
Abstract
Background:
Atypical pigmented facial lesions (aPFLs) often display clinical and dermoscopic equivocal and/or overlapping features, thus causing a challenging and delayed diagnosis and/or inappropriate excisions. No specific registry dedicated to aPFL paired with clinical data is available to date.
Methods
: The dataset is hosted on a specifically designed web platform. Each complete case was composed of the following data: (1) one dermoscopic picture; (2) one clinical picture; (3) two lesion data, that is, maximum diameter and facial location (e.g., orbital area/forehead/nose/cheek/chin/mouth); (4) patient's demographics: family history of melanoma, history of sunburns in childhood, phototype, pheomelanine, eyes/hair color, multiple nevi/dysplastic nevi on the body; and (5) acquisition device (videodermatoscope/camera-based/smartphone-based system).
Results:
A total of 11 dermatologic centers contributed to a final teledermoscopy database of 1,197 aPFL with a distribution of 353 lentigo maligna (LM), 146 lentigo maligna melanoma (LMM), 231 pigmented actinic keratoses, 266 solar lentigo, 125 atypical nevi, 48 seborrheic keratosis, and 28 seborrheic-lichenoid keratoses. The cheek site was involved in half of aPFL cases (50%). Compared with those with the other aPFL cases, patients with LM/LMM were predominantly men, older (69.32 ± 12.9 years on average vs. 62.69 ± 14.51), exhibited larger lesions (11.88 ± 7.74 mm average maximum diameter vs. 9.33 ± 6.46 mm), and reported a positive history of sunburn in childhood.
Conclusions:
The iDScore facial dataset currently represents a precious source of data suitable for the design of diagnostic support tools based on risk scoring classifiers to help dermatologists in recognizing LM/LMM among challenging aPFL in clinical practice.
Introduction
Cutaneous malignant melanoma (MM) is a public health problem: over the past 10 years, an increase in incidence rates was reported worldwide (e.g., from ∼25–30 new cases/100,000 population/year in Europe and United States, to ∼60 new cases/100,000 population/year in Australia). 1 –3 Lentigo maligna (LM) is an in situ cutaneous melanoma occurring in photodamaged skin, with a peak incidence in the seventh to eighth decades of life, characterized by the proliferation of atypical melanocytes along the basal epidermal layer. If untreated, LM progresses to its invasive form, lentigo maligna melanoma (LMM), in ∼2–3.5% cases per year. 4 The majority of LM/LMM cases localized on the face, scalp, and neck, with rare presentations on the trunk and extremities on rare occasions. 3 –5 The importance of the body location—and, consequently, the modality of sun exposure (chronic vs. intermittent)—for the development and prognosis of MM has been pointed out in several studies. 5 –8 In particular, LM/LMM of the face, scalp, and neck seems to have poorer survival rates compared with MM of the body. 5,6,9
However, few investigations to date have been carried out to define a comprehensive set of independent risk factors (e.g., age, sex, histology, and thickness) and/or develop an integrated tool to comprehensively predict the prognoses of LM/LMM of the face, scalp, and neck. 9,10 Moreover, some LM subtypes are often excluded from studies on in situ MM; in other cases, the reported MM incidence rates do not take into account histological specific subtypes. 1 –4,9 –11 Besides the fact that majority of LM/LMM cases develop in elderly people, which can explain a late referring to a specialists, a tardive diagnosis can be determined by a certain quote of wrong diagnoses and/or treatments. 12,13 This is because of the fact that photo-aged skin also exhibits a series of atypical pigmented facial lesions (aPFLs), which can possibly simulate LM/LMM not only clinically but also dermoscopically. These challenging entities, which can be either benign (i.e., solar lentigo —SL, seborrheic keratosis—SK, or seborrheic-lichenoid keratosis—SLK) or potentially evolve into malignancy (i.e., pigmented actinic keratosis—PAK, atypical nevus—AN) are far more common than LM/LMM and, thus, frequently excised. On the contrary, the currently available dermoscopic web registries are dedicated to the clearcut cases of the overmentioned simulators and are not paired with a detailed list of risk factors, patient characteristics, and clinical pictures. 14 –16 In addition, exhaustive international datasets for facial LM/LMM describing lesions and patients' characteristics are still lacking. 5
Based on this, there was the need of creating an international web registry devoted to a better understanding of the epidemiology, risk factors, and commonly shared features of benign and malignant aPFL, suited for the extensive data collection capable of overcoming the research issues related to the peculiar number of patients referring to each single dermatologic center.
