
Abstract
Objective:
Older adults are generally less proficient in technology use compared with younger adults. Data on telemedicine use during the COVID-19 pandemic in older persons with type 1 diabetes (T1D) and the association of telemedicine with the use of diabetes-related technology are limited. We evaluated care delivery to older adults compared with younger adults with T1D in a prepandemic and pandemic period.
Methods:
Data from electronic health records were evaluated for visit types (in-person, phone, and video) from two sequential 12-month intervals: prepandemic (April 2019–March 2020) and pandemic (April 2020–March 2021).
Results:
Data from 2,832 unique adults with T1D were evaluated in two age cohorts: younger (40–64 years) and older (≥65 years). Half of each group used continuous glucose monitoring (CGM), whereas 54% of the younger and 37% of the older cohort used pump therapy (p < 0.001). During the pandemic compared with the prepandemic period, visit frequency increased in both the younger (0.65 vs. 0.76 visits/patient/quarter; p < 0.01) and older (0.72 vs. 0.80 visits/patient/quarter; p < 0.01) cohorts. During the pandemic, older adults used more phone visits compared with younger adults (48% vs. 32%; p = 0.001). Patients using either pump therapy or CGM were more likely to use video visits compared with phone visits in both younger (41% vs. 24%; p < 0.001) and older cohorts (53% vs. 42%; p < 0.001).
Conclusions:
Adults using diabetes-related technologies, independent of age, accessed more video visits than those not using devices. Telemedicine visits appeared to maintain continuity of care for younger and older adults with T1D, supporting the future of a hybrid-care model.
Introduction
The use of telemedicine services offers opportunities in the management of chronic conditions such as diabetes with its potential to expand access to care. 1 Telemedicine services carry potential opportunities to expand access to care and reduce costs. However, telemedicine also carries limitations owing to the lack of physical exam and laboratory data, which are instrumental for clinicians to assess chronic health conditions and guide therapy. Older people who are at higher risk of health deterioration may be less proficient in using new technology and/or lack the right equipment (Wi-Fi connection, smart devices, and computer), which may impair their ability to use and benefit from telemedicine encounters. 2,3
Recently, a few studies have assessed telemedicine's impact on clinical outcomes and economic benefits for persons with type 1 diabetes (T1D), supporting telehealth use. 1,4,5 However, the implementation of telemedicine has been slow because of differences in coverage across insurers and states, and other hurdles to establishing routine telemedicine use within health care systems. 6 Moreover, the benefit of telemedicine as a care delivery method in older persons with T1D has not been studied.
The advent of the COVID-19 pandemic imposed a rapid shift in the use of telehealth, and created a “natural experiment” for the rapid deployment of telehealth to all patients, independent of age, preference, technical proficiency, and/or previous use of such technology. 7
Older adults are often considered less proficient in the use of newer technologies compared with younger adults. 3,6 Moreover, older adults with T1D are a subgroup of older adults with especially unique health care needs owing to the self-care demands of T1D. 8,9
The use of insulin pumps and continuous glucose monitoring (CGM) devices, have proven to be beneficial in both younger 10 and older adults in improving glycemic control and reducing hypoglycemia. 11,12 However, the use of diabetes-related technologies in older persons with T1D is lower than in younger adults with T1D. 13,14 Similarly, it is likely that the use of telehealth services may also vary between younger and older adults with T1D. There is an opportunity to evaluate telehealth use in older compared with younger adults with T1D during the COVID-19 pandemic and whether there are any associations between the use of diabetes-related technologies and modality of telehealth.
Events during the pandemic offered a unique opportunity to assess the frequency of telehealth use as a clinical care delivery method compared with in-person visits prepandemic in adults with T1D and permitted the comparison of visit frequency between younger and older adults. Furthermore, we speculated that comfort with use of diabetes technologies might favor use of telehealth, so we compared telehealth use between diabetes device users and nonusers in both younger and older cohorts of adults with T1D. The aim of this retrospective analysis of electronic health records (EHRs) was to assess the utilization of the telehealth (video and phone visits) compared with in-person visits in younger adults (40–64 years) and older adults (≥65 years) with T1D and the relationship between the type of telehealth visits and use of diabetes-related technologies.
Methods
Institutional Review Board approval was obtained to perform this retrospective analysis and all data were de-identified.
