to COVID-related restrictions, have delayed the care of cancer patient living far from the referral centers. In this scenario, several telemedicine approaches have been proposed to reduce the distance between clinicians and patients and to allow a fast and effective access to care even for patients distant from referral centers. The aim of the study is to analyze the evidence and describe the current utility of telemedicine tool for patients with pancreatic cancer.
Methods:
We systematically searched the literature in the following databases: Web of Science, PubMed, Scopus, and MEDLINE. The inclusion criteria were article describing a telemedicine intervention (virtual visits, telephone follow-up/counseling, mobile or online apps, telemonitoring) and focusing on adult patients with pancreatic cancer at any stage of the disease.
Results:
In total, 846 titles/abstracts were identified. Following quality assessment, the review included 40 studies. Telemedicine has been proposed in multiple clinical settings, demonstrating high levels of patient and health professional satisfaction.
Conclusion:
Successful telemedicine applications in patients with pancreatic cancer are telerehabilitation and nutritional assessment, remote symptom control, teledischarge after pancreatic surgery, tele-education and medical mentoring regarding pancreatic disease as well as telepathology.
Introduction
Pancreatic cancer is one of the most lethal malignancies and is characterized by high physical and psychological supportive care needs. 1 Pancreatic cancer treatment requires a high degree of skill and expertise as well as a multidisciplinary team approach for good patient outcome. Centralization of patients with pancreatic cancer has been strongly associated with lower morbidity and mortality after pancreatic surgery as well as better long-term outcome. 2 –4 As a result, during the past decades, there was a growing trend toward referral of patients to high-volume hospitals, thus requiring them to face long journeys to receive adequate treatment, with important economic, fatigue, and time costs to bear. Furthermore, the distance also makes it difficult to arrange rehabilitation programs, provide nutritional support, and postdischarge assessment that these patients require.
Moreover, the COVID-19 pandemic has determined a reorganization of the health system, first, by committing the health system to focus all the efforts in countering the virus spread and assisting COVID-19 patients and second, by introducing travel limit. Consequently, there was a severe global reduction of routine hospital services for oncological patients and a reduction of patients' access to the referral centers.
A recent global survey from 267 centers in 37 countries showed that the majority of centers (n = 166, 62.2%) performed less pancreatic surgery because of the COVID-19 pandemic, reducing the weekly pancreatic resection rate from 3 [interquartile range (IQR) 2–5] to 1 (IQR 0–2) (p < 0.001). 5 Likewise, an Italian report from the Pancreas Institute of the University of Verona showed that in 2020, there was an overall significant reduction of pancreatic resections performed (n = 394 in 2020 vs. n = 506 in 2019) as well of outpatient visits, procedures [Endoscopic Ultrasonography (EUS), Endoscopic Retrograde Cholangio pancreatography (ERCP) and Esophago gastro duodenoscopy (EGDS) and percutaneous fine needle aspiration (FNA)], and radiographic diagnostics. 6
As a result of the overburdening of the health care system, oncological care has been reorganized and several telemedicine approaches (Web-based video consulting or telephone calls) have been proposed to reduce the distance between clinicians and patients and to allow a fast and effective access to care even for patients in distant locations. 7
Recently, the European Society for Medical Oncology during COVID-19 pandemic, proposed the telemedicine as the first-choice instrument, for patients affected by pancreatic cancer with low and medium level priority (patients who need a fast triage of newly complained symptoms or a clinical assessment), which, if necessary, can be followed by promptly patient's admittance to the clinic. 8 Given this premise, we therefore conducted this review with the aim to provide a synthesis of existing evidence of telemedicine for patients with pancreatic cancer and describe its current utility.
Methods
As a priori study, protocol was agreed upon and strictly followed by all authors. This systematic review follows the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. 9 We systematically searched the literature in the following databases: Web of Science, PubMed, Scopus, and MEDLINE through December 16, 2021.