We thus aimed to: (1) obtain an epidemiological and morphological characterization of a large series of aPFL cases; (2) investigate multiple demographic data and risk factors of patients together with the clinical and dermoscopic features of the lesions; and (3) define a subset of data that differentiate LM/LMM from their simulator aPFLs.
Methods
STUDY DESIGN
The registry was set up as part of the iDScore-facial lesions project and is currently hosted on
The data were collected both retrospectively, in reference to the data available at the time of the enrolment of each participating center into project, and prospectively with respect to information collected starting from the time of enrolment. This retrospective study was approved by Local Ethics Committee and was carried out in accordance with Helsinki declaration.
CENTER PARTICIPATION
Participation was open to any European dermatologic center that was routinely active in the skin cancer screening and management as well as in the diagnostics of pigmented skin lesions based on dermoscopic examination, picture collection, and analysis. There were neither costs nor financial compensation to participate, as data collected refer only to information routinely gathered in clinical practice. A center was enrolled if it was able to provide at least 80 cases (up to a maximum of 130 cases) of clinically and dermoscopically challenging aPFL excised suspecting malignancy, evaluated during routine skin tumor screening activity. In each contribution, a minimum of 30 malignant cases and 50 benign cases should be provided. Each center was recommended to follow specific ranges for case distribution: 30–50 LM/LMM, 20–40 SL, 20–40 PAK, 10–30 AN, 10–30 SK, and 10–30 SLK.
INCLUSION CRITERIA
Each aPFL case should be composed of one dermoscopic image and a series of five mandatory data referring to the lesion (three) and to the patients (two). Lesion mandatory data included: definitive histopathological diagnosis, maximum diameter (mm), and precise body location according to six different subareas—nose, orbital area, chin, cheek, forehead, and mouth. Patients' mandatory data included sex (F/M) and age (years). The association with one clinical picture was strongly recommended. A series of eight optional parameters were required, including: histologic data for LMM (thickness, mythoses number, regression %, and presence of lymphocytic infiltrate), personal or family history of melanoma (i.e., in a first degree relative) (positive/negative), history of sunburns (>3) in childhood below the age of 14 years (positive/negative), presence of multiple common nevi (>100) or dysplastic nevi (>10) on the body (positive/negative), phototype (I–IV), presence of pheomelanine (yes/no), presence of green/light-blue/blue eyes or blond hair. Of note, only one lesion per patient could be provided, to avoid repetition of clinical/anamnestic data and further bias affecting data analysis.
IMAGE REQUIREMENTS
Dermoscopic images should conform to minimal quality requirements, including: in focus lesion, ≥1.5 Mpx, 15–20 × enlargement, and JPEG format. To reduce the differences in photographic characteristics, a series of specific device for dermoscopic images acquisition was also indicated: videodermatoscope—Fotofinder system Medcam1000; camera-based systems—Dermlite Photo System Pro/Dermlite Foto II Pro WITH Nikon D500, 3GEN Dermlite Foto Dermoscopy System, Heine DL 20 Canon/Nikon; smartphone-based system—Foto X Dermlite.