We used data from EHR from Joslin Diabetes Center, a tertiary health care facility. The EHR from the adult diabetes clinic provided data from April 1, 2019 to March 31, 2021. Eligibility criteria included adults, aged ≥40 years, who were seen at least once in the adult clinic during the prepandemic period from April 1, 2019 to March 15, 2020, and at least once in the pandemic period from April 1, 2020 to March 15, 2021. The 2-week period from March 15 to March 31, 2020 was excluded because of the urgent transition from in-person to telemedicine visits with the start of quarantine and expected delays in setting up the EHR system to account for visit type, leading to discrepancies in appointment coding during this time. The same 2 weeks were excluded in 2021 to allow for time matching of the prepandemic and pandemic periods. Additional criteria for inclusion were a diagnosis of T1D (defined by International Classification of Dieases [ICD] 10 codes E10.XX), duration of diabetes ≥1 year, and receipt of one or more insulin prescriptions. Exclusion criteria included type 2 diabetes, dysglycemia codes, and/or pregnancy.
During the pandemic period, there was rapid introduction of virtual care that began via telephone, which was followed by video telemedicine visits once a Health Insurance Portability and Accountability Act-compliant telemedicine video platform became available to the Joslin clinic. Thus, during the period between April 2020 and June 2020, almost all telemedicine visits were via phone. In late summer 2020, in-person visits were re-introduced on a selective basis to a limited number of patients to avoid overcrowding. The in-person visits were for individuals for which outpatient visits were necessary, for safety.
We extracted sociodemographic variables (age, gender) and clinical variables from the electronic medical record, including duration of diabetes, characteristics of diabetes management (multiple daily injections [MDI], insulin pump [pump]), and modality of glucose monitoring (self-blood glucose monitoring [SMBG], and CGM); however, insurance, income, and travel data were not available.
We assessed clinical appointment status with respect to kept or missed appointments during the prepandemic and pandemic periods. Clinical appointments were defined as scheduled appointments with a member of the diabetes team, including either a nurse practitioner or medical doctor. Kept appointments were divided by: in-person, phone, and video visits. Missed appointments were defined as scheduled appointments for which the patients did not cancel before the scheduled appointment time. Total number of appointments per patient per year and per quarter were determined, as the latter calculation was aligned with the American Diabetes Association guidelines for visits every 3–6 months 15 and per Medicare regulations every 3 months for older, insulin pump-treated patients. For all appointments, whether kept or missed, we extracted the scheduled date as well as the modality of visit (in-person, phone, or video).
Data were analyzed using STATA, version 15.0. Data are reported as means, standard deviations, percentages, and confidence intervals (CIs), as appropriate. The analyses included stratification by age: younger adults aged 40–64 years and older adults aged 65 years and older. We examined the differences between appointment types (in-person, phone, or video) across three key attributes: (1) age: younger adults versus older adults; (2) time: prepandemic versus pandemic; and (3) diabetes management methods: pump versus MDI and CGM versus SMBG and the various combinations. Comparisons between the attributes are expressed using independent t-tests for continuous variables and chi-square tests for categorical variables. Time-series bar charts depict group differences graphically. A type 1 error of 0.05 was used in these analyses with no correction for multiple comparisons, as these were a priori hypotheses.
Results
We identified 2,832 unique patients, aged ≥40 years, with T1D, including 1,968 younger adults 40–64 years of age and 864 older adults ≥65 years of age, 69% and 31%, respectively, of the study sample. Younger adults (52% women) had a mean age of 52 ± 7 years and older adults (53% women) had a mean age of 72 ± 6 years. Table 1 provides demographic and clinical characteristics of the two cohorts. Half of both the younger and older groups used CGM, whereas 54% and 37%, respectively, received pump therapy (p < 0.001).
Characteristics of Adults with Type 1 Diabetes Who Had ≥1 Visit in the Prepandemic Period April 1, 2019–March 15, 2020, Divided by Younger Adult (Age 40–64 Years) and Older Adult (Age ≥65 Years) Cohorts
Note: Data are expressed as either (mean ± SD) or percentage (number).
Younger adult versus older adults device use. Pearson's chi-squared: p < 0.001.
