
Abstract
Introduction:
Native American Veterans are the most rural and experience heightened risk for mental health (MH) challenges while facing significant health care inequities and access barriers. Rural Native Veterans (RNVs) have experienced historical loss and racial discrimination, contributing to mistrust of Veterans Health Administration (VHA) and other Federal systems. Telemedicine, including video telehealth (VTH), can improve access to MH care for RNVs by addressing barriers. Understanding the cultural context and existing community resources can improve engagement and implementation efforts with RNVs.
Objective:
This article describes a model of culturally centered MH care and a flexible implementation approach, Personalized Implementation of Virtual Treatments for Rural Native Veterans (PIVOT-RNV), used to disseminate the model.
Methods:
Participants included four VHA sites serving large RNV populations where PIVOT-RNV was applied to expand the availability of virtual solutions, including VTH, for RNVs. A mixed methods formative evaluation tracked VTH utilization and used provider and RNV feedback to inform iterative process improvements.
Results:
Where PIVOT-RNV was used, number of providers using VTH with RNVs, number of unique RNVs receiving MH care through VTH, and number of VTH encounters with RNVs grew annually. Provider and RNV feedback highlighted the importance of addressing the unique barriers and cultural context of RNVs.
Conclusions:
PIVOT-RNV demonstrates promise for improving implementation of virtual treatments and access to MH care for RNVs. The integration of implementation science within a cultural safety framework helps address specific barriers to adoption of virtual treatments for RNVs. Next steps include expanding PIVOT-RNV efforts at additional sites.
Introduction
Native Americans have served in the U.S. Armed Forces for over 200 years, 1 with the highest per capita military service of any racial or ethnic group. 2 Military service carries significant honor and status in many Native American communities, as it is consistent with the highly valued warrior identity. 3 Native Veterans (defined by Veterans Health Administration [VHA] as American Indian, Alaska Native, and Native Hawaiian Veterans but used in this article to refer to those individuals in the lower 48 states) experience higher rates of posttraumatic stress disorder (PTSD) and other mental health (MH) challenges than Veterans of other racial and ethnic groups. 4,5 Native Veterans are more than twice as likely to endorse thoughts of suicide as non-Hispanic White Veterans, 5 and rates of suicide among Native Veterans have risen in recent years. 6
Despite an increased risk for MH challenges, Native Veterans face significant barriers and health care inequities compared with other Veterans. 7,8 Native Veterans are the most rural of any racial or ethnic Veteran group, with 49% of Native Veterans residing in rural and highly rural areas. 9 Rural residence is associated with notable geographic barriers to accessing health care, particularly MH care, and significant provider shortages. 10 Furthermore, Native Veterans are more likely to lack health insurance, have a service-connected disability, or be unemployed and are less likely to use VHA benefits. 1 The combination of increased needs with increased and unique barriers are notable drivers of these inequities.
Access barriers encountered by Native communities must be viewed within cultural and historical contexts, particularly as Native communities have endured threats to Indigenous vitality, including forced relocation from tribal lands and attempted genocide. 11 Many Native Veterans experience substantial issues around cultural misunderstandings, trust, and engagement concerns with VHA health care and other Federal systems. 12,13 Native Veterans report barriers to accessing VHA health care, including lack of VHA outreach to Native communities and Native Veterans' perceptions that the VHA system is difficult to navigate and culturally insensitive. 13 Furthermore, members of Native communities are more likely than non-Hispanic Whites to report problems with transportation, work or family responsibilities, difficulty finding childcare, and concerns about cultural misunderstandings and racial discrimination. 12
It is imperative that health care systems, including VHA, emphasize addressing or reducing access barriers for Native Veterans, which includes attending to specific cultural and contextual dynamics that may impact service delivery, engagement, and community wellbeing.
