
Abstract
Aim:
To investigate patterns of virtual prenatal visits and examine reasons for not pursuing virtual visits for prenatal care.
Methods:
A pooled cross-sectional study used Pregnancy Risk Assessment Monitoring System from October 2020 through June 2021, a nationally representative surveillance system targeted at women who recently gave live birth. Individuals (n = 11,829) who reported their prenatal care experiences were included. A modified poison regression estimated prevalence ratios for virtual prenatal visits and reasons for not using virtual services.
Results:
One-third of participants used virtual prenatal care. Hispanics were more likely to use virtual prenatal care than whites. Compared with college graduates, those with high school graduation (Prevalence Ratios [PR] 0.87, 95% confidence interval [CI] 0.76–0.99; p = 0.033) or some college education (PR 0.86, 95% CI 0.77–0.96; p = 0.009) were less likely to use virtual visits. A preference for in-person was the most common reason for not pursuing virtual visits (77.1%), followed by no available virtual appointments (29.5%), technology barriers (6.1%), and no private space (1.7%). Individuals with less than or with high school graduation had 4.16 times (95% CI 2.32–7.46; p ≤ 0.001) and 2.72 times (95% CI 1.67–4.43; p ≤ 0.001) greater technology barriers, and 10.03 times (95% CI 3.42–29.46; p ≤ 0.001) and 4.29 times (95% CI 1.56–11.80; p = 0.005) greater likelihood of lacking private space, respectively, while they had a lesser in-person preference.
Conclusions:
In a disrupted health care landscape, barriers to accessing virtual prenatal care may have further exacerbated access to care and effective management of pregnancy among those underserved. The findings provide practical implications for safe and effective prenatal care.
Introduction
Because of the challenges posed to routine prenatal care during the COVID-19 pandemic, virtual care has received particular attention as an effective alternative care model. Understanding patterns of, and barriers to, virtual care is salient vis-à-vis effective prenatal care.
Prenatal care encompasses routine checkups and monitoring pregnancy-related complications, or risk assessment to improve health outcomes related to pregnancy. 1 The United States (U.S.) Department of Health and Human Services notes that prenatal care is an essential part of the pregnancy trajectory and recommends that women receive prenatal care early on and continuously to meet their unique health care needs during pregnancy. 2
While there is a broad consensus that the literature regarding the health benefits of prenatal care is not comprehensive and there is a need for more robust corroboratory evidence, many studies have shown that efficient prenatal care is an important intervention to prevent or ameliorate a range of maternal health conditions, such as anemia, genitourinary tract infection, and obstructed labor. 3 –5 Moreover, previous studies suggest that it is vital to incorporate counseling and professional guidance reflecting individuals' needs to help improve the effectiveness of the prenatal care, while embracing behavioral and social aspects that may further amplify the effects on maternal health. 3,6 –8 It is also noteworthy that prenatal care plays a significant role in helping enhance the health of infants and reduce fatal mortality through proactive screenings and early intervention. 9
Despite the clinical importance of prenatal care for maternal and child health, its provision was interrupted during the COVID-19 pandemic. 10 Swift federal and state responses implemented to protect the public from the virus, capacity reduction at health care facilities, and social distancing practices have intensified barriers to accessing prenatal care. 11 –13 The disruption was also seen as creating risks, including suboptimal management of pregnancy and negative maternal and child health outcomes, raising significant public health concerns. 14
In the challenging health care landscape, virtual care quickly evolved to supplement or act as a substitute for in-person care. 15,16 Even before the pandemic, virtual care was considered a useful option, especially for individuals who faced barriers to accessing health care, such as a lack of resources in rural areas or transportation restrictions. The public health crisis led to a push to further expand virtual care. 16,17 For example, the federal COVID-19 Public Health Emergency Declaration strengthened national efforts to accelerate virtual care accessibility, adjustments to cope with the disruption of health care. 18,19 A population-representative investigation suggested that ∼30% of Americans used virtual care, compared with <10% before the pandemic. 20,21 In the case of prenatal care, a study of local health care systems found that 48.5–82% of patients received virtual care and that those who used virtual visits reported 70–90% satisfaction rates. 17,22 –24 Although in-person care remains the primary care model, the recent changes to health care revealed the critical role of virtual care in addressing prenatal care needs. 17
Despite the growing attention to virtual care as an alternative to in-person care in the public health emergency, there has been a paucity of evidence on population-representative patterns of virtual prenatal care use. 17,20,22,25 Moreover, little is known about the reasons that women do not pursue virtual visits for prenatal care. 26,27 To fill these gaps, our study first investigated the patterns of virtual prenatal care use and examined the reasons that women may not use virtual services.
