
Abstract
Introduction:
This study set out to examine the use of telehealth resources to tackle the coronavirus disease 2019 (COVID-19) pandemic in Latin America within the scope of national telehealth projects (NTPs).
Methods:
A qualitative study developed using ethnomethodology for appropriate understanding of how telehealth actions were carried out in practice during the COVID-19 pandemic within the scope of NTPs, in the following countries: Argentina, Colombia, Costa Rica, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Peru, and Uruguay. The study was carried out from October to 2020 to March 2021. The number of participations in the discussion groups, formed by coordinating teams of NTPs, totaled 90. Results were described in the worksheet completed according to the script. Each country reviewed its respective data, three times on average, in an effort to clarify actions developed.
Results
: Three groups of countries were identified: (1) Countries with a telehealth background that used these resources to tackle COVID-19 and thereby refined telehealth activities. Countries with greater experience in NTP design, such as Mexico, Colombia, Peru, and Argentina, were able to use a wide range of telehealth activities to tackle the pandemic, with offers of teleconsultation, teleguidance, telemonitoring to patients, and training of health professionals; (2) Countries with some telehealth activities to address COVID-19. Uruguay, Ecuador, El Salvador, and Costa Rica; and (3) Countries with no evidence of telehealth resource use during the pandemic. Honduras and Guatemala.
Discussion:
Most NTPs in Latin America have improved their telehealth activities, contributing to address the COVID-19 pandemic in Latin America.
Introduction
An Increased use of telehealth and telemedicine resources during the coronavirus disease 2019 (COVID-19) pandemic has highlighted its potential benefits and limitations. In some countries, planned telehealth development processes enabled wider use of these resources to tackle the pandemic.
Telemedicine has offset the decline in outpatient service volume. 1 Analysis of data from a national sample of 16.7 million individuals living in the United States in 2020, revealed that telemedicine use growth has offset about two-thirds of the decline in in-person visit volume during the COVID-19 pandemic. According to a study with 2,900 physicians carried out in Pennsylvania, 2 the use of telehealth resources to tackle COVID-19 increased by 1,000%.
Another study 3 that examined Primary Health Care (PHC) structuring processes and the use of telemedicine in Europe revealed that telehealth is an alternative. Overall, extensive adoption of telehealth in PHC appears to be a matter of work organization and health financing rather than technology and ethics. An Australian 4 study investigating telehealth and PHC has also reported that COVID-19 has transformed Australian primary care.
However, despite the rapid expansion of telehealth resources, the continuity of telehealth care and the different aspects that interfere with telehealth expansion are being further investigated. According to a study 5 carried out in the United States in 2021, the COVID-19 pandemic had immediate and far-reaching implications for the health care system. Recent reports revealed a significant and ongoing decline in telehealth use (down to 21% of medical appointments).
A systematic review addressing telehealth and COVID-196 identified a sizable body of literature on telehealth use during the first 6 months of the COVID-19 pandemic, particularly in high-income countries. The feasibility and utility of telehealth in resource-limited settings and low- to middle-income countries must be determined. In another systematic review on telehealth and COVID-19, 7 articles were focused on obstacles to maximizing telehealth use and how to tackle them.
In Latin America, telehealth resource incorporation and National Telehealth Project (NTP) structuring varies widely. Large gaps between Latin American countries and countries with higher socioeconomic status have been reported in studies 8,9 published by the WHO and PAHO. Before the pandemic, some studies 10,11 had already shown that Mexico, Colombia, and Brazil were the Latin American countries with better-structured NTPs, whereas most other countries were still developing their respective NTPs. This study set out to examine the use of telehealth resources to tackle the COVID-19 pandemic in Latin America within the scope of NTPs.
Methods
This is a qualitative study developed using ethnomethodology (i.e., the study of practices, procedures, methods, and common-sense knowledge used by social actors to understand and produce the social environments in which they participate). 12 Ethnomethodology was selected for appropriate understanding of how telehealth actions were carried out in practice during the COVID-19 pandemic in different Latin American countries. This methodological approach is applicable due to the wide range of terminologies and actions in selected countries, which require different consensus-building processes for reliable comparisons of data.
This study examined the performance of national telehealth programs during the COVID-19 pandemic in the following countries: Mexico, Colombia, Peru, Costa Rica, Argentina, Guatemala, Honduras, El Salvador, Uruguay, and Ecuador. The study was carried out in these 10 countries from October to 2020 to March 2021.