VIDEO TELEHEALTH
Telemedicine, including video telehealth (VTH), can improve access to MH care for Native Veterans by reducing barriers (e.g., cost, travel, time) and improving quality of care. 14 For decades, VHA has used VTH to increase access to care, particularly for rural Veterans. VTH enables a patient and provider to meet virtually, using secure videoconferencing technology. Early VTH was often conducted clinic to clinic, meaning the patient and provider were located at different VHA clinics. Patients could receive care at a clinic closer to their home, which reduced geographic/distance barriers and decreased time away from family or work responsibilities. VTH also helped address provider shortages or limited availability of specialty care, particularly in rural areas. Recent technological developments have resulted in VA Video Connect (VVC), VHA's VTH platform, which enables a Veteran to connect with a VHA provider from any private, convenient location (e.g., home, work) and further addressing or eliminating some barriers to care. 15
VVC has enhanced security features (e.g., end-to-end encryption, integrated e-911), and VHA has a digital tablet loan program that allows Veterans to request a device for VTH appointments to enhance accessibility of VTH. 16 Although VTH can be one solution for increasing access to care, Native communities face challenges to virtual treatment, including reduced access to internet compared with both urban and rural non-Native households. 17 Efforts to engage Native Veterans would be improved by addressing these unique access barriers while emphasizing culturally adapted models of care.
MODEL OF CULTURALLY CENTERED MH CARE
To meet the unique needs of Native Veterans, a model of culturally centered MH care that leverages telehealth technology while addressing the specific sociocultural, historical, and contextual factors of Native Veterans is critical. This model is the culmination of a two-decade collaboration between VHA's Office of Rural Health-Salt Lake City Rural Resource Center, and the Centers for American Indian and Alaska Native Health. 18 This approach acknowledges and integrates evidence-based Western medicine, traditional healing, and rural Native communities' strengths.
The first telepsychiatry clinics focused on expanding care to Native Veterans with PTSD. 19 Early efforts demonstrated the feasibility of VTH for Native Veterans and informed later VTH expansion, highlighting the importance of local partnerships between VHA and Tribal communities as well as the value of an initial assessment to better understand the local context. 19 –21 The initial VTH clinic implementation involved identification and training of local VHA-based peer outreach workers (i.e., Tribal Outreach Workers) who acted as liaisons between Native Veterans and VHA to facilitate engagement in treatment and wider access to VHA benefits and services. Including outreach workers, who were often Native Veterans with knowledge of both military and Native cultures, optimized the impact of outreach efforts and identified areas for improvement. 22
Initial work used a hub and spoke approach and showed important impacts in terms of improving access, service utilization, and cost, 23 although widespread dissemination across the VHA system faced significant challenges. As overall VTH adoption increased, amplified by VHA's development of more mobile and agile video platforms (i.e., VVC), we sought to expand VTH for Native Veterans, transitioning to a broader-based dissemination approach to engage and train a greater number of VHA providers in supporting Rural Native Veterans (RNVs). To shift the culturally centered telepsychiatry model developed for RNVs while capitalizing on expansion in the use of mobile video platforms and addressing widespread dissemination challenges, a telehealth implementation approach was developed to expand access to MH care, Personalized Implementation of Virtual Treatments for Rural Native Veterans (PIVOT-RNV).
This model draws upon implementation science, which has long been used to improve and expedite uptake of health innovations. 24 For example, Implementation Facilitation, a multifaceted process specifically intended to support integration of new clinical practices in VHA, includes a variety of strategies that can be combined to meet the needs of a particular innovation or health care system. 25
The purpose of this article is to describe the PIVOT-RNV approach and examine the utility of implementation science for dissemination of the culturally centered model of MH care for RNVs. Results from a mixed methods formative evaluation that tracked VTH utilization and informed iterative process improvements are presented.