Methods
DATA
The pooled cross-sectional study used Pregnancy Risk Assessment Monitoring System (PRAMS) from October 2020 through June 2021, drawn from the jurisdictions' birth certificates in the U.S. PRAMS is a nationally representative surveillance system targeted at women who recently gave live birth. The survey collects information ranging from demographics to maternal health attitudes, health status, and obstetric history. Participants were primarily interviewed through a mailed questionnaire and a telephone interview was followed for those who did not respond to mail invitations. The survey adopts a complex sampling design that accompanies stratification and weights, which produces unbiased standard errors and estimates that represent the population. PRAMS included a questionnaire about prenatal care experiences during the COVID-19 pandemic. The information collected through these questions facilitates the understanding of the unique patterns in the use of, and barriers to, virtual prenatal care. This investigation included individuals who reported their prenatal care experiences, yielding a total of 11,829 samples for analysis.
MEASURES
Key outcomes
The key outcome variable was constructed using responses to the question, “During the COVID-19 pandemic, which types of prenatal care appointments did you attend?” The response that indicated any virtual appointment was coded as virtual care or no virtual care, otherwise. Among those who reported no virtual care use were subsequently asked a question, “What are the reasons that you did not attend virtual appointments for prenatal care?” Respondents checked “yes” or “no” to the following items: available virtual appointments from my provider, an available telephone, enough cellular data or cellular minutes, computer or device, internet service, a private/confidential space, or preferred seeing my health care provider in person. With these reports, dichotomous variables were created for a lack of available virtual appointments, preference for in-person care, and a lack of private/confidential place. Technology-driven reasons that include lacking telephone, cellular data, computer devices, or internet access were constructed for a single measure to represent technology barriers.
Covariates
The study included key covariates that potentially influence the use of virtual prenatal care. In demographics, 17,28 –30 age was categorized into <25, 25–29, 30–34, 35–39, and above 39 years old. Race/ethnicity was grouped into Non-Hispanic Whites, Non-Hispanic Blacks, Non-Hispanic Asians, and Non-Hispanic others. Marital status was dichotomized as married or nonmarried. Education was a categorical variable: below high school graduation, high school diploma, some college, and bachelor's degree or above. Insurance was a four-category variable, classified as private, Medicaid, self-pay, or other types of insurance. The Census region had four categories according to the Census regions and Divisions of the U.S., such as Northeast, Midwest, South, and West. Health conditions were also captured, including depression, diabetes, hypertension, obesity, and COVID-19 infection. 17,31 Additionally, the study incorporated past pregnancy experiences. 17,32 Past live births and terminations of pregnancy were coded as 0, 1, or ≥2. The past preterm birth was dichotomized to represent having such a history or not.
STATISTICAL ANALYSES
Bivariate analysis between virtual prenatal care and sample characteristics was performed to describe patterns of virtual care use using independent χ 2 tests. A simple modified Poisson regression was performed to calculate prevalence ratios as a measure of an association between virtual care use and key population characteristics. Subsequently, we employed multivariable regression to estimate adjusted prevalence ratios to see whether the unadjusted associations remain, by accounting for study covariates, such as age, race/ethnicity, marital status, education, census region, insurance, health conditions, and previous pregnancy experiences. Next, among individuals who did not use any virtual care (n = 7,556), the percentage of each reason, such as in-person preference, a lack of available virtual appointments, technology barriers, and a lack of private space, was calculated and graphically presented to describe their distribution. Then, we conducted a series of regression analyses to investigate factors associated with the reasons for not pursuing virtual care. Regression models incorporated survey design variables and weights to derive the population-representative estimates.