CGM, continuous glucose monitoring; MDI, multiple daily injection; SD, standard deviation; SMBG, self-monitoring blood glucose.
First, we examined visit frequency and visit types in the prepandemic and pandemic periods in both the younger and older adult cohorts. The total number of visits (in-person, phone, and video) for younger adults was 3,697 during the prepandemic year and 3,907 during the pandemic year. The total number of visits for older adults was 1,869 during the prepandemic year and 1,922 during the pandemic year. In both cohorts, the number of visits/patient/quarter increased from the prepandemic to pandemic periods (younger adults: 0.65 vs. 0.76 visits/patient/quarter; p < 0.001; older adults: 0.72 vs. 0.80 visits/patient/quarter; p < 0.001). The number of visits per patient per quarter was higher in the older adult cohort compared with the younger adult cohort during both the prepandemic period (0.72 [CI, 0.7–0.74] vs. 0.65 [0.63–0.67] visits/patient/quarter; p < 0.001) and pandemic period (0.80 [0.78–0.82] vs. 0.76 [0.75–0.77] visits/patient/quarter; p = 0.001).
As expected, in the prepandemic period, almost all the visits were delivered in-person in younger as well as older adults (0.63 [0.61–0.65] vs. 0.71 [0.69–0.73] visits/patient/quarter in the younger vs. older cohorts; p < 0.001) with very few phone and video visits (Table 2). During the pandemic period, use of phone and video visits immediately and dramatically increased in both age groups. However, older adults used more phone visit compared with younger adults (0.39 [0.37–0.41] vs. 0.28 [0.28–0.28] visits/patient/quarter; p < 0.001); in contrast, younger adults used more video visits compared with older adults (0.39 [0.37–0.41] vs. 0.31 [0.29–0.33] visits/patient/quarter; p < 0.001) (Table 2) during the pandemic period.
Number of Kept Visits and Visit Types in the Prepandemic and Pandemic Periods in Adults with Type 1 Diabetes, Divided by Younger Adult (Age 40–64 Years) and Older Adult (Age ≥65 Years) Cohort
Note: Pandemic period younger versus older adults chi-squared.
Younger adults prepandemic versus pandemic t-test, p < 0.05.
Older adults prepandemic versus pandemic t-test, p < 0.05.
Pandemic period younger versus older adults t-test, p < 0.05.
Next, we examined the distribution of kept visits by scheduled visit type, including in-person, phone, and video visits, in the prepandemic and pandemic periods. As expected, during the first 3 quarters of the prepandemic period, patients in both age groups completed almost all visits in-person, with similar rates between the younger (97%) and older (98%) cohorts (p = 0.14) (Table 2; Fig. 1). However, in the fourth quarter (January–March 2020) compared with the first quarter of the prepandemic period, there was a small but significant increase in the proportion of visits conducted by phone in both age groups, 0% versus 11% (p < 0.001) in younger adults and 0% versus 9% in older adults (p < 0.001).