Aforementioned countries were selected due to their relations with the organization of a group of Latin American telehealth coordinators and former coordinators who meet periodically to reflect and formulate proposals and investigate the development of telehealth in Latin America. These meetings have been held since 2012. Despite the participation of Brazilian institutions within the group, the Brazilian Ministry of Health has not participated in the group since 2017.
Ethnomethodology seeks to understand organizational phenomena from the practical social context of a group and its everyday activities. 13
This study was based on the following question: Which of the telehealth activities were incorporated into the NTP to combat the COVID-19 pandemic? Two strategies were used to appreciate these dimensions in the context of telehealth and the COVID-19 pandemic. First, discussion groups were structured with the coordinating teams of the NTP through Web-based conferences. In group meetings, different telehealth initiatives carried out in COVID-19 settings in each country were presented and discussed according to a pre-established script.
Telehealth coordinators from the different countries delivered presentations addressing the following guiding question: Walk us through how telehealth actions are organized and developed in COVID-19 settings in your country, in the light of the NTP. An instrument to be used as a script for the discussion was then prepared, including the following aspects: Current contextualization of telehealth in the national health care system––telehealth status before the pandemic, new telehealth actions developed during the pandemic, results of telehealth actions developed in COVID-19 settings, maintenance and replicability perspectives in other scenarios, and (whenever possible) impacts on assistance.
Discussions were recorded and transcribed. Researchers then produced a script based on aspects described in Table 1, including two key items: (1) Overview of telehealth and COVID-19 actions in Latin America and (2) Telehealth activities carried out during the COVID-19 pandemic in Latin America.
Telehealth Actions to Tackle Coronavirus Disease 2019
COVID-19, coronavirus disease 2019.
At a later stage, data extracted from presentations and discussions were compiled by researchers and sent back to telehealth coordinators from selected countries for validation and/or rectification. A worksheet prepared by research group experts was used as a reference.
Five discussion groups were held with the coordinating teams of the NTP from participating countries. Presentations to be given by each country were scheduled in advance. In this manner, the material could be prepared according to the script. The number of participations in the discussion groups totaled 90, with an average duration of 2.5 h.
Results were described in the worksheet filled out according to the script shown in Table 1. For validation purposes, each country reviewed its respective data, three times on average, in an effort to clarify actions developed.
Data analysis was based on the ethnomethodological approach. This study set out to examine the implementation of telehealth actions developed in selected countries to tackle the COVID-19 pandemic. Hence, efforts were made to organize the analysis of data collected according to important ethnomethodology concepts: social actor, social order, and social action. Efforts were also made to identify which resources are being routinely used to promote COVID-19-tackling actions to understand the structuring phases of national telehealth programs and determine how telehealth activities are organized in daily health care routine. Are new standards emerging? How are norms expressed in daily activities? 14,15 Figure 1 presents a flow chart illustrating the executed activities.
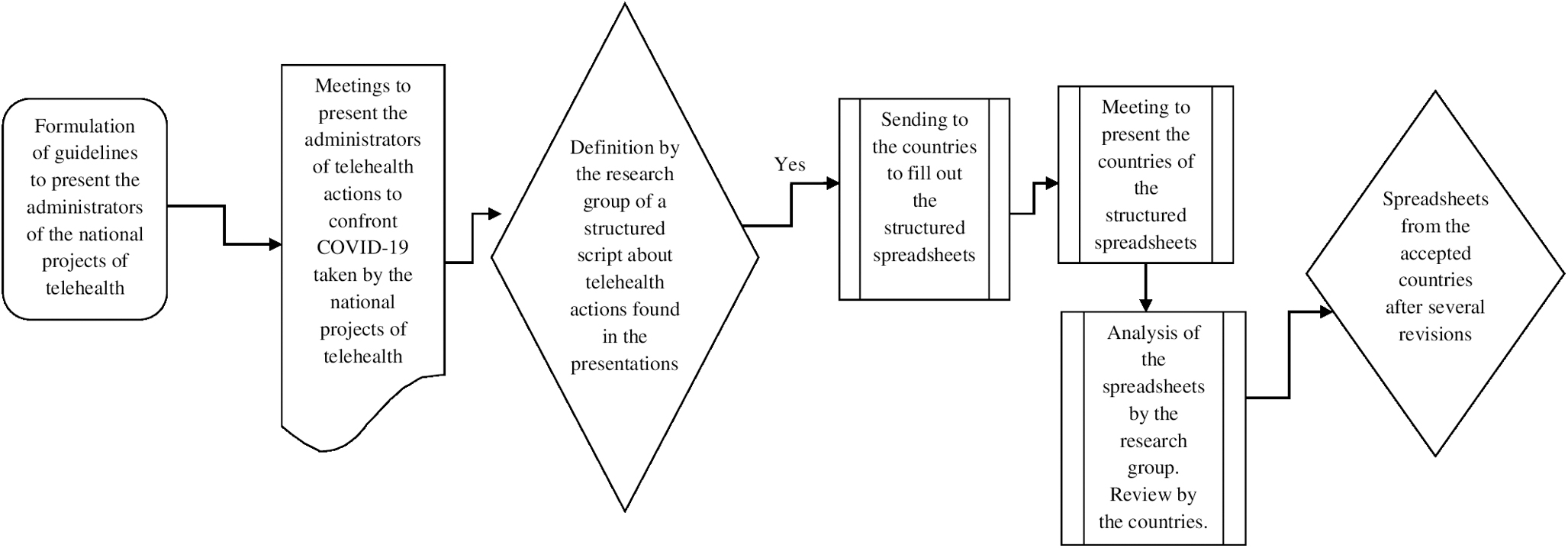
Organizational chart of activities performed by the research group.
