
Abstract
Background:
Unequal access to telemedicine services exacerbates health inequities and was evident at the start of the COVID-19 pandemic. We sought to explore whether unequal access persisted within a classical hematology division beyond the peak of COVID-19.
Methods:
Patient demographics by virtual visit type (telephone only [TO] or video only [VO]) between March 2020 and December 2021 were analyzed using adjusted odds ratio (aOR).
Results:
Of 8,207 patients, 18.4% had TO and 28.4% had VO visits. Fewer Black (21.8%; aOR 0.5 [0.4–0.62]), Hispanic or Latino (18.8%; 0.45 [0.34–0.59]), Spanish-speaking (7.6%; 0.32 [0.19–0.54]), high school (21.2%; 0.64 [0.52–0.78]), and older (24.2%) patients used VO compared with White (30.6%), English-speaking (29.5%), college (31%), postgraduate (34.9%), and younger (35.4%) patients.
Conclusions:
Groups that historically experience health inequities had fewer VO visits during and beyond the pandemic peak. Thus, there is a need to continue digital inclusion efforts to promote video access equity.
Introduction
The COVID-19 pandemic prompted an expedited shift toward telemedicine use to allow for physical distancing. Historically, widespread adoption of telemedicine was limited by lower reimbursement rates and strict regulations. 1 Emergency COVID-19 pandemic policies allowed for temporary pay parity between virtual and in-person visits as well as loosened regulations that facilitated telemedicine expansion. 2
Telemedicine, however, can be a mechanism to either mitigate or aggravate health disparities. Although expansion of telemedicine increases overall access to care, this increase is not always equally distributed. Older patients, those from racial minority and lower socioeconomic groups, and areas with limited health care resources are less likely to have broadband internet access, and thus less access to virtual platforms. 3 –5 Patients from advantaged backgrounds, therefore, benefit disproportionately from telemedicine expansion, widening care gaps. 3
Moreover, within telemedicine, disparities in access to video and telephone visits also exist. Video visits are generally understood to be more desirable as a visual physical examination is possible, and offers a better replication of the “face to face” interaction than telephone visits. 6 However, studies published in the early COVID-19 pandemic demonstrated lower use of video visits by individuals who were older and from racial minority groups. 7,8 Whether this disparity persisted or diminished months to years after the pandemic began has not been established. Classical hematology as a specialty relies heavily on laboratory-based diagnosis and is readily suited to telemedicine. Thus, it is critical to evaluate the adoption of telemedicine services within specialties such as classical hematology that are apt for ongoing use of telemedicine.
Methods
Electronic health record data were obtained for “pandemic” patient encounters occurring at Brigham and Women's Hospital Division of Hematology between March 19, 2020 (date division switched to virtual visits) and December 31, 2021. Encounters between January 1, 2019 and March 18, 2020 were obtained to serve as a “pre-pandemic” comparator. Patient age, gender, race and ethnicity, preferred language, education level, employment status, zip code (merged with the American Community Survey data for zip code level median income), and patient portal activation status were extracted.
Data were analyzed at the patient level. The type of visit a patient had during the study period (telephone only [TO], video only [VO], or a combination of in-person and/or telemedicine visits), was determined by visit billing codes. Differences across demographic categories were tested for significance using Kruskal–Wallis and chi-square tests. Multivariable regression modeling was used to compare VO with TO visit use within demographic categories and reported as adjusted odds ratio (aOR). Approval was obtained from the Dana Farber Cancer Institute Institutional Review Board.
Results
A total of 8,307 prepandemic visits and 15,108 pandemic visits were included in the analysis. Almost all visits (99.9%) were in-person prepandemic compared with 42.4% in-person, 26.9% TO, and 30.6% VO during the pandemic. Pandemic patients were younger than prepandemic patients (51 vs. 55 years; p < 0.001). There were more females (71.5% vs. 66.6%, p < 0.001) and fewer non-English-speaking patients (6.1% vs. 8.6%, p < 0.001) during the pandemic. Otherwise, there was no difference in the racial composition or median income level of pandemic and prepandemic patients (Table 1).
Demographic Characteristics of Patients Who Completed Prepandemic Compared with Pandemic Visits
Comparing prepandemic-only and postpandemic-only patients.
Note: Boldened p-values are significant at the 0.05 significance level.
There were 8,207 patients who completed 15,108 pandemic visits. More patients had VO (N = 2329, 28.4%) than TO (N = 1509, 18.4%) visits. Table 2 and Figure 1 show the demographic composition of patients completing VO and TO visits. VO were younger than TO patients (46 vs 58 years, p < 0.001). Overall, majority (89%) had activated patient portals. Patients with an activated portal were more likely to have VO visits compared with those without an activated portal (30.8% vs. 8.6%, aOR 5.49 [4.18–7.2]). Overall, 63.6% of pandemic patients self-identified as White, 13.6% Black, 10.6% Hispanic, and 12.2% other.