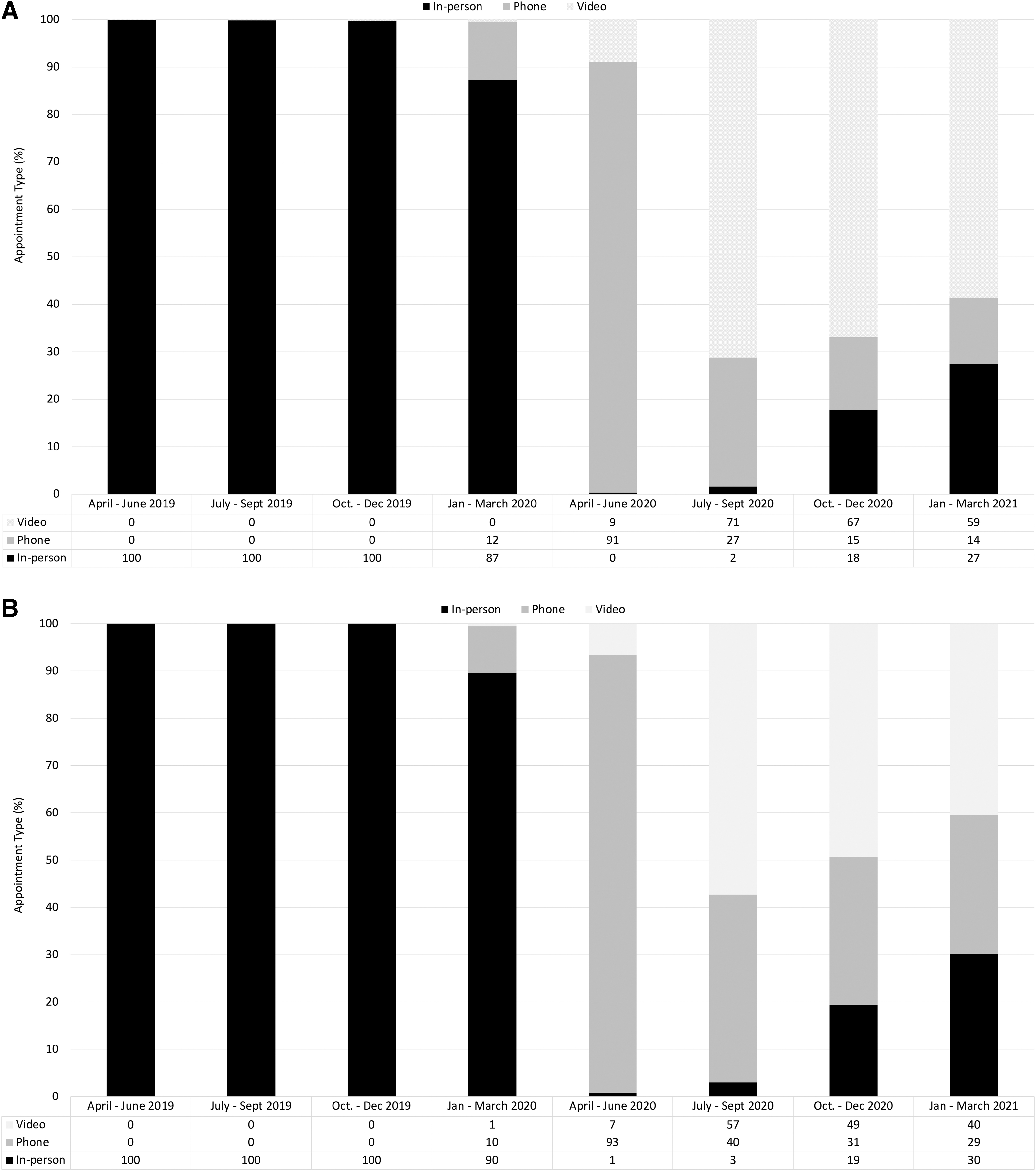
Following the introduction of restrictions at the start of the COVID-19 pandemic, in-person visits were immediately curtailed for both younger and older adults, as evident in the first quarter of the pandemic period, April–June 2020. Initially, the most commonly used method of care delivery was by phone calls in both age groups with no in-person visits per lockdown guidance. In the second quarter of the pandemic period (July–September 2020), there was a substantial increase in the use of video visits, given implementation of a robust video telemedicine platform, along with the return of some in-person visits, resulting in a substantial reduction in phone visits for both the younger and older adults. In the third (October–December 2020) and fourth (January–March 2021) quarters of the pandemic period, the proportion of phone visits further decreased to 15% in younger adults and 30% in older adults (p < 0.001), mainly owing to a greater proportion of encounters occurring in-person.
Overall, however, video visits represented the most popular modality for care delivery for both the younger (56%) and older (41%) cohorts (p < 0.001) (Fig. 1). In general, during the 12-month pandemic period, older adults compared with younger adults had more phone visits (48% vs. 32%; p < 0.001), fewer video visits (42% vs. 52%; p < 0.001), and fewer in-person visits (10% vs. 16%; p = 0.03) (Table 2).
Next, we examined visit type (in-person, phone, and video) according to use of diabetes-related technologies, including insulin pumps and CGM, in both the younger and older adult cohorts. During the first quarter of the pandemic period, visit type did not differ by management modality, likely owing to the near universality of phone visits, by necessity. However, visit type subsequently differed by management modality. There was a significant difference in visit type when comparing the first and fourth quarters of the pandemic period, with greater use of video visits in both the younger and older adults who were using diabetes devices (insulin pump therapy and/or CGM) ( Fig. 2A, B ). Furthermore, younger adults using MDI and SMBG, compared with those patients using pump and SMBG had statistically significantly more phone visits (27% [23–31] vs. 9% [7–11]; p < 0.001), whereas the former used video visits less compared with younger adults treated with pump and/or CGM devices (57% [53–61] vs. 70% [68–72]; p = 0.002) (Supplementary Fig. S1).