The statistical significance was set to a two-tailed p < 0.05. All analyses were conducted using R programming. This study was reviewed by the University of Texas at San Antonio Institutional Review Board and deemed to be research not involving human subjects.
Results
Overall, ∼33.1% of women reported that they used virtual prenatal care (Fig. 1). Virtual care use varied across subpopulations, such as by region, race, age, and education (Table 1). The most frequent reason for not using virtual care was a preference for in-person care (77.1%), followed by a lack of available virtual appointments (29.5%), technology barriers (6.1%), and a lack of private space (1.7%) as shown in Figure 2.
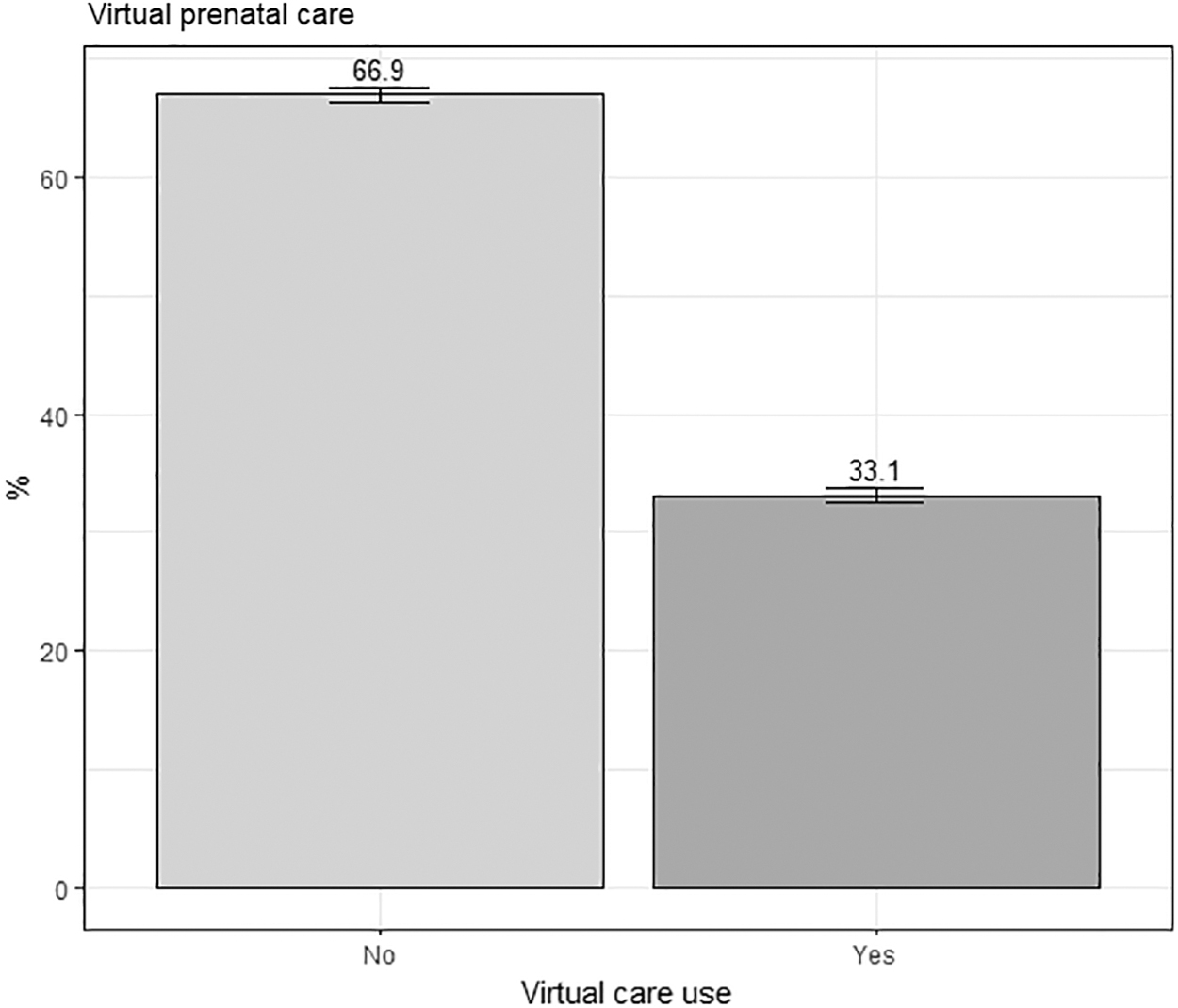
Proportion of virtual visits for prenatal care in October 2020 through June 2021. Data source: PRAMS from October 2020 through June 2021. PRAMS, Pregnancy Risk Assessment Monitoring System.