The following algorithm was applied: “(telemedicine OR telehealth OR teleultrasound OR telepathology OR telemonitoring OR e-health OR tele-cytopathology OR telephone OR mobile application OR home health care OR home-based activities OR home-based activity) AND (pancreas cancer OR pancreas tumors OR pancreatic tumors OR pancreatic neoplasm OR pancreatic cancers).” The review has been registered on PROSPERO with the number CRD42022298767. The inclusion criteria were (1) articles describing a telemedicine intervention (virtual visits, telephone follow-up/counseling, mobile or online apps, telemonitoring) and focusing on adult patients with pancreatic cancer at any stage of the disease and (2) English language studies only. The exclusion criteria were (1) publications of conference abstracts or other non-full-text reports and (2) editorials, books, and opinions or comments. For the checklist, please refer to supplementary data.
DATA EXTRACTION
The data extracted included authors, year of publication, number of patients, time of enrollments, type of participants, stage of disease, type of telemedicine intervention, and outcomes. The studies that met our predefined inclusion criteria were screened based on title/abstract and the articles that completely fulfilled our inclusion criteria were extracted for deeper analysis.
Results
CHARACTERISTICS OF INCLUDED STUDIES
The initial search, which began on December 16, 2021, yielded 846 potentially relevant articles (241 from PubMed, 420 from Web of Science, 26 from Scopus, 159 from MEDLINE), of which the duplicate and non-English resources were omitted and excluded the articles due to the absence of comprehensiveness, relevancy, and enough analytical criteria, and finally 40 studies were deemed eligible. The studies included in the review have been published between 2003 and 2021. The Figure 1 summarizes the selection process. All included studies were organized under the following categories: (1) Rehabilitation and nutritional assessment, (2) Remote symptom control, (3) Teledischarge, (4) Patient education and medical mentoring, and (5) Telepathology.
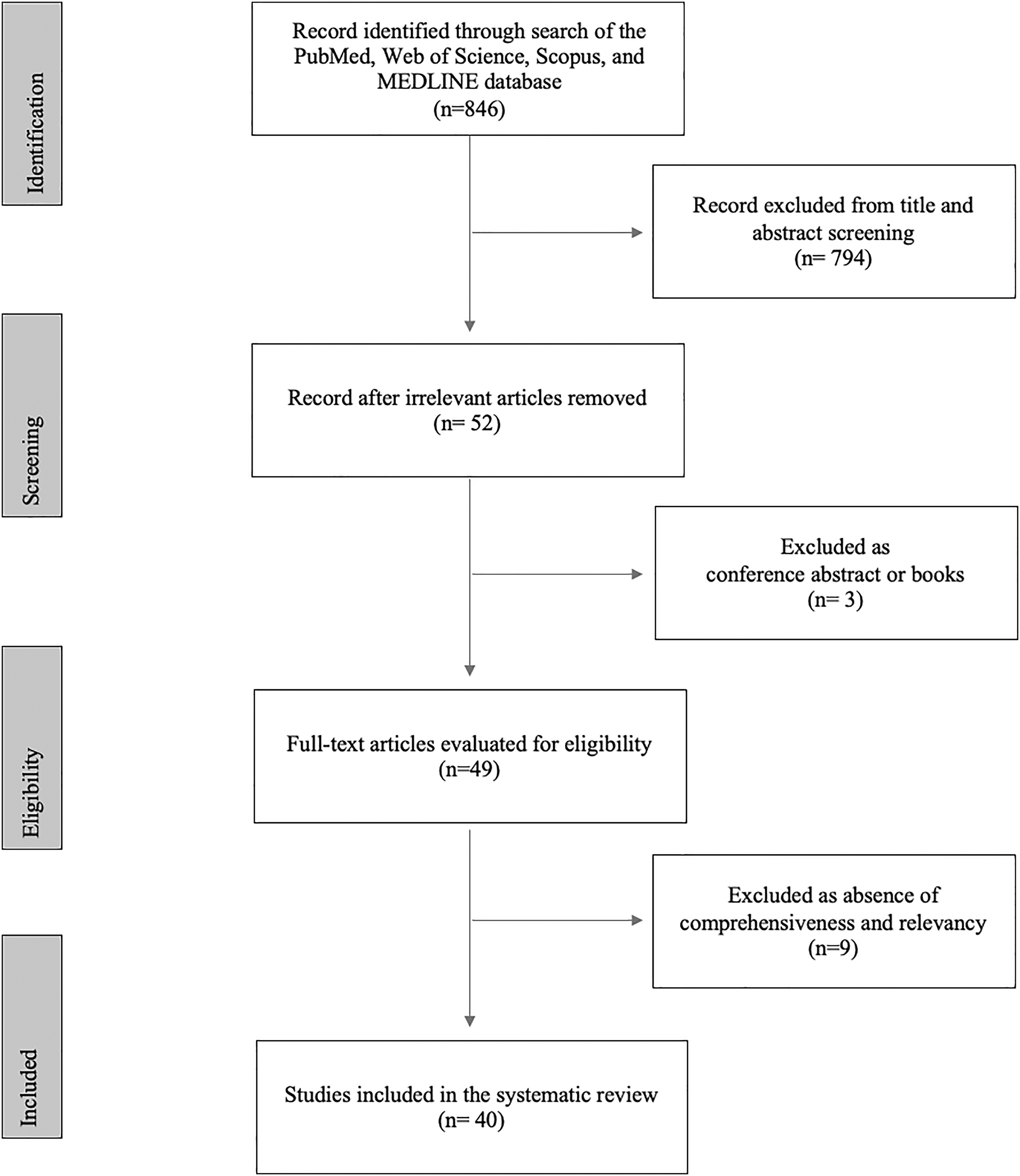
This summarizes the selection process.
TELEMEDICINE: REHABILITATION AND NUTRITIONAL ASSESSMENT
Sarcopenia, malnutrition, and cachexia are frequent in pancreatic cancer patients, especially in advanced and elderly patients, and are associated with worse prognosis and quality of life (QoL) causing patient's disability, while combinations of exercise and nutritional support might improve the functional prognosis for cachectic cancer patients. 10,11 Telemedicine has been proposed to promote recruitment and compliance of patients in a multimodal approach, including home-based exercise and nutritional support. 12 –14
This multimodal approach has been reported in the literature with a total of 16 studies focused on a nutritional intervention and home-based exercise with a telemedicine approach both for patients with advanced cancer who underwent chemotherapy, 10,11,15 and for patient candidates for surgery (prehabilitation) 16 –22 as well as for patients who underwent surgery (postsurgical resection walking program). 23 A detailed description of the data is reported in Table 1.
Reports on Telemedicine Rehabilitation and Nutritional Program in patients with pancreatic cancer
CHRT, chemoradiotherapy; CHT, chemotherapy; GI, gastrointestinal; HPB, hepatopancreato biliary; NA, not available; PDAC, pancreatic ductal adenocarcinoma.