Methods
A telehealth implementation approach was developed for RNVs (Fig. 1) as part of a quality improvement effort to expand utilization of VTH among Native Veterans receiving care within VHA. The project was determined to be a non-research Quality Improvement VHA operations activity and did not require IRB review. We started with Personalized Implementation of Virtual Treatments for Rural Veterans (PIVOT-R), an implementation approach guided by Implementation Facilitation that addressed the specific challenges of implementing virtual treatments (e.g., evolving technology, provider concerns about therapeutic alliance, and changes in guidelines or policies) and needs of rural Veterans. 26,27 PIVOT-R relies on collaboration between External Facilitators, project staff outside the local site with expertise in implementation science and telehealth technology, and Internal Facilitators, individuals at the site who are empowered to support local expansion of VTH. PIVOT-R uses reach, effectiveness, adoption, implementation, and maintenance 28 to guide an iterative evaluation process where feedback was continually shared with partner sites and used to refine the implementation approach.
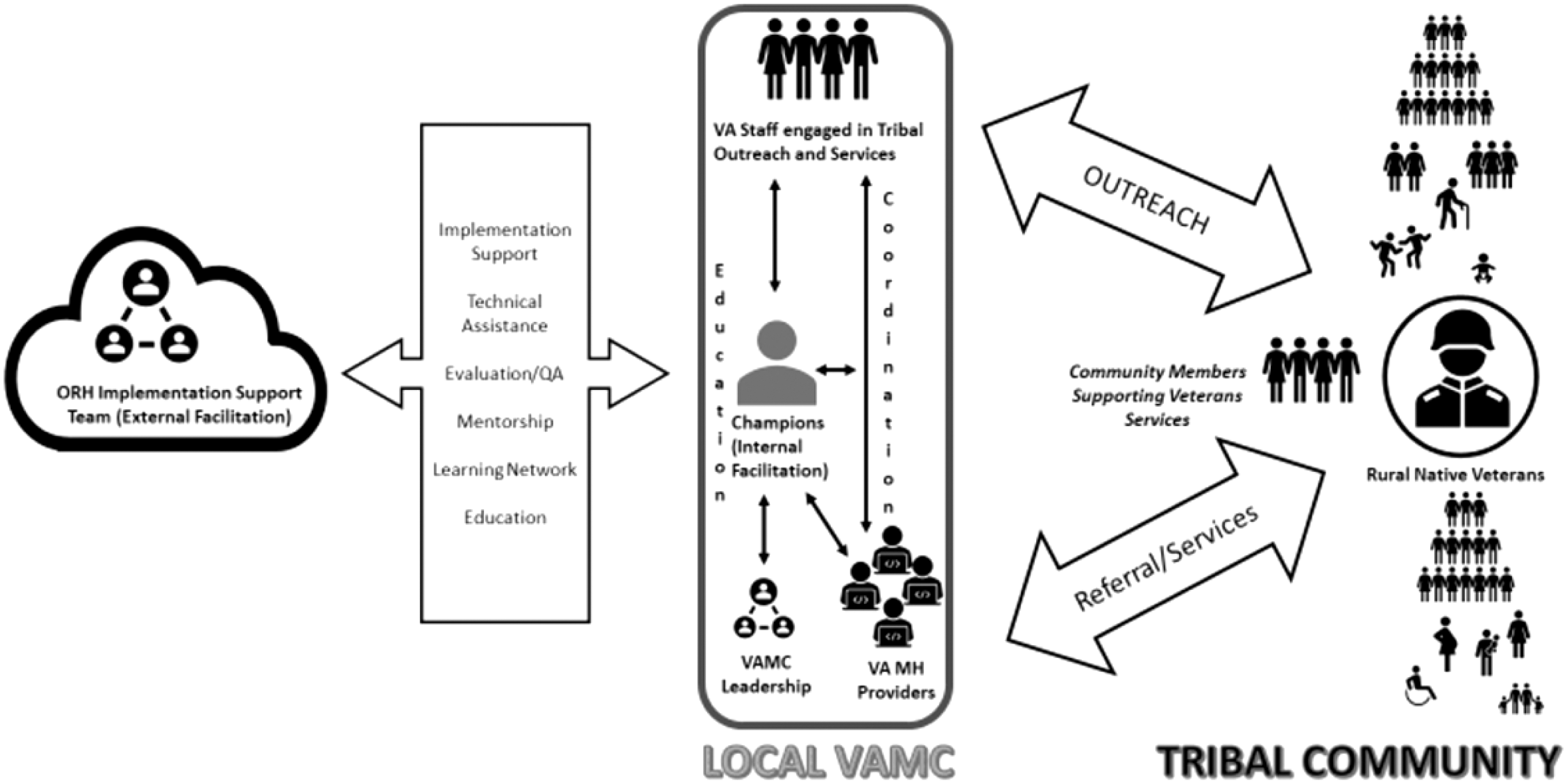
Implementation Model for increasing access and engagement for RNVs to Virtual VHA Mental Health Care. ORH, Office of Rural Health; QA; RNVs, Rural Native Veterans; VAMC, VA Medical Center; VAMH, VA Mental Health.