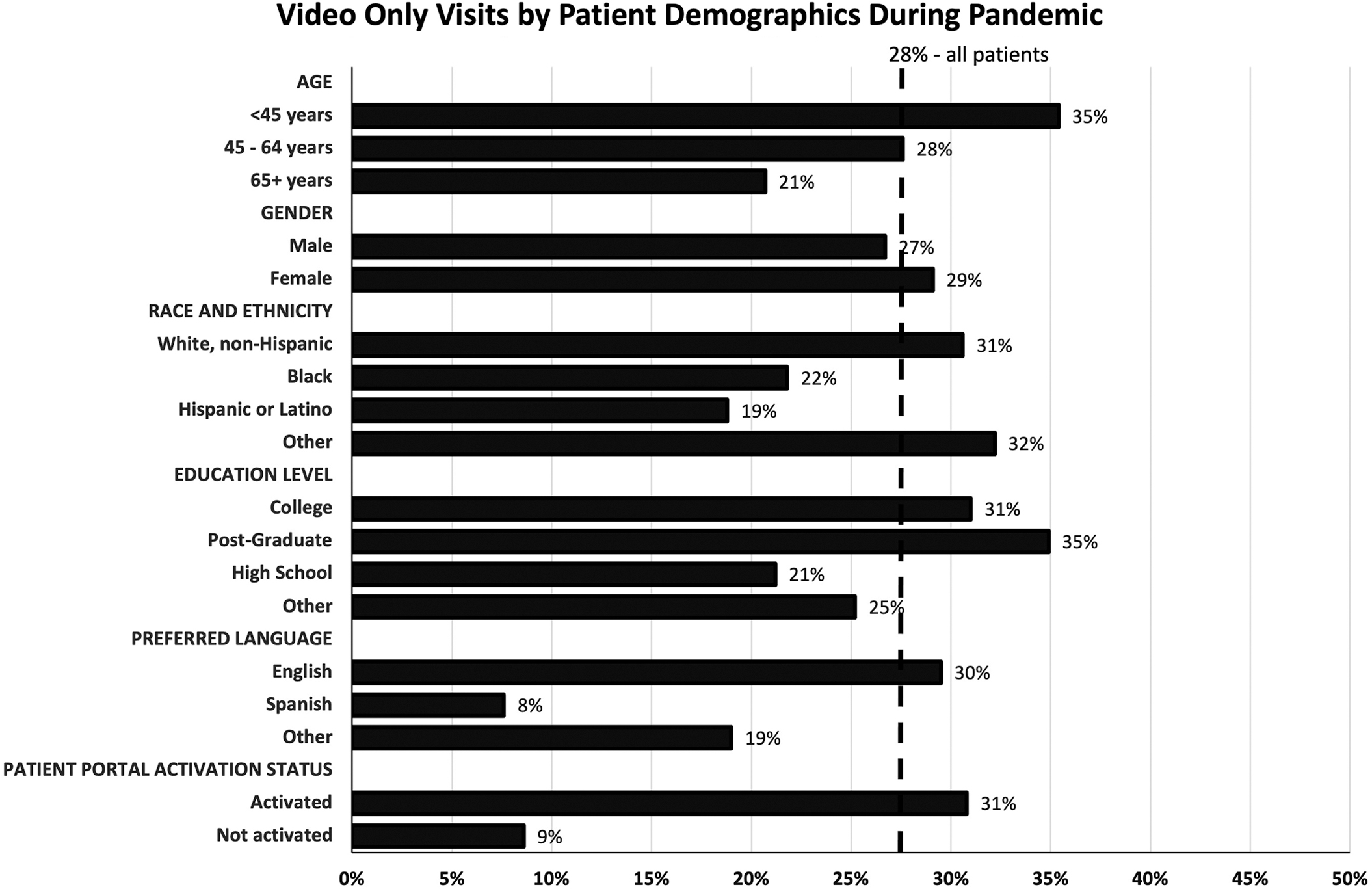
Bar graphs represent percentage of patients completing video-only visits by gender, race and ethnicity, education level, preferred language, and patient portal activation status Dotted line represents the percentage of all patients who completed video-only visits.
Demographic and Socioeconomic Characteristics of Patients Completing Video-Only and Telephone-Only Visits During the Pandemic (March 2020–December 2021) and Adjusted Odds Ratio of Video Visit Use by Demographic Groups
N of all patients including those who had a combination of in person and/or telemedicine visits during the study period.