Most of these multimodal exercise and nutritional program used the routinely collection of Patient Reported Outcome Measures (PROMs). PROMs are information concerning how symptom type and severity affect daily life as directly reported by the patient and they have the potential to identify patients with nutritional and dietary needs and provide targeted information and precise nutritional care. 15
Several rehabilitation programs have been proposed for patients with advanced pancreatic cancer. In detail, Keum et al., in randomized controlled trial evaluated the efficacy of a mobile app-based 12-week program, in 40 patients (50% mobile app users; 50% nonmobile app users) receiving chemotherapy for unresectable pancreatic ductal adenocarcinoma. This app offered (1) interactive interface with coach, (2) daily items for basic health knowledge, (3) food logging with color coding, and (4) automated feedback-based food choices. The mobile app users showed a significant improvement in the nutritional status (p = 0.001), and in the global health status and QoL scale compared to the non-app users over time (p = 0.004). 10
Likewise, the Nutrition and Exercise Treatment for Advanced Cancer home-based program showed excellent compliance and safety in 30 elderly patients (>70 years) receiving concurrent chemotherapy for advanced pancreatic (n = 6) or non-small cell lung cancer (n = 24), other than an improvement in patient's physical capacity and activity from baseline to the end of the treatment after 8 weeks. 15
A prehabilitation program exercise delivered by telemedicine for patients candidate for surgery has been suggested to reduce surgical complications, accelerate recovery, and facilitate the delivery of other necessary cancer treatments. 16 The prehabilitation program frequently provides program instruction, periodical follow-up calls to encourage adherence, compilation of a daily logs of physical activity, and objectively measurement of physical activity using accelerometers. 16 –18 Moreover, the prehabilitation may include a smoking cessation program and a stress reduction strategy 21 that has been correlated with a protective effect on physiologic decline from chemotherapy. 20 As for patients with advanced pancreatic cancer and also for patients who are candidates for surgery, the home-based prehabilitation and postresection rehabilitation program have been related to an improvement in terms of physical function and QoL. 18,23,24
Several studies reported the evidence on benefit of the home-based prehabilitation and rehabilitation program on the sarcopenia status of patients with pancreatic cancer. Indeed, pancreatic cancer patients who participated to the home-based exercise program showed a good skeletal muscle index (SMI) maintenance or a better SMI than before the start of the program. 11,15,19
About the patient's perception regarding the telematic method, patients declared that delivery of an early and intensive rehabilitation or nutritional intervention via telephone or mobile app were both largely acceptable delivery modes. 12 –14,25,26
Social support and encouragement from friends, family members, and health care providers and location (easily accessible or home-based) were positively associated with physical activity, while concomitant preoperative treatment (chemo/radiotherapy), physical issues, personal issues, distance, and lack of social support were demotivating factors. 17,26
TELEMEDICINE: REMOTE SYMPTOM CONTROL