Data collected were analyzed according to this design. This study was approved by the Research Ethics Committee of Universidade Federal de Minas Gerais (UFMG), CAAE opinion No. 12735019.1.0000.5149. Participants signed an Informed Consent Form (ICF).
Results
Systematic analysis carried out to obtain an overview of telehealth actions aimed at tackling COVID-19 in selected Latin American countries revealed significant advancements in NTPs in most cases. These advancements contributed to the fight against COVID-19 in Mexico, Colombia, Peru, Ecuador, Argentina, El Salvador, Costa Rica, and Uruguay, in particular initiatives carried out in Mexico, Colombia, and Peru.
Guatemala and Honduras have not made progress regarding the use of telehealth resources to tackle COVID-19. However, Guatemala is taking the first steps toward implementation of an NTP: “After the COVID-19 pandemic, the Ministry of Health of Guatemala acknowledged the importance of developing a NTP and created a group for this purpose. Currently, only 23% of the population has access to telehealth coverage, through NGO projects such as Tula Salud, Unicar, private universities and other private institutions.” (DG,02).
Detailed description of telehealth activities used by each country provides an overview of the use of telehealth resources during the pandemic. Seven out of 10 countries analyzed report improvements in telehealth service structure in 2020 and 2021 (Table 2).
Overview of Telehealth and Coronavirus Disease 2019 Actions in Latin America—March 2021
Mexico: Telehealth actions 2019 = 246,720; 2020 = 5,741,033.
Colombia: Increases since January 2020—117% head offices (from 1,067 in 2019 to 2,450 in 2020); services (from 3,047 in 2019 to 9,582 in 2020; 192% increase in services). From March 2020 to August 2021, 113,379,109 calls were made (teleguidance and teleconsultations).
Peru: Before the pandemic—250 people per day; then—30,000 people per day; more than 31 million telemedicine appointments at MINSA public health facilities and regional administrations.
Ecuador: The use of technology platforms and line 171 (option 5 in call center services for people with symptoms).
With regard to regulations related to structuring of telehealth and COVID-19 services, a specific law was approved by the National Congress in Argentina and Peru. Interim laws for implementation of telehealth services were also approved in Mexico, Uruguay, Colombia, and Costa Rica, opening up new possibilities for telehealth resource use. Peru and Colombia also published additional rules and resolutions in an effort to guide and detail the scope and operating process of telehealth services aimed at tackling COVID-19, as did other countries.
In Mexico, Dirección General de Información en Salud, incorporated new remote care variables, especially those describing actions aimed at care for symptomatic patients and suspicious cases of COVID-19. Diversification of telehealth resource use was also observed in most countries (Table 2). The use of direct text messaging systems linked to telehealth services and implementation of video calls between patients and telehealth services were reported by six countries (Mexico, Colombia, Peru, Ecuador, El Salvador, and Costa Rica). In these countries, patients were also able to make direct calls to telehealth services to obtain information about COVID-19. Integration of telehealth systems to new innovative techniques (artificial intelligence and machine learning) was implemented in Colombia, Mexico, Peru, and Ecuador, although in an incipient manner: “Telehealth transforms traditional methods of relation between patients and health care professionals; actions aimed at integration with other tools must be incorporated into health care services. Colombia has launched an ethical framework for artificial intelligence in the country…” (DG,01)
As to telehealth activities developed by selected countries, different modalities were used (Table 3). Activities aimed at providing direct access to telehealth services were particularly emphasized. Mexico, Colombia, Peru, El Salvador, and Costa Rica implemented direct access systems for telehealth services for teleconsultations.