PLATFORM LAYOUT
The web-based platform was designed in 2018 by informatic engineers in collaboration with dermatologists (L.T., P.R.) and a biomedical engineer (G.C.), and progressively updated by a biostatistician (A.C.) and a data manager. It currently hosts two other iDScore projects dedicated to the melanoma of the body and of palmoplantar areas. The iDScore facial dataset is accessible from the dedicated link on the platform connected and stored in a secured server of Siena University (
CONTRIBUTION TIMING AND MODALITY
Cases were collected in the online database between July 2021 and April 2022 through a predefined online form, the “Contribution form,” which was designed to record a total of 13 parameters (5 mandatory and 8 optional) along with 2 standardized image files. The modality of image acquisition was also required, among videodermatoscopes, camera-based systems, or smartphone-based systems.
EXCLUSION CRITERIA
All blurred dermoscopic and/or clinical images were rejected. Moreover, we excluded clinical pictures from which the patient's personal characteristics were recognizable (tattoos, piercings, etc.). Finally, contribution forms that were deficient of mandatory data or those concerning the device used for image acquisition were not accepted.
CASE QUALITY CHECK
Review of all the cases received in the registry was performed by the Principal Investigator (L.T.) and data managers (A.C. and A.T.) from September 2021 to July 2022, in parallel with the case uploaded: this allowed the PI to update each Site Investigator about the current rate of case acceptance and make them go ahead with the contribution until reaching the minimum criteria. A case was finally accepted if judged “challenging” according to two three skilled dermoscopists (L.T., M.B., E.C.). Duplicate cases (e.g., multiple dermoscopic images of the same patient uploaded as separate cases, the same case entered two or three times) were rejected.
ETHICS
This study was approved by Siena local ethical committee in April 2018 (Azienda Ospedaliero-Universitaria Senese, Siena, Italy, Study Protocol No. 16801) and then shared with the participating centers, following the recommendations from the Declaration of Helsinki. Patient consent for data collection was waived due to the observational study type; it was obtained for image publication. All data were deidentified before use and are kept in accordance with the EU General Data Protection Regulations (GDPR) on the processing of personal data and the protection of privacy in the electronic communication (2016/679/EU). 21
STATISTICAL ANALYSIS
Descriptive statistics was applied to the whole database. The binomial or categorical data were variously expressed as number of observations (n), percentage (%), mean, standard deviation, and range. Analysis of variance test and chi-squared test were used to evaluate the mean of age and diameter between the histological diagnosis and the association between categorical variables and histological diagnosis, respectively. If the tests were significant, multiple t-tests and multiple Fisher's exact tests with false discovery rate (FDR) correction were performed to evaluate the difference among the diagnoses taken in pairs. The t-test and chi-squared test were used to compare benign with malignant lesions. A significance of p < 0.05 was assumed.
Results
PARTICIPANTS AND DATABASE COMPOSITION
Among 21 invited centers, 11 were able to meet the minimum contribution criteria, that is: Thessaloniki, Gothenburg, Modena, Reggio Emilia, Napoli, Nis, Meldola, Bologna, Brussels, St. Etienne, and Siena. After quality check, a total of 1,197 of 1,253 aPFL cases were accepted: of them, 272 (23%) had the optional risk factor data assessed, whereas 700 (58.5%) had the optional clinical picture (Figs. 1 –3 ).