PIVOT-RNV was developed from a formative evaluation process that used early experiences implementing VTH at sites with RNVs and feedback from Internal Facilitators, champion providers, and RNVs, to evaluate efforts and inform changes. Throughout this iterative process, adaptations were made to meet the unique needs of Native Veteran populations and communities. Notable changes include adding Internal Facilitators focused on Tribal outreach and community members supportive of RNVs, integrating training and education on Native culture, and devoting extra attention to building trust and relationships with key personnel at partner sites. Participants included four VHA sites in the Midwest, Southwest, and Rocky Mountain regions that were mentored in the PIVOT-RNV implementation approach. Potential partner sites with significant RNV populations were identified, and information about the project was shared during introductory meetings. Site participation entailed designating Internal Facilitators, local staff dedicated to VTH or RNVs, who agreed to attend scheduled meetings with External Facilitators.
External Facilitators assisted with identification and engagement of Internal Facilitators who were most often existing staff with prior roles, experience, or interest in supporting VTH or RNVs. To optimize their effectiveness, ideal Internal Facilitators also possessed some social capital, cultural knowledge, and credibility with additional training provided as needed.
Since we began this work, our approach to meet the diversity and equity needs of Native Veterans transitioned from emphasizing cultural competency to a cultural safety framework, which acknowledges sociohistorical drivers underpinning health inequities, examines power structures that undermine equity, and promotes an ongoing bidirectional process of acknowledgment, curiosity, and respect. 29 Our PIVOT-RNV efforts are informed by a cultural safety lens and aim to be receptive and responsive to specific cultural and contextual considerations.
The PIVOT-RNV approach (Table 1) focuses on addressing challenges related to technology adoption and strategies to increase engagement within the cultural context of RNVs and their communities. This is accomplished through collaboration and mentoring of local partners, trust and relationship building with providers, and consultation with and supervision of individual sites as well as larger collaborative meetings designed to share successful practices among sites. PIVOT-RNV acknowledges the historical trauma and loss experienced by Native communities and works to address the warranted mistrust toward federal systems or entities, which may influence Native communities' openness and receptivity to engaging with VHA. The approach prioritizes collaborative relationships, trust building, and mutual learning. We adapted efforts to be culturally aligned, collaborating with Tribal outreach and Native community members on development of implementation strategies, VTH messaging, and images. By learning how to effectively expand the availability of VTH for RNVs, we seek to enhance agency and self-determination, helping RNVs to make informed choices about their MH care.
Personalized Implementation of Virtual Treatments for Rural Native Veterans
RNV, Rural Native Veteran; VTH, video telehealth; VVC, VA Video Connect.