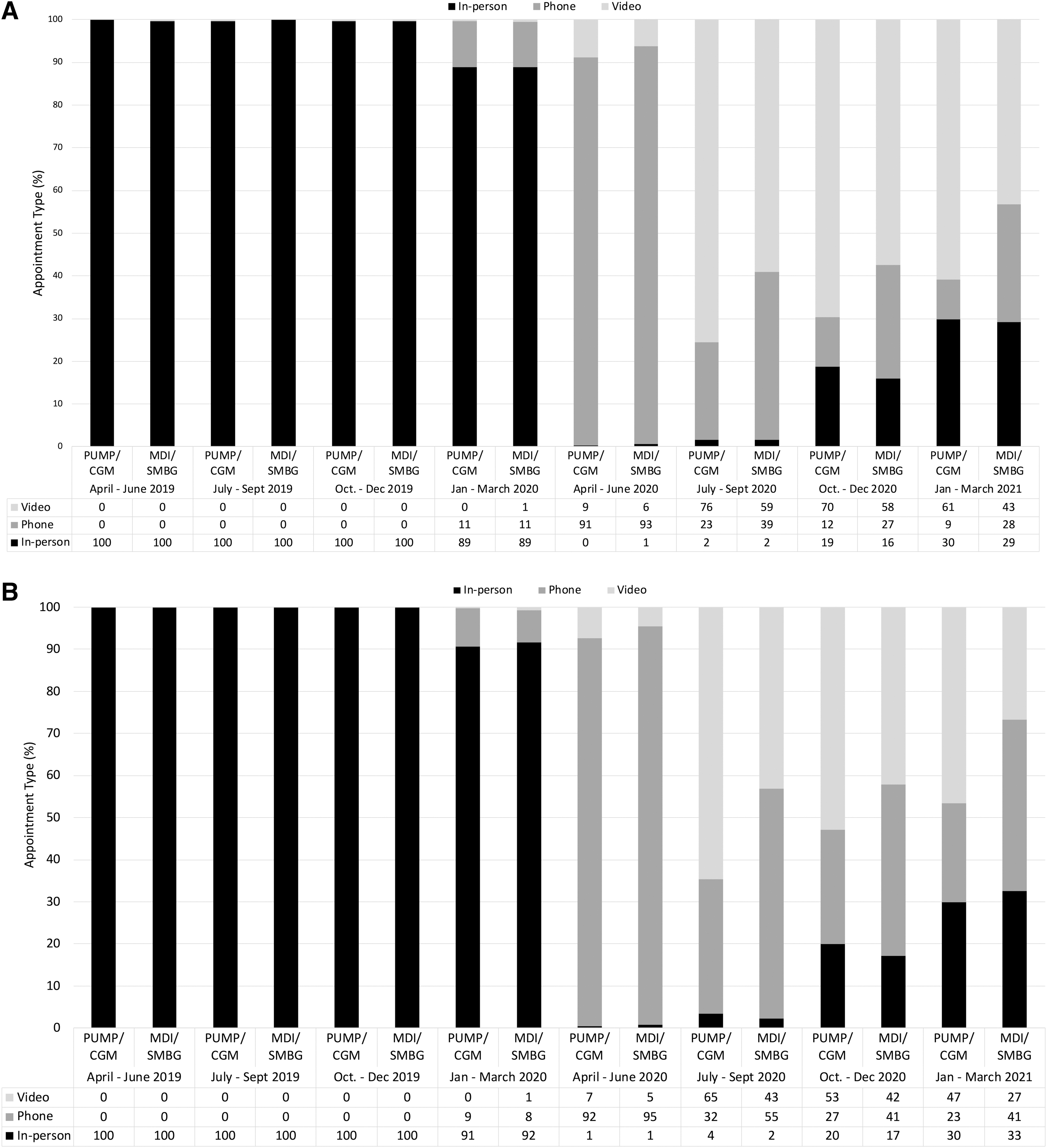
Similarly, older adults managed with MDI and SMBG, compared with those managed with pump and SMBG, had more phone visits (41% [35–47] vs. 24% [16–32]; p = 0.04) (Supplementary Fig. S1), whereas the former older adults used fewer video visits compared with pump and CGM users (42% [36–48] vs. 53% [44–62]; p = 0.04). In addition, the number of overall kept appointments during the pandemic period compared with the prepandemic period was greater in older adults using CGM (59% vs. 55%; p = 0.046), whereas there was no difference among older adults using pump (p = 0.06).