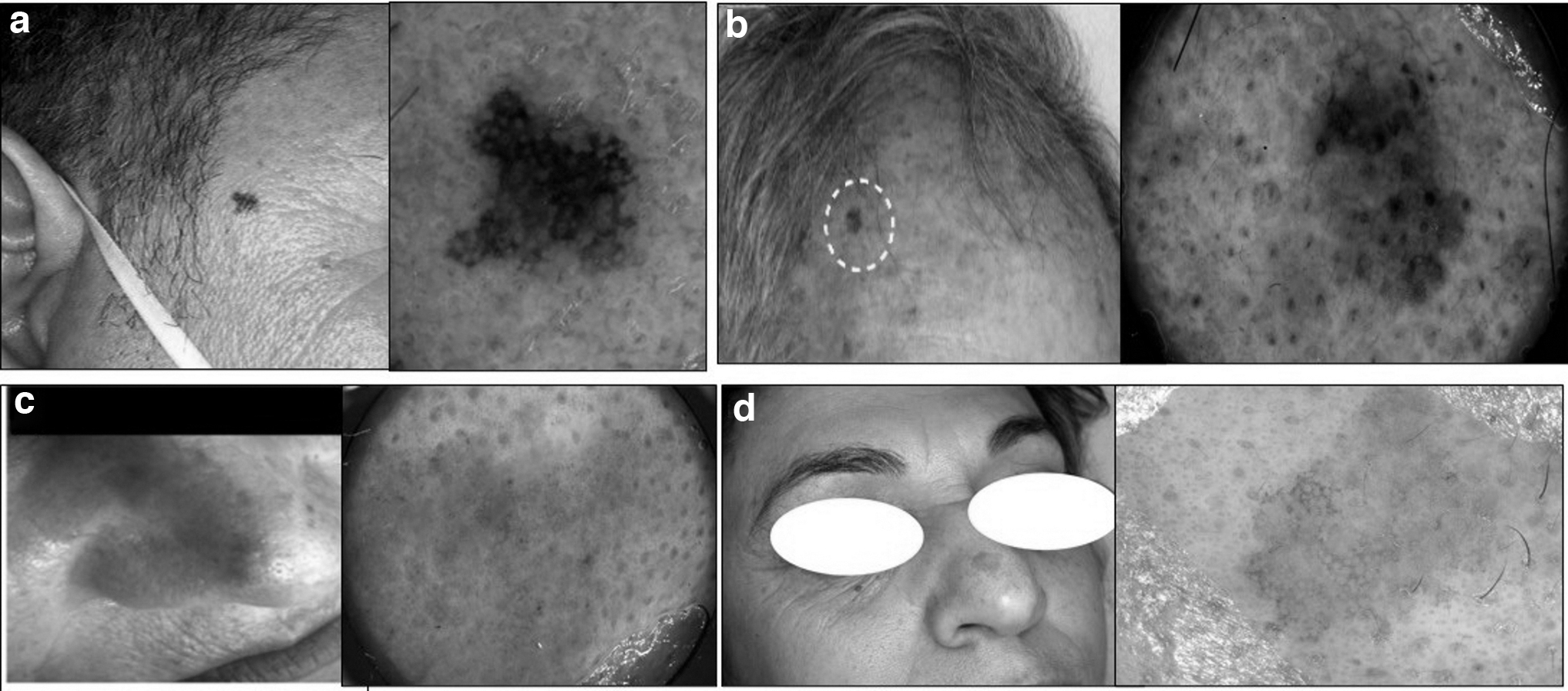
Example of benign cases of atypical pigmented facial lesions excised because of a challenging clinical and/or dermoscopic appearance and histopathological examination to rule out LM suspect: an AN of 6 mm in diameter in the temple of a 52-year-old man
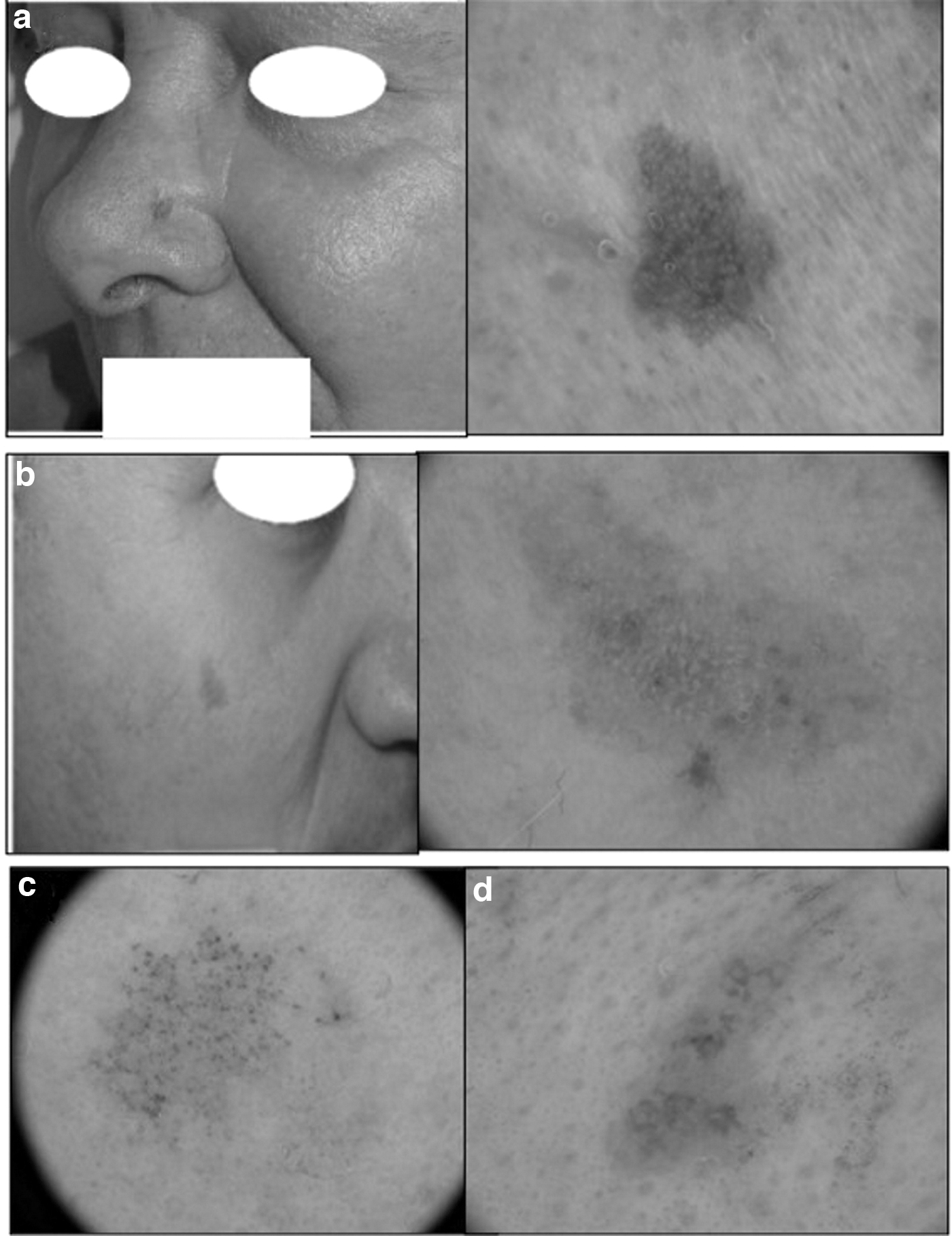
Example of LM cases showing equivocal dermoscopic appearance and misinterpreted as benign pigmented facial lesions: a 4 mm LM on the nose of a 69-year-old woman, simulating SL
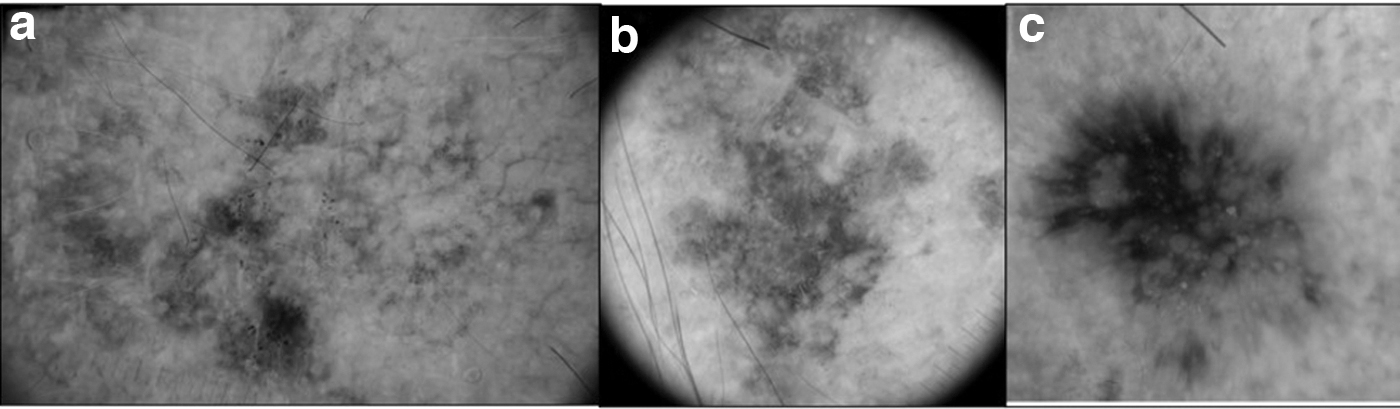
Example of PAK acquired with different imaging devices, showing dermoscopic atypical features and excised suspecting malignancy: a 18 mm PAK on the forehead of a 76-year-old man, acquired with a videodermatoscope system
PATIENTs' DATA
Descriptive analysis on patient characteristics showed a mean age of 65.4 years (range, 18–97), an equal distribution among women and men, and history of sunburn in childhood as the most frequently reported risk factor (Table 1). The significance of the distribution and association analysis between the two patient demographics and eight melanoma