The formative evaluation involved ongoing collection of mixed methods quantitative and qualitative data. Quantitative data on VTH utilization were obtained from the VHA Support Service Center Capital Assets Databases. External Facilitators created monthly data reports on VTH utilization for each partner site, which were shared and reviewed to track progress and inform subsequent implementation efforts. Qualitative data included feedback about implementation progress from Internal and External Facilitators during biweekly meetings, periodic reflections with Internal Facilitators conducted by evaluation team members, and quarterly community of practice meetings with all partner sites. Evaluation team members conducted mixed methods interviews with RNVs who had used VTH for MH care to understand cultural factors and experiences using VTH. Evaluation team members created quarterly Rapid Reviews, site-specific reports that included VTH use and implementation successes or strong practices, which were shared with site partners.
Results
We applied PIVOT-RNV for implementation of VTH at three sites in fiscal year (FY) 2019 and an additional site in FY 2020. In FY 2018, before starting PIVOT-RNV efforts at partner sites, 8 providers used VTH with 12 unique RNVs during 89 encounters. Implementation efforts are ongoing with partner sites still in the implementation phase.
QUANTITATIVE DATA
Throughout RNV implementation, all partner sites increased each year on three VTH metrics: number of providers using VTH with RNVs, number of unique RNVs receiving MH care through VTH, and number of VTH encounters with RNVs. In 2019 (3 sites), 31 MH providers served 42 unique RNVs during 228 VTH encounters. In FY20 (4 sites), 242 MH providers served 296 unique RNVs during 1,445 VTH encounters. In FY21, 357 MH providers served 548 unique RNVs during 3,878 VTH encounters.
QUALITATIVE DATA
Feedback from Internal Facilitators, many of whom were also MH providers, highlighted challenges and unique factors when engaging RNVs for VTH. Interviews with RNVs enhanced our understanding of contextual factors and benefits of using VTH for MH care. Information from providers and RNVs was a key component of the iterative approach, used to refine the PIVOT-RNV process and highlight important lessons (Table 2).
Lessons Learned and Important Considerations When Implementing Virtual Treatments for Mental Health Care with Rural Native Veterans
RNV, rural Native Veteran; VHA, Veterans Health Administration.
The importance of building and nurturing relationships was reiterated throughout the evaluation process, prompting PIVOT-RNV team members to deliberately foster egalitarian partnerships that involved self-reflection, flexibility, and respect. Internal Facilitators repeatedly indicated preference for a collaborative approach focused on team efforts over individual accomplishments, allowing a fuller appreciation of how each team member's unique abilities and contributions supported implementation efforts. Some RNVs described how being offered VTH for their MH care improved their opinion of VHA because it demonstrated consideration for their needs and comfort. RNVs also discussed the value of community and in-person interactions for Native communities, encouraging us to integrate low-tech outreach in the community rather than the default expectation that Veterans must come to VHA.
Feedback from RNVs, their providers, and Internal Facilitators confirmed the value and importance of cultural safety when engaging Native communities. Moving forward, we aim to integrate cultural safety more fully throughout the stages of implementation, engaging in reflective practice about our own role and position within the sociopolitical and historical contexts relevant to the Veterans we serve.
Discussion
Results indicated that PIVOT-RNV had a positive impact on VTH utilization for MH care among RNVs and provided many lessons learned for continued improvements in access and quality of care. Our approach focused on the specific needs and barriers facing RNVs, leveraging virtual treatments (i.e., VTH) to connect VHA providers with RNVs needing care. We intervened at the local level to develop culturally aligned strategies tailored to address specific needs identified during the needs assessment.
Descriptive data showed increased VTH utilization among RNVs and their providers at all partner sites, suggesting some benefit of PIVOT-RNV, although the unprecedented virtualization of care in response to the COVID-19 pandemic makes it difficult to distinguish the impact of implementation efforts from the overall increase in VTH. Regardless, the importance of addressing barriers to care for Native Veterans is particularly salient within the context of the pandemic, during which Native communities experienced disproportionately negative impacts. Native Americans had a mortality rate that was twice that of non-Hispanic White individuals, 30 and one study found an association between historical trauma and increased risk of psychological distress among Native individuals after the start of the pandemic. 31 Tailored interventions, such as PIVOT-RNV, are critical strategies to help mitigate negative effects and health inequities during widespread weather or health emergencies.
