
Abstract
Background:
There is growing interest in the incorporation of video consultations in primary care. Remote medical devices used for remote physical examinations are a new complementary addition to these consultations and may increase their effectiveness. This study examines a social behavioral-technological model by the factors predicting the acceptance of video consultation with or without a technological medical device, their perceived ease of use (PEU), and their perceived usefulness (PU), as well as social behavioral factors: trust and shared decision making.
Methods:
We conducted an online survey among patients who had visited a physician during 2021 and had the option to receive video consultations with or without remote medical devices. Structural equation modeling was applied to assess the proposed model of predicting the extent of future telemedicine use.
Results:
Among the 1,198 patient responders, the intention to use telemedicine video consultation had a significant positive association with trust, shared decision making, PEU, and PU and with high socioeconomic constructs. The intention to use telemedicine video consultation with a medical device had a significant positive association with shared decision making, PEU, and PU. The statistical results suggest a good fit with the proposed models.
Conclusions:
The proposed social behavioral-technological model demonstrated that to successfully adopt video consultations and new remote medical devices in primary care, there is a need for trust and shared decision making to be established in patient–physician relationships.
Introduction
Previous studies have identified patient acceptance of telemedicine technology or lack of it, as one of the most crucial factors toward utilization. 4 –6 Some health care studies on technology adoption are based on a theoretical framework. 7,8 The technology acceptance model (TAM) can help us better understand barriers and promoters for adoption of technology. The TAM, proposed by Davis et al. 5 and Venkatesh and Davis, 9 is a well-established theory for predicting and interpreting users' adoption