Reference group for aOR analysis.
aOR, adjusted odds ratio.
Note: Boldened p-values are significant at the 0.05 significance level. Boldened aOR indicates an associated significant p-value at the 0.05 significance level. aOR of completing video visit over telephone visit compared with reference group after controlling for other variables in table.
Fewer Black (21.8%, aOR 0.5 [0.4–0.62]) and Hispanic or Latino (18.8%, aOR 0.45 [0.34–0.59]) patients had VO visits compared with White (30.6%) patients (Table 2). Patients with a high school (21.2%, aOR 0.64 [0.52–0.78]) or other level of education (25.2%, aOR 0.77 [0.64–0.93]) were less likely to have VO visits than patients with a postgraduate (34.9%, aOR 1.04 [0.84–1.29]) or college (31%) degree. In addition, 29.5% of English-speaking patients had VO visits, but only 7.6% of Spanish-speaking patients had VO visits (aOR 0.32 [0.19–0.54]). Median household incomes approximated from patient zip codes were significantly higher in patients with VO than with TO visits ($97,404 [77,484–120,613] vs. $90,279 [67,805–109,149]; p < 0.001).
To assess whether disparities were dissipating with increasing experience with telemedicine, patient characteristics were compared in 2020 versus 2021. TO visits decreased from 42.6% of visits in 2020 to 16.8% in 2021 and VO increased from 30% to 34.2%. Patient portal activation status did not change significantly. However, differential use of VO and TO visits remained from 2020 to 2021. For example, Black patients had an aOR of 0.44 [0.33–0.59] in 2020 and 0.39 [0.29–0.52] in 2021 of using VO visits compared with White patients. Spanish-speaking patients had an aOR of 0.35 [0.17–0.75] in 2020 and 0.3 [0.16–0.56] in 2021 compared with English-speaking patients. VO use by older adults decreased even further from 2020 to 2021 with those >65 years having an aOR of 0.49 [0.37–0.66] in 2020 and 0.22 [0.16–0.31] in 2021 compared with those <45 years.
Discussion
This study highlights utilization of telemedicine modalities by demographics and shows that older adults and non-English-speaking patients lost access to classical hematology care during the COVID-19 pandemic. Moreover, individuals from groups that have historically experienced health inequities in the United States, including the elderly, Black and Hispanic individuals, non-English speakers, individuals with lower education attainment, and lower median incomes, were less likely to receive care through VO and more likely to utilize TO compared with patients who were younger, non-Hispanic White, English speaking, and had higher levels of education and median incomes.
Previous studies had shown this disparity in video visit use at the beginning of the pandemic when specialties were troubleshooting the use of telemedicine platforms. 7,8 Our findings indicate that disparities remained and for older adults, even worsened over time despite improved adaptation of video visit platforms by the division. As such, structural inequities remain a vital consideration for both overall access to classical hematology care as well as the type of visit utilized.
Given that video visits typically offer better clinical interaction than telephone, the observed disparity may exacerbate underlying health inequities if not addressed. This highlights the need for digital inclusion efforts focused on historically disadvantaged groups and centered around broadband internet and device access and affordability as well as digital literacy at the patient, institutional, clinician, and policy levels. 9 Notably, video visits are already showing promise in use and satisfaction among patients with Sickle Cell Disease who are predominantly Black and face many barriers to hematology care. 10
In addition, with the return to no or markedly lower reimbursement rates for telephone visits, the differential reimbursement disincentivizes providing care through the telephone, even if that is a patient's only means of access. As increasing access to video visits will undoubtedly take time, disincentivizing telephone visits could pose a further barrier to telemedicine for vulnerable populations who may not have access to video visits and exacerbate structural racism, ageism, classism, and other inequities.
The persistence of differential access observed in this study over a year into the pandemic makes it clear that although classical hematology is likely to continue to utilize telemedicine, caution must be taken that this does not become another venue to ingrain structural bias, including racism and ageism.
Footnotes
Authors' Contributions
Conceptualization (supporting), writing—original draft (lead), methodology (lead), and formal analysis (supporting) by M.A.O. Methodology (supporting) and writing—original draft (supporting) by L.E.M. Data curation, methodology (supporting), and formal analysis (lead) by S.R. and D.S.N. Supervision (supporting) and writing—review and editing (supporting) by M.A. and J.A.R. Conceptualization (lead), methodology (supporting), supervision (lead), and writing—review and editing (lead) by A.L.L.
Disclosure Statement
M.A. is a member of the scientific advisory board for Pharmacosmos A/S, AMAG, Global blood therapeutics, and Fulcrum pharmaceuticals. The remaining authors declare no competing financial interests.
Funding Information
No funding was received for this article.