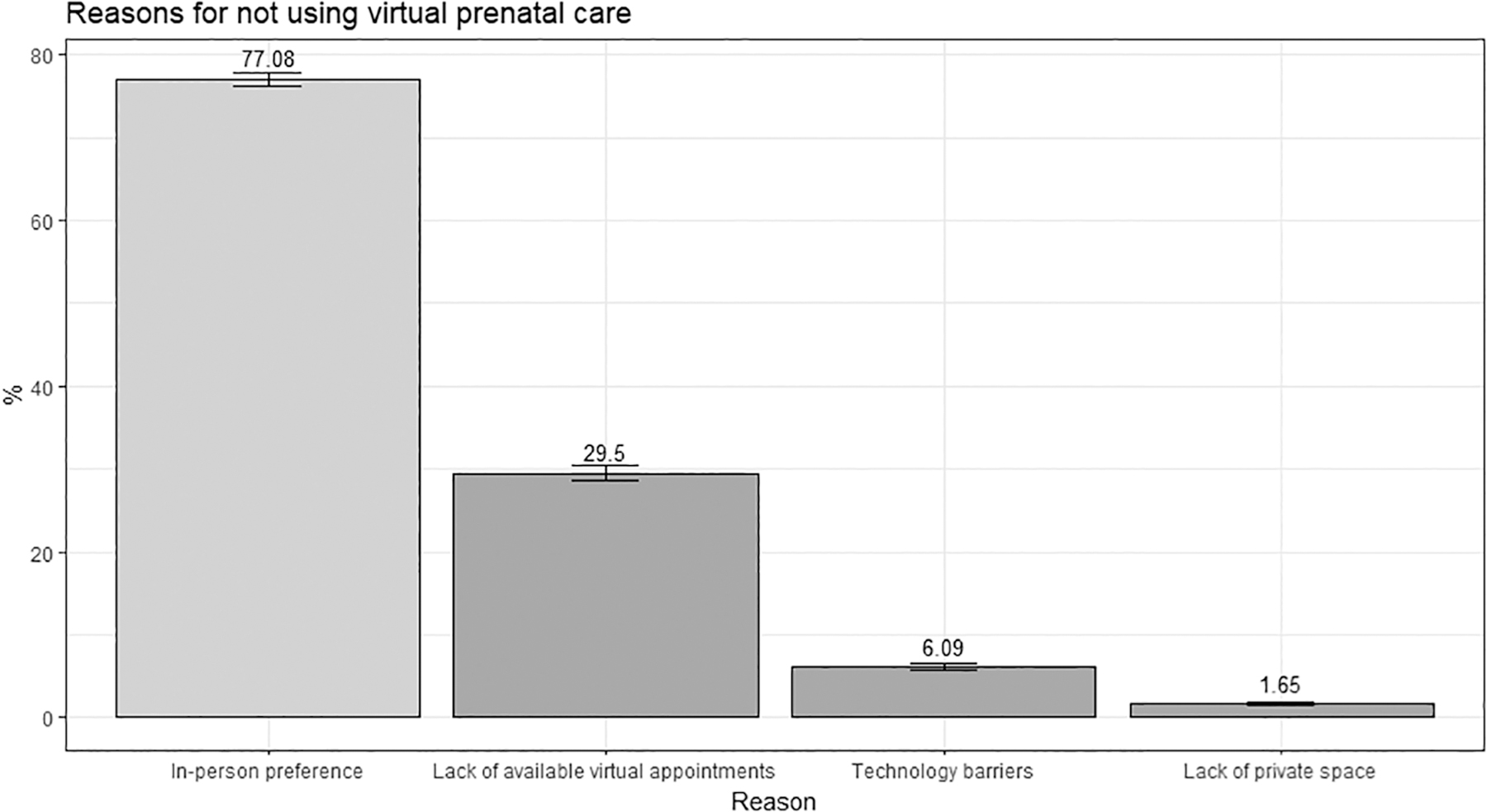
Reasons for not using virtual prenatal care among persons who did not use virtual care. Note: Percentages of reasons do not represent 100% as individuals reported multiple reasons. Data source: PRAMS from October 2020 through June 2021.
Virtual Visits for Prenatal Care by Sample Characteristics
Data source: PRAMS from October 2020 through June 2021.
PRAMS, Pregnancy Risk Assessment Monitoring System; WT, Weighted.
Multivariable analysis showed that individuals from other census regions compared with those from the Northeast, and women who had two or more live births than those who had not given live birth were more likely to use virtual care, which was consistent with the unadjusted estimates (Table 2). However, in a departure from the unadjusted results, the adjusted analysis showed that Hispanic people were more likely to use virtual prenatal care than their white counterparts (Prevalence Ratios [PR] 1.21, 95% confidence interval [CI] 1.08–1.36; p = 0.002). Compared with college graduates, women who had only a high school diploma (PR 0.87, 95% CI 0.76–0.99; p = 0.033) or some college education (PR 0.86, 95% CI 0.77–0.96; p = 0.009) were less likely to use virtual prenatal care.
Predictors of Using Virtual Visits for Prenatal Care (n = 11,829)
Note: statistical significance *<0.05; ** <0.01; *** <0.001.
Data source: PRAMS from October 2020 through June 2021.
CI, confidence interval; PR, Prevalence Ratios.