People affected by pancreatic cancer can experience several complex symptoms, including weight loss, fatigue, pain, cachexia, and malabsorption. 1 Moreover, in the first 6 months after pancreatic surgery, patients can experience eating or bowel function problems and emotional distress along with fatigue and pain. 27 Telemedicine allows us to interact with the patients and remotely monitor their symptoms, integrating patients into health care and delivering them a personalized care. 1 The remote symptom control can be done through “PROMs” 27 –32 or “by telemonitoring.” 33 A detailed description of studies on “remote symptom control” is reported in Table 2. PROMs are information concerning how symptom type and severity affect daily life as directly reported by the patient. Those tools allow clinicians to understand the patient perspective and determine if their interventions are effective 1 and, on the contrary, allow the patients to acquire a greater enhanced symptom management and participate in cancer care. 29
Reports on Telemedicine Remote Symptom Control in Patients with Pancreatic Cancer
PROMs, patient reported outcome measures; RT, radio therapy.
Gustavell et al. tested the use of a mobile health app (Interaktor) on six patients in the first 4 weeks after discharge following pancreaticoduodenectomy (PD). The app allowed daily assessment of symptoms and access to self-care advice that includes a risk assessment model for alerts with real-time interactions with professionals. Fatigue was the most common symptom 91% (n = 128) of all the reports, while the most common alert was associated to pain in the abdomen and/or back (43%). The adherence to reporting daily symptom was on average 84% (range, 68–93%) demonstrating that the app was feasible, acceptable, and easy to use for patients after discharge. 28
In another study, Gustavell et al. also compared the QoL of patients' Interaktor utilizer with the control group, before surgery, at 6 weeks after surgery, and at 6 months after surgery. The authors showed that the Interaktor group reported fewer symptoms than the control group 6 weeks after surgery and that the use of the Interaktor app can provide support to decrease symptom burdens during the first weeks after surgery. 32
Recent progress in wearable sensor technology allows routine tracking of patient's physiologic parameters at home. Telemonitoring of symptoms by an e-health platform has been proposed for patients receiving multidrug chemotherapy [chronomodulated irinotecan, fluoro-uracil-leucovorin, and oxaliplatin (chronoIFLO4)] at home for advanced or metastatic colorectal or pancreatic cancer. This e-health platform made it possible to integrate objective [circadian rest-activity rhythm (CircAct), sleep, and body weight changes] and subjective (patient-reported outcome measures) parameter records and has been related to a good patient's compliance to telemonitoring , and also, it demonstrated a satisfactory tolerance for this multidrug chemotherapy. 33
TELEDISCHARGE
Despite the advances in surgical and perioperative care, pancreatic surgery is still associated with a high morbidity rate, which is related to prolonged hospitalization and patient's debilitation. Some adverse events after pancreatic surgery may be preexisting during hospital stay and worsen after discharge or may occur again after discharge with a reduction of patient's postoperative QoL and a delay in access to chemotherapy. Moreover, an inefficient transition from hospital care to home may cause a high rate of readmission after complex abdominal surgery. 34 To reduce barriers between patient discharged at home and the hospital and to promote a faster but safe discharge, some remote follow-up strategies have been demonstrated. 34 –37 A detailed description of studies on “Teledischarge” is reported in Table 3.