risk factors, investigated among the seven different aPFL histotypes is given in Table 2: age ranged from 68–69 years of LM, LMM, and PAK cases to 47.86 ± 13.8 of AN cases; the presence of multiple common nevi (>100) or dysplastic nevi (>10) on the body was predominantly observed in LM and LMM cases (28% and 22%, respectively), whereas that of pheomelanine in AN, PAK, and SL cases (10–11%); the history of sunburns in childhood was positive in PAK (83%) and AN (78%) cases; phototype II was prevalent in LM (21%) and SL (18%) cases, whereas phototype III in SK cases (48%); no statistically significant differences were observed in the distribution sex, pale eye color, and blond hair.
Characteristics of the Patients Included into the iDScore facial Dataset
SD, standard deviation.
Significance of the Distribution and Association Analysis (p) Between Two Patients Demographics and Eight Melanoma Risk Factors, Investigated Among the Seven Different Atypical Pigmented Facial Lesions Histotypes
The difference between the following pairs is statistically significant:
Subset of 1,111 aPF cases;°numerosity is expressed as ratio between the number of positive cases for that risk factor/the number of “assessed” cases for that aPFL type.
AN, atypical nevus; aPFL, atypical pigmented facial lesions; LM, lentigo maligna; LMM, lentigo maligna melanoma; PAK, pigmented actinic keratosis; SK, seborrheic keratosis; SL, solar lentigo; SLK, seborrheic-lichenoid keratosis.
LESIONs' DATA
LM represented the most numerous group (29.5% of cases) followed by SL (22.2%), PAK (19.3%), LMM (12.2%), AN (10.4%), SK (4%), and SLK (2.3%). Maximum diameter ranged from 1 to 53 mm, with an average value of 10.4 mm. About half of aPFL cases were located on the cheek, then on the forehead (18%), nose (16.7%), orbital area (10.8%), chin (3.3%), and mouth (1.5%). Significant associations were as follows: SK on the forehead, PAK on the nose, LMM on the chin; distribution analysis is further detailed in Table 3.
Characteristics of the Atypical Pigmented Facial Lesions Included in the iDScore facial Dataset: Significance of the Distribution and Association Between Histologic Classification and the Investigated Variables Is Also Reported (p)
Values are given as n (%)/mean ± SD.