In reasons for not using virtual care, compared with those with bachelor's degrees, individuals with education below a high school diploma or with high school graduation had 4.16 times (95% CI 2.32–7.46; p ≤ 0.001) and 2.72 times (95% CI 1.67–4.43; p ≤ 0.001) greater risk of experiencing technology barriers, respectively (Table 3). Those who were covered by Medicaid were 1.57 times (95% CI 1.01–2.42; p = 0.043) more likely to face technology barriers than those covered by private health insurance.
Correlates of Reasons for Not Using Virtual Prenatal Care (n = 7,556)
Note: statistical significance *<0.05; ** <0.01; *** <0.001.
Data source: PRAMS from October 2020 through June 2021.
Low educational attainment was also significantly associated with a lack of private space. An education with below a high school diploma or with high school graduation was associated with 10.03 times (95% CI 3.42–29.46; p ≤ 0.001) and 4.29 times (95% CI 1.56–11.80; p = 0.005) greater likelihood of having no private space, respectively.
There were fewer barriers with respect to a lack of available virtual appointments among individuals who graduated from high school (PR 0.82, 95% CI 0.67–1.00; p = 0.045) and for those in the Midwest (PR 0.82, 95% CI 0.70–0.96; p = 0.015) and West (PR 0.78, 95% CI 0.66–0.92; p = 0.004). Hispanics (PR 0.93, 95% CI 0.86–0.99; p = 0.020) and individuals who had an education below a high school diploma (PR 0.87, 95% CI 0.79–0.96; p = 0.007) had a lesser preference for in-person care.