Telehealth Activities Developed in Countries Studied During the Coronavirus Disease 2019 Pandemic
A significant increase in the number of teleconsultations has been observed, particularly in Colombia and Peru. Costa Rica has experienced an increase in direct health care provision, allowing for follow-up of COVID-19 patients as well as continuity of care for patients with chronic diseases. In Uruguay, face-to-face consultations were restricted to the maximum. Consultations and follow-up were carried out virtually or by telephone call through different platforms.
Telemonitoring activities were offered in the following countries: Mexico, Colombia, Peru, El Salvador, and Ecuador. Digitized prescriptions were implemented and supported by telehealth programs. Most countries managed to incorporate teleguidance activities into the telehealth system. In Peru, a dedicated robust teleguidance system was developed and reached more than 2 million people.
With regard to contact between professionals, the use of telehealth resources for teleconsulting during the COVID-19 pandemic was reported by seven countries: Mexico, Colombia, Peru, Ecuador, Costa Rica, El Salvador, and Honduras.
Guatemala and Honduras did not report teletraining activities through telehealth systems. Tele-management activities were carried out in Mexico, Peru, Ecuador, Argentina, El Salvador, Costa Rica, and Uruguay.
According to the data collection analysis of this study, three large blocks of countries emerged regarding the use of telehealth resources to tackle COVID-19 (Table 4).
Distribution of Countries Regarding Telehealth Activities in the Face of Coronavirus Disease 2019 According to Groups
COUNTRIES WITH A TELEHEALTH BACKGROUND THAT USED THESE RESOURCES TO TACKLE COVID-19 AND THEREBY REFINED TELEHEALTH ACTIVITIES
This block includes countries that have had structured PNTs for several years, in particular Colombia and Mexico. In these countries, with many years of continuous NTP operation, available telehealth resources were used to their full potential to tackle COVID-19. Legislation was improved, services and activities were expanded, and other innovative dimensions, such as the use of artificial intelligence and machine learning, began to be incorporated into existing telehealth projects. Exposures shifted from telehealth accumulation in respective projects to quickly taking a stance to tackle COVID-19 in the country.
In Peru, as of March 2020, the Ministry of Health started to act toward innovation, implementation, and modification of telehealth legal regulations in force so far, as well as adaptation of assistance processes for patient care in public health care establishments at the national level, boosted by new telemedicine services in times of COVID-19.
“In Peru, telehealth is a National Policy. Telehealth implementation is of national interest and connects the 25 regions. Text messaging services, video calls and use of fixed or mobile telephone services are allowed and were implemented for access to telemedicine services. One implementation was carried for scheduling of and assignment of patients to health care personnel for telemedicine care. A large teleguidance service for patients (the so called HAKU), was implemented at the national level.” (DG,4).
Of these selected countries, Argentina is the one with the most recent PNT, implemented in 2018. However, in the context of the pandemic, telemedicine was quickly adopted in many aspects, in public and private settings. Argentina experienced high levels of adherence to telemedicine during the COVID-19 pandemic. Actions aimed at tackling the pandemic were particularly related to screening, postpandemic monitoring, and moderate patient management.
COUNTRIES WITH SOME TELEHEALTH ACTIVITIES TO TACKLE COVID-19
The following countries fell into this group: Uruguay, Ecuador, El Salvador, and Costa Rica. El Salvador has taken a big step forward regarding the telehealth project. In that country, actions were structured to tackle the pandemic in several areas, including teleassistance, telemonitoring, teletraining, teleguidance, teleconsulting, and telescheduling across different levels of care.
During the pandemic, Uruguay, which started its NTP based on images, implemented the use of digitized prescriptions, enacted the Telemedicine and the Telework laws, and developed specific apps for health care during the pandemic. However, a definitive national plan for use of telehealth resources is lacking.
Costa Rica started to develop an NTP based on the COVID-19 experience. Significant structuring of telehealth actions involving teleconsultations and teleguidance has already taken place. Ecuador, which also has a very inconsistent NTP, managed to implement its telehealth project only in regions where there is a collaboration with Peru to tackle COVID-19.
“A telehealth project is being developed in Ecuador. However, the country faces severe limitations regarding connectivity and access to the rural population is very complicated…the national project is still being structured….” (DG,4).