The difference between the following pairs is statistically significant:
BENIGN/MALIGNANT a PFL COMPARATIVE ANALYSIS
According to the histopathological malignancy criteria, 41.7% cases were malignant and 58.3% were benign aPFL. Multivariate analysis showed significant differences in age and diameter (Table 4): patients with malignant cases were older (69.32 years on average vs. 62.69) and exhibited larger lesions (11.88 average diameter vs. 9.33) than the others, with a slight male prevalence.
Comparative Analysis of the Distribution and Association (p) of 4 Objective Parameters Among Lentigo Maligna/Lentigo Maligna Melanoma Group and Other Atypical Pigmented Facial Lesions Cases of the iDScore facial Dataset
Values are given as n (%)/mean ± SD.
aPFL: PAK, AN, SLK, SK, SL.
IMAGE ACQUISITION DATA
Table 5 provides the frequency of use of different dermoscopic devices on 1,111 aPFL and among the 7 different histotypes, along with association analysis. Camera-based system was used in 46% of aPFL cases, videodermatoscope in 43%, and smartphone in 10%. Concerning aPFL groups, smartphone-based systems were used in 9.9% cases, especially for LM (45) and PAK (30). Camera-based system acquisitions (46.3%) were mostly used for LM cases (147), followed by SL (130) and PAK (106). Videodermatoscope acquisitions (43.5%) were performed in 137 LM cases, and then in SL (104). Of note, half of PAK and SL cases were imaged with a camera-based system, whereas the majority of SK (76%) and SLK (71%) were imaged with a videodermatoscope. No significant differences were observed when considering malignant versus benign aPFL cases.
Frequency of Use of Different Dermoscopic Devices for Imaging of Atypical Pigmented Facial Lesions: Significance of the Distribution and Association Among Seven Different Histotypes Classification Is Also Reported (p)
Values are given as n (%).
Discussion
Web registries are developed with the aim of facilitating the spreading of knowledge and establish research collaboration between researchers, clinicians, specialists, and residents. This is even truer in the field of rare or peculiar diseases, as the small number of cases is a barrier to translational research and makes identification of a substantial cohort very difficult. In this context, the iDScore facial project and the corresponding database dedicated to challenging aPFL and correlated clinical–anamnestic data represents a very useful tool to overcome the current fragmentation of knowledge and accessible iconographic material on these conditions. Indeed, the public datasets of dermoscopic images to data available include clearcut exemplificative cases that are retrospectively collected based on a histopathologic criterion. 22 –25 Of converse, the lesion comprising the iDScore facial dataset were collected based on clinical, practical, and physician-driven criteria to respond to the necessity of further investigating the area of difficult-to-diagnose aPFL. Moreover, the registry is characterized by a high number of complete cases collected from 11 different centers of different countries, paired with clinical–anamnestic data and risk factors of the patients. 26,27
Actually, the present registry provided new insight into the clinical characterization of aPFL and patient profiling. We observed that aPFL has a similar incidence among men and women, aged ∼65 years, but a clearcut predilection for the check site: this can be explained by both the chronic sun exposure and the dimension of this area. Considering the site distribution among the seven histotypes, there was a slight predominance of LM and PAK in the forehead, of LMM in the nose, and of LM in the mouth. Concerning maximum average diameter, the LMM and SLK were the largest (12 and 13 mm, respectively), whereas AN was the smaller (6 mm) ( Tables 1 and 3 ).