Discussion
This study examined patterns of virtual prenatal care use from October 2020 through June 2021. Also, our study investigated reasons for not using virtual care among those who used only in-person care. Approximately 33.1% of women used virtual prenatal care. Hispanics were more likely to use virtual prenatal care, while those with low educational attainment were less likely to use virtual prenatal care. Among individuals who did not use virtual prenatal care, ∼77.1% indicated that in-person preference was the reason for not pursuing virtual care, followed by a lack of available virtual appointments (29.5%), technology barriers (6.1%), and a lack of private space (1.7%). Reasons for not using virtual prenatal care varied across population subgroups. Notably, women with low educational attainment experienced significant barriers to having technology and private space, while they expressed a relatively lesser preference for in-person care.
PATTERNS OF VIRTUAL VISITS
Earlier studies found that access to care among pregnant women has diminished significantly due to the disruption caused by the COVID-19 pandemic, which had led to greater demand for virtual care. 12,13 Our findings showed that about one-third of women used virtual prenatal care, which is similar to the figure for virtual care use among the general population. 20 Although in-person care remains the primary source of prenatal care and is largely preferred, our analysis suggests that virtual settings perhaps helped ensure continued prenatal care and have been a valuable alternative during the public health emergency. 12,14,22,33
While virtual care evolved, there were observed variations across population subgroups. 28,34 Previous population estimates showed that Hispanics more frequently used virtual prenatal care than their white counterparts, which our analysis confirmed, whereas studies from clinical settings reported mixed findings. 28,34 –37 Also, there are differences in virtual care use across education levels: there was lower utilization among individuals with low educational attainment. These findings suggest that those of low socioeconomic status continue to experience various barriers to accessing virtual care, even during the global pandemic, in which they have also been shown to be vulnerable to infection from the novel virus and poor health outcomes. 20,38 Compared with the Northeast, other census regions used virtual care much less. Although more studies are needed to understand the regional variations, individuals' vigilance toward the virus, along with policy or political environments, perhaps influence individual behaviors, leading to regional differences in virtual care utilization. 39
REASONS, NOT PURSUING VIRTUAL VISITS
Most pregnant women (77%) did not opt for virtual care because of their preference for in-person visits, consistent with previous reports. 7,22,40 The strong preference for in-person is not surprising given the potentially high-risk conditions that can occur as part of pregnancy. The intense preference for in-person care could also be attributed to a desire for better communication about personal concerns related to pregnancy that may not be shared effectively in a remote setting. 22 Hispanics showed a relatively lower preference for in-person, which reflects our finding that this ethnic group is more likely to use virtual visits than non-Hispanic whites. The unique conditions Hispanics face, such as job inflexibility in a large proportion of the essential workforce or transportation barriers, may play a role in a lesser preference for in-person visits. 41,42 Also, those who had not graduated from high school had a lesser preference for in-person visits. While these variations will be further explored in future investigations, the present study provides evidence of varying patterns in the preference for in-person prenatal care.
A lack of technology, private space, and virtual appointment availability can present further practical barriers to virtual visits. The barriers to accessing technology were more prevalent for those with less education than those with more education, suggesting that individuals with less education do not have necessary technical support, such as phone, internet access, and data availability. Disparities in accessing technology often referred to as a digital divide—are a critical public health concern, as they can lead to inequitable care, such as a lack of informed patient–provider communications. 43 Our study also found that individuals covered by Medicaid had greater technology barriers. Medicaid accounts for almost half of the insurance coverage in the U.S. While a large proportion of individuals receive government assistance for prenatal care, these individuals may have practical difficulties in making virtual visits. These findings suggest that disparities in technology access remain among a subgroup of the population and continued efforts to reduce such gaps are required.