Next, we examined the total number of visits delivered during the pandemic period to older adults using insulin pump compared with older adults using MDI, the former group had a greater number of visits, as expected per Medicare requirement (0.79 [0.77–0.81] vs. 0.74 [0.73–0.75] visits/patient/quarter; p < 0.001).
Finally, we examined the number of missed appointments during the prepandemic and pandemic periods in the younger and older adult groups, and whether the use of telemedicine was associated with a reduced frequency in missed visits. Of note, the frequency of missed appointments was higher in younger adults compared with older adults in the prepandemic period (0.09 [0.06–0.12] vs. 0.05 [0.01–0.09] per visits/patient/quarter; p < 0.001), along with a pattern of greater missed visits in the pandemic period (0.10 [0.07–0.13] vs. 0.08 [0.08–0.08] per visits/patient/quarter; p < 0.002). Missed appointments increased significantly in older adults in the pandemic period compared with the prepandemic period (0.08 [0.08–0.08] vs. 0.05 [0.01–0.09] visits/patient/quarter; p < 0.001). In the older adult cohort, missed appointments did not associate with pump or CGM use. Most of the missed appointments during the pandemic period occurred for phone and video visits rather than in-person visits for both younger and older adults (Table 3).
Number of Missed Visits Overall and According to Scheduled Visit Type in the Prepandemic and Pandemic Periods in Adults with Type 1 Diabetes, Divided by Younger Adult (Age 40–64 Years) and Older Adult (Age ≥65 Years) Cohort
Note: Pandemic period younger versus older adults chi-squared.
Younger adults prepandemic versus pandemic t-test, p < 0.05.
Older adults prepandemic versus pandemic t-test, p < 0.05.
Pandemic period younger versus older adults t-test, p < 0.05.
Discussion
The results of our study of ∼2,000 younger adults and ∼900 older adults with T1D show that telemedicine was not inferior to in-person visits with respect to maintaining continuity of care. Older adults used more phone visits compared with younger adults; however, current use of diabetes-related technologies, such as an insulin pump or CGM was associated with greater use of video visits compared with phone visits during the pandemic period for both age groups. Finally, older adults tended to miss less appointments compared with younger adults, independent of insulin delivery method. To our knowledge, this is one of the largest cohorts of older adults with T1D reported during the pandemic regarding their use of telemedicine.
Our findings are consistent with the data in the literature from a systematic review of the use of telehealth in older adults, which identified factors that influence the use of telemedicine as being the individual attitude toward technology, the proficiency and availability of technology, social support for the use of technology, and trust in the use of technology among others. 16 Among the barriers on the use of technology are the need for more time for education and support, 17 as well as insurance coverage, 18 which were not captured in our data set.
Of interest, we found that the total number of visits delivered during the pandemic period increased in both age groups. This finding suggests that telemedicine is a viable and possibly preferable care delivery modality to maintain continuity of care in adults with T1D aged 40 and older. These data are consistent with a retrospective chart review study from the Veterans Health Care system in which telemedicine was associated with increased adherence in a small sample of patients with T1D (N = 32), and resulted in time and cost savings compared with in-person visits. 19
It is especially important to maintain continuity of care for older adults with T1D, given their many unique needs related to long duration of disease with high risk for hypoglycemic unawareness, 14,20 multiple comorbid conditions, potential cognitive decline, 21 and questionable comfort with use of up-to-date technologies, 3 in general, and diabetes technologies, in particular. 21,22
In our cohort, older adults used more phone visits overall compared with the younger adults, even when later in the pandemic period; video visits were the preferred method of delivery of care. This observation is consistent with a recent analysis of phone and video visits in two geriatric clinics during the early COVID-19 pandemic, where the use of phone was similarly more common than video visits. 23,24
The preference of using phone compared with video visits by the older adults may be explained by different proficiency in the use of technology and/or socioeconomic disparities as shown in a recent systematic review on satisfaction of older adults with telemedicine. 25 This preference may be the resulting lack of ability to use and/or having the proper equipment to perform video visits. 4,6,24
Such data are important to consider by policy-makers when considering whether to pay for telemedicine via phone calls in the older adult population.