Reports on Teledischarge in Patients Who Underwent Surgery for Pancreatic Cancer
Recent evidence showed that Enhanced recovery After Surgery decreases complications, hastens recovery, shortens hospital length of stay, and reduces costs in patients who undergo PD. Lavu et al., proposed a specific “Whipple accelerated recovery pathway (WARP)” for patients undergoing PD at low-to-moderate risk of perioperative complications. WARP include precise patients' education regarding the discharge planning, a hospital program for early discharge, and a close telehealth follow-up after hospital discharge with an experienced nurse practitioner expert in pancreatic surgery recovery.
This randomized trial study showed that the WARP group (37 patients) significantly increased the number of patients discharged to home by postoperative day 5 compared with controls group (75.7% vs. 12.8%; p < 0.001), without increasing readmission rates (8.1% vs. 10.3%; p = 1.0) and overall complication rates (29.7% vs. 43.6%; p = 0.24); moreover, the WARP group showed a significant reduction of the time from operation to adjuvant therapy initiation (51 vs. 66 days; p = 0.005) and hospital cost ($26,563 vs. $31,845; p = 0.011). 36
Similarly, Katz et al., proposed a comprehensive “Tele-Discharge” protocol to 15 patients after pancreatectomy. In the study, all patients participated in two scheduled and an unlimited number of unscheduled virtual clinical encounters after discharge, focused on medication review, inspection of the surgical incision and drains, and treatment disposition. The authors showed that this health approach for patients undergoing complex surgery for pancreatic cancer is practicable, relatively inexpensive, associated with high patient satisfaction, and may prevent the worsening of early adverse event after surgery. 37
Ceppa et al. planned an innovative model called Project Re-Engineered Discharge (RED) which provides a “Readmissions team with a discharge coach” to reduce complications and readmission rate after pancreatectomy. The Project RED was based on a precise discharge plan before discharge, on patient's education about principal diagnosis and a telephone reinforces of the discharge plan within 3 days of discharge. The authors showed that during the 5-year study, the development of a discharge team and the introduction of Project RED caused a 30-day morbidity reduction from 57% to 46%, and reduction in 30-day all-cause readmissions from 23% to 11.5% (p = 0.001). 35
Acher et al. have projected a Coordinated Transitional Care program for 212 patients who had undergone pancreatic surgery based on a phone transitional care protocol. Patients enrolled in the study received about 1 call every 5 days and most of the call resolved discrepancy of postdischarge medication reconciliation. In line with the other studies, patients showed a high participation in this program with <1% refusals. 34
TELEMEDICINE: PATIENT EDUCATION AND MEDICAL MENTORING
Patients with cancer require a significant amount of information about their condition and most of them wish to receive both negative and positive health information. Cancer patients have indicated that they are willing to receive information from multiple sources, including online material, if this information is easily accessible. Telemedicine has been demonstrated to be a useful method to educate patients about their health situation, help making them part of the decision-making process, and improve the patient's ability to self-manage symptom or therapy side-effects. 38 Moreover, telemedicine could also be useful as a method to disseminate prevention-related information such as the genetic screening in pancreatic cancer patients.