Those with low educational attainment also reported greater barriers to accessing a private/confidential space. The lack of private space has emerged as a major concern with respect to the security and safety of patients in a virtual setting, as many people were sheltering at home during the COVID-19 pandemic. 44,45 Studies have indicated that there are challenges emerging in remote communications between patients and providers on sensitive health-related information. 45,46 In a qualitative study, women expressed their hope of having a private space in which they could speak to providers about personal issues, including domestic violence during pregnancy without fearing of their spouse's interference or threat. 46 Policy will need to consider assistance for socioeconomically disadvantaged individuals who need a secure space for virtual care.
Our findings also showed regional variations in the virtual appointment availability. Compared with the Northeast, the Midwest and West showed a lower likelihood of there being no available virtual appointments and a greater preference for in-person care. Varying demand for virtual prenatal care coupled with levels of policies and institutional responses to the novel virus may be a potential explanation for these variations across regions. 47 Further studies examining individual and institutional factors are needed to confirm or improve our findings. Additionally, individuals with depression reported barriers, including technological, private space, and virtual appointments. In rising mental health problems during the pandemic, the health care and public health community proposed the expansion of virtual care provisions for mental health, as remote settings proved an effective source of care. 48 –50 Considering that psychosocial problems, such as depression, are important complications of pregnancy, ensuring virtual care could help women effectively manage their psychological wellbeing and pregnancy.
POLICY IMPLICATIONS
Virtual care has largely been considered supplementary when there are challenges to receiving traditional in-person care, particularly for those who have barriers to accessing care. Such a perception may have shifted to the more proactive use of virtual care as a sustainable care model in uncertain health care environments. Nonetheless, this study suggests that the majority of people prefer in-person care. Although in-person care is likely to remain the primary care model, virtual prenatal care has provided another useful choice. 51
One-third of participants reported a lack of available virtual appointments, suggesting that many women might adapt to virtual visits for prenatal care once it becomes available. Providers' clinical perspectives, insurance policies, and technical capabilities may also influence virtual care availability, which policymakers should consider promoting virtual care. Notably, socioeconomically disadvantaged individuals experience significant barriers to accessing virtual prenatal care, including a lack of technology and private space, while they reveal a relatively lower preference for in-person care. Our findings exhibit gaps that the health community needs to address.
LIMITATIONS
Our study has some limitations. First, although PRAMS is a nationally representative database, reliance on self-reports has inherent limitations, such as potential recall bias and social desirability issues. Individuals may under or over-report barriers to technology, private space, or virtual appointment availability. Second, our study did not go into further detail concerning the reasons for not pursuing virtual care. For example, a lack of available virtual appointments could be related to technical capabilities or organizational/institutional responses to the pandemic. Third, although our analysis included various reasons for not using virtual visits, this study was not comprehensive to include other potential reasons, such as gaps in knowledge or acceptance of technology. 29
Also, although our analysis incorporated important factors that could affect measuring the association, there is a potentially unmeasured issue, which could have confounding effects and potentially undermine our findings. Lastly, although the study findings suggest important correlates for virtual prenatal visits and the reasons for not pursuing them, this pooled cross-sectional design did not intend to examine a causal relationship.
Despite these limitations, our study makes significant contributions to understanding the patterns of virtual visits and reasons that women do not pursue them. Future studies are warranted to further investigate the prospective relationship and contextual factors that may influence individuals' choice of virtual prenatal care.
Conclusions
While the COVID-19 pandemic disproportionately affected those underserved, barriers to accessing virtual prenatal care may have further exacerbated their access to care and effective management of pregnancy. The study findings provide policymakers with practical implications to address barriers to virtual prenatal care.
Footnotes
Authors' Contributions
J.L. led the study conceptualization, design, data analysis, and article preparation. W.S.M. contributed to interpretation of results and critical review editing.
Disclosure Statement
No competing financial interests exist.
Acknowledgments
We thank the PRAMS (Pregnancy Risk Assessment Monitoring System) Working Group for its role in conducting PRAMS surveillance.
Note. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Funding Information
No funding was received for this article.