In our cohorts, the use of insulin pumps was greater in the younger adults (54%) compared with the older adults (37%), consistent with other data, 26 whereas the use of CGM was similar between the younger (50%) and older (50%) cohorts. This observation highlights how CGM uptake has increased dramatically in the past few years, especially in the older population, following universal Medicare coverage along with studies showing benefit of CGM use in this frail population. 11,12 Of note, those patients, both younger and older, using diabetes-related technologies also accessed more video visits than those not using technologies; patients in both age cohorts treated only with MDI and SMBG used more phone visits. These findings suggest that persons using diabetes technology are more likely to adapt to using video telemedicine technologies, indicating that they are more likely to possess the proper equipment to perform video visits. Of note, although smart phones and/or computers can be used for video visits, these technologies are also used to upload or share both pump and CGM data.
Of interest, older adults missed fewer appointments compared with younger adults in the prepandemic period with a similar trend for fewer missed appointments during the pandemic period. One of the reasons for fewer missed appointments prepandemic for the older adults may relate to the requirement by the Centers for Medicare and Medicaid Services for timely visits every 3–6 months, for ongoing pump, and CGM coverage, respectively. 27 Moreover, older patients may have fewer competing life demands than younger adults, permitting them to keep their diabetes appointments.
The limitations of this study include the retrospective, electronic chart review nature of the study, performed at a single tertiary diabetes center from the Northeastern United States, mostly representative of a white, non-Hispanic, English-speaking population. These analyses lack information regarding insurance coverage, household income and travel time, as well as outcomes of care delivery; and these topics remain an important area for future research. Furthermore, the use of diabetes-related technologies might be higher in our cohort than in the general U.S. adult population with T1D, given the highly specialized nature of our center. 13 Nonetheless, these data provide important information regarding the viability of telemedicine for care delivery in both younger and older adults with T1D.
Telemedicine visits during the COVID-19 pandemic preserved continuity of care at a time of extraordinary disruption for younger and older adults with T1D, although there appeared to be differences in the modality of telehealth care delivery. Patients using diabetes-related technologies, independent of age, were able to access more video compared with phone visits, suggesting that use of any technology facilitates use of other technologies.
Further studies are needed to understand the potential barriers and enablers of telemedicine and its impact on glycemic parameters in persons with T1D, especially older adults.
Conclusions
In conclusion, telemedicine offers an important alternative to in-person visit for diabetes management and appears accessible even for older adults, supporting the need to maintain its reimbursement. Future studies are needed to investigate clinical outcomes associated with telemedicine use.
Footnotes
Acknowledgments
Data were presented virtually at the 14th International Conference on Diabetes Technologies and Treatments (ATTD 2021) June 2–5, 2021 and the 82nd Scientific Sessions of the American Diabetes Association (ADA) June 25–29, 2021.
Authors' Contributions
E.T. had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design: E.T., A.A., L.L., M.M. Data acquisition, analysis, and interpretation: E.T., A.A., L.L., and M.M. Drafting the article: E.T., A.A., A.A.-C., C.S., L.L., and M.M. Critical revision of the article of important intellectual content: E.T., A.A., C.S., L.L., and M.M.
Disclosure Statement
E.T.: Consultant for Medtronic. A.A., A.A.C., and C.S.: No conflicts of interest relevant to this article were reported. L.L.: Consultant for Boehringer Ingelheim Pharmaceutical, Eli Lilly and Company, Insulet Corporation, Janssen Pharmaceuticals, Medtronic, Dompe, Provention, Roche. M.M.: Consultant for Sanofi.
Funding Information
This study was supported by the Beatson Foundation (Grant number: #2021-017). Role of the funder/sponsor: The funding source had no role in the design or conduct of the study; collection, management, analyses, interpretation of the data; or preparation and decision to submit article for publication.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.