Qualitative feedback highlighted the importance of relationship building and cultural safety for engaging Native communities. Our implementation efforts build upon previous work to expand care for Native Veterans 17,18,21 and offer important new information about effective strategies for addressing barriers to care, which have been well documented for both Native 12,13 and rural Veterans. 32 Despite recent widespread increase in the use of VTH, 33 rural and highly rural areas continue to struggle with limited availability of Wi-Fi and high-speed internet. 17 While targeted education and training can help improve willingness to try or use virtual care, the digital divide must be addressed to facilitate broader uptake and ensure equitable access to health care. PIVOT-RNV's inclusion of an initial needs assessment to understand unique cultural and contextual considerations while emphasizing collaborative relationships aims to directly address barriers to care that RNVs face (i.e., cultural insensitivity, mistrust, lack of Wi-Fi or high-speed internet). 12,13,17
Fostering strong relationships with Internal Facilitators allowed us to engage in ongoing and honest discussions about race and culture. These conversations also included how to approach mistrust due to historical trauma when doing outreach, which in turn optimized the outreach and implementation efforts of Internal Facilitators.
LIMITATIONS AND ADDITIONAL CONSIDERATIONS
We outline a flexible approach for implementing virtual care with RNVs, which can be adapted for other patient populations, particularly those with unique cultural and contextual considerations. However, PIVOT-RNV was notably developed and refined within VHA, which benefits from “anywhere-to-anywhere” legislation enabling a provider and Veteran patient located in any state or U.S. territory to participate in care. Many states do not approve VTH across state lines for non-VHA providers, which can limit the availability of virtual care. Despite differing state guidelines, virtual treatment can be a powerful tool to enhance access and quality of care for patients experiencing barriers or inequitable access. We also deliberately partnered with sites serving large RNV populations to demonstrate impact, which means sites with lesser concentrations of RNVs may have different experiences applying PIVOT-RNV.
FUTURE DIRECTIONS
We focused on VTH as one avenue for increasing access to MH care for RNVs and will continue our efforts by expanding the PIVOT-RNV approach at additional VHA sites. We will further apply and tailor the PIVOT-RNV approach, integrating cultural safety throughout implementation, 29 specifically examining the impact of PIVOT-RNV as more care transitions to a hybrid of in-person and virtually delivered care. Future research could also broaden to include the role of virtual treatments besides VTH, including apps or web-based programs, to enhance or extend care for Native communities. However, any research or implementation focused on technology-based solutions needs to address infrastructure limitations facing many RNVs. 17 Finally, although PIVOT-RNV was specifically developed and applied for RNVs, this approach may hold promise for implementing virtual treatments with other underserved populations and communities, including other Veteran populations, and Native and rural communities.
Conclusions
While there are overarching values that may be shared by many Native Veterans, every individual is unique. As every Tribe is distinctive, and every reservation is a sovereign nation with its own culture and government, it is crucial to continually engage in bidirectional learning and remain receptive and responsive to specific cultural and contextual considerations. When working to engage RNVs, or any population with specific cultural considerations and barriers, it is critical to consider how sociocultural and historical dynamics interact with accessibility and engagement in MH care to facilitate contexts that allow individuals and communities to pursue ways of living that they value.
Footnotes
Ethics Statement
This article describes efforts that were determined to be non-research Quality Improvement VHA operations and did not require IRB review.
Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This work is funded by grants from the VA Office of Rural Health and Veterans Health Resource Center-Salt Lake City. This work is also supported by the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN13-413) and the VA South Central Mental Illness Research, Education and Clinical Center.
The opinions expressed are those of the authors and do not necessarily reflect those of the Department of Veterans Affairs, the U.S. government, University of Colorado, or Baylor College of Medicine.