As per the anamnestic MM risk profiling, the majority of patients presenting with aPFL have a positive history of sunburns in childhood; the phototype distribution was mainly on II and III, which are the most represented in the studied populations. When stratifying patient profiling per seven histotypes, it comes out that the presence of multiple common nevi (>100) or dysplastic nevi (>10) on the body was significantly more frequent in LM cases than in the other aPFL, as well as having blond hair (Table 2). Finally, the comparative data analysis of benign and malignant aPFL groups showed significant differences (<0.001) in patient's age and lesion maximum diameter (Table 4). Based on the overmentioned findings, a man older than 69 years presenting with aPFL lesion of >12 mm on the cheek or nose has an increased risk to have LM/LMM than a benign aPFL. On the contrary, a woman aged ∼62 years presenting with aPFL <9 mm in diameter on the cheek or forehead has more probably a benign lesion.
Considering the analysis carried out over different devices for dermoscopic imaging acquisition, it turned out that both benign (47%) and malignant (42%) aPFL were indifferently imaged with fixed devices with larger screen (videodermatoscope) or mobile devices with medium to small screen (camera based/smartphone based). In particular, 45 of 112 LM cases were imaged with a smartphone connected to a dermatoscope (Table 5). This can elicit two considerations: first, all devices are currently able to reach high dermatoscopic resolution imaging 28,29 ; second, the investigators were usually unable to define the malignancy of a given aPFL a priori, thus reserving the use of a fixed dermatoscope to the imaging of LM/LMM.
The peculiar characteristics of the iDScore facial make it a unique entity in the field of dermoscopic research and open up the opportunity to realize multiple research and educational projects. Indeed, the workflow of the iDScore facial project currently includes six phases, namely: (1) database set up; (2) teledermatologic test; (3) teledermoscopic education; (4) development of a risk scoring clinico-dermoscopic checklist; (5), design of web and smartphone Apps dedicated to the iDScore facial checklist; and (6) creation of deep learning diagnostic algorithms (i.e., deep convolutional neural networks). To date, the first three phases have been completed: the iDScore facial 30 database served as testing set for >100 European clinicians, including specialists and residents in dermatology and venereology and plastic surgeons, combining teledermoscopic training with an educational purpose.
Indeed, each participant had the possibility to perform, for free, a personal test—unique in composition—on 30 aPFL complete cases extracted from the database (i.e., dermoscopic picture, clinical picture, clinical data) and were supported in the pattern analysis having the suggestion of 14 dermoscopic features (i.e., exemplificative dermoscopic images plus the currently accepted definition). This enabled the participants not only to face and evaluate, in an adequate amount of time and in a relaxed setting, a high number of difficult lesions with standardized high-quality pictures, but also to train themselves on the recognition of specific dermoscopic patterns.
The present study has some limitations: (1) lesions on the scalp, neck, and ear were excluded although chronically exposed to the sun because, being anatomically out of the face, are characterized by different dermoscopic appearance; (2) we excluded ulcerated, inflamed, and intensely traumatized aPF from the dataset, because the dermoscopic appearance in these conditions is altered; (3) we decided not to include nodular MM cases, because their differential diagnosis from LM//PAK/SLK is not challenging; and (4) the mandatory data of the availability of histopathologic report for each aPFLs case may be otherwise considered as a lesion selection bias.
In future, multiple data analyses, based not only on the biological and anamnestic data of lesions and patients but also on the collected participants' evaluations, will allow the development of different precious tools (i.e., semi-automatic scoring checklist, automatic AI software) able to support dermatologists in the diagnosis and management of challenging aPFL. 13,23
Footnotes
Acknowledgments
This study is submitted on behalf of the European Teledermatology task force—European Academy of Dermatology and Venereology.
Authors' Contributions
L.T., A.T., and A.C. contributed to the design and implementation of the research, to the analysis of the results and to the writing of the article. A.L., J.P., F.F., C.L., R.P., E.M., D.T., I.S., S.M., M.S., V.D.M., E.M., I.Z., E.Z., M.A.P., G.P., and M.B. contributed to data collection. E.C., G.C., G.A., and P.R. conceived the original and supervised the project.
Informed Consent
The patients in this article have given written informed consent to publication of their case details.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.