COUNTRIES WITH NO EVIDENCE OF TELEHEALTH RESOURCE USE DURING THE PANDEMIC
This group includes Honduras and Guatemala. In spite of not having used telehealth resources to tackle the pandemic, Guatemala has taken important steps toward structuring its PNT. Honduras does not have a PNT, which makes the local intervention process difficult.
“We are still trying to generate and guarantee the academic and technological knowledge required for Telehealth implementation in the National Health System of Honduras in a standardized and systematic way.” (DG,4).
Discussion
The use of telehealth resources in NTPs to tackle the COVID-19 pandemic in Latin America varies widely. Still, the use of telehealth resources increased in most countries in this sample. Similar findings have been reported in studies carried out in different countries. 1,16,17 Greater difficulty to incorporate telehealth resources in middle- to low-income countries has been described is some studies. 18,19 This digital divide has been driven by social determinants of health, including lack of internet access or internet-enabled devices, digital literacy, medical or technological distrust, and issues related to access to and reimbursement of health care. Another study 20 revealed that telehealth played a prominent role in primary care delivery in New York City. However, the transition to telehealth did not take place in the same manner in different communities.
Difficulties associated with the use of different ICTs have been addressed in a CEPAL study. 21 Socioeconomic factors pertaining to Latin America, particularly urban–rural mismatches, have been emphasized in that study.
Countries with greater experience in NTP design, such as Mexico, Colombia, Peru, and Argentina, were able to use a wide range of telehealth activities to tackle the pandemic. These countries already had a background in the use of telehealth resources. 22 Analysis of telehealth activities carried out to tackle the COVID-19 pandemic revealed significant advancements in the articulation of telehealth services and direct relationships with the population in these countries, with offers of teleconsultation, teleguidance, telemonitoring to patients, and training of health professionals. The use of telehealth resources also led to improvement of technological processes and incipient incorporation of artificial intelligence and machine learning, as reported in another study. 23 According to that study, a greater use of telehealth resources encourages to gradual reinvention of health services.
One study conducted in North Carolina 24 reported that health systems should take advantage of lessons learned during the COVID-19 pandemic to inform the sustainable adoption of telemedicine.
These aforementioned countries also interacted with regulatory bodies to improve regulatory activities related to telehealth actions. Greater institutionalization of ST actions within the scope of national projects has been described. Countries, such as France and the United States 2,17,25 have refined the regulation of telehealth resource use by incorporating telehealth activity reimbursement dimensions. According to Indian National Telemedicine data, an extensive use of telehealth resources generated more than 10 million consultations in India up to December 2020. 17
Latin American countries, which could not implement such a wide array of telehealth resources to tackle the COVID-19 pandemic have also moved forward and used telehealth for teleguidance and telemonitoring activities. Most Latin American countries in this sample went through a similar process. A direct use of teleconsultations followed the global development trend. 26,27 In Ecuador, the NTP did not advance during the pandemic. In Uruguay, the telehealth law was enacted and drafting of a regulatory decree is in progress. Guatemala launched its national project. Honduras was the only country which failed to developed an NTP. These findings reveal inequalities in the incorporation of telehealth resources in Latin America. 28
In this study, data were collected from presentations delivered by the Ministries of Health and may contain overestimations. Terminology standardization processes are subject to different interpretations and comparisons with prepandemic periods. In spite of these limitations, this study provided an overview of telehealth resource incorporation processes during the COVID-19 pandemic in Latin American countries.
Conclusions
Incorporation of telehealth resources supported the confrontation of the COVID-19 pandemic in several countries in this sample. National projects were improved in some countries. In other countries, new activities were incorporated into existing NTPs. A minority of countries did not make progress regarding the use of telehealth resources within the scope of national projects to tackle the COVID-19 pandemic. There is still a lot to be done regarding the development of telehealth actions in Latin America.
Footnotes
Authors' Contributions
Each author played a role in the development of this article. They are as follows: (1) A.d.F.d.S.—Redaction and revision; (2) A.P.-L.—Data collection; (3) A.C.C.H.—Data collection; (4) B.I.C.U.—Data collection; (5) D.C.A.M.—Data collection; (6) E.L.—Data collection; (7) M.P.d.A.—Revision, formatting and submission; (8) O.I.R.—Data collection; (9) R.H.R.A.—Data collection; (10) S.E.D.C.—Data collection; (11) S.E.G.M.—Data collection; (12) S.B.R.C.R.—Data collection and translation; (13) Y.A.H.M.—Data collection; and (14) R.G.C.R.—Data collection.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.