Hamilton et al., 39 described an innovative mainstreaming genetic testing model for 1,054 patients with ovarian, prostate, or pancreas tumors. The study consisted in a multigene panel testing with standardized pretest patient education, and genetic counselors delivered results and post-test genetic counseling via telephone. 40
Another study performed a website enrollment (
In addition, telemedicine has been used to promote the diffusion of medical information among health professionals. The Pancreas Institute of the University of Verona has proposed an app (iCyst) to diffuse the existing pancreatic cystic neoplasm (PCN) guidelines. In addition, this study explored which specific guidelines were mostly followed for the management of PCNs. 42
TELEPHATOLOGY
Progress in digital imaging and technology has made the use of telecytopathology possible, which allows to transmit diagnostic images of specimens to a remotely located cytopathologist. It is currently proposed for the assessment of specimen adequacy, primary diagnosis, or for diagnostic consultation in second opinions and it could be performed in a static way, with whole slide imaging, and dynamic real-time. 43 –46
Several studies have investigated the concordance between a specimen diagnosis of pancreatic cancer remotely transmit to a pathologist by telepathology and conventional microscopy with encouraging results in term of similar diagnostic accuracy, sensitivity and specificity in both groups, nevertheless are preliminary studies, non-randomized and without a solid statistical analysis. 4,43
Discussion
The increasing use of telemedicine has piloted a new era of patient-focused cancer care through technology-assisted interventions. Thanks to medical progress, pancreatic cancer patients experienced a better survival, and the treatment focus has also shifted toward optimal control of adverse symptoms and improving physical and mental status. 23 Besides, several studies are focused on patient benefits beyond clinical and cost-effectiveness advantage and this review showed to elevate patient's compliance and participation to telemedicine approach in the remote symptom control, virtual rehabilitation, and nutritional program. 25,33
Moreover, the home-based nutritional and rehabilitation program showed a benefit in terms of QoL and physical function in patients with different stages of pancreatic cancer. 16 –21 The rapid change in health approach related to COVID-19 has improved the e-health approach, which has as its main objective to provide a reduction of distance between patients and clinicians and between clinicians themselves. Telemedicine supply patient education providing useful information regarding pancreatic cancer as well as a video consultation 38,40 other than disseminate guidelines and medical information for the clinical practice, and this is especially useful in a complex pathology such as pancreatic cancer, which requires a specialized approach. 42
Telemedicine, thanks to the large diffusion of technology, has the possibility to vehicle useful information regarding modifiable risk factors for pancreatic cancer as diet, tobacco-use and obesity, and to contribute providing the enhanced program of preventive medicine, which need to be prioritized in modern health care. To promote this telemedicine preventive program, a series of innovative strategies and policies need to be implanted. For instance, a development of a prevention app, which send periodic notifications and reminder to play sports, stop smoking, and eat healthy food, could be a valid and smart method of cancer prevention especially in younger age group who are affected by “early onset pancreatic cancer”, which has been associated to obesity and tobacco use.
Furthermore, Telemedicine is an effective method of transferring surgical knowledge and skills from an experienced surgeon to a young one and to guide him/her in a surgical procedure, in which he/she had minimal experience. Several reports have described the use of telementoring in various surgical subspecialities, including neurosurgery, urology, and vascular surgery, while few data are available regarding pancreatic surgery, probably because of the high technical skills required to perform this type of surgery. 47,48 Nevertheless, it is expected that these limits in the telementoring in pancreas surgery are likely to be overcome in time as technology improves.
However, the integration of telemedicine in cancer care requires an extensive staff and patient education, platforms easy to use to facilitate video and audio communication and a proper training to guarantee a professional tele-consult that goes beyond a simple video call with a patient. Although this review highlights that the telemedicine approach is spreading in the different aspect of pancreatic cancer treatment and several studies have documented the acceptability and feasibility of such e-health program, the available evidence for the effectiveness of telemedicine in patients with pancreatic cancer are still limited and most studies are still descriptive. Further studies are necessary to facilitate the implementation of this new health approach and to establish how to make the best use of telemedicine in health care, especially after the pandemic.
Footnotes
Disclosure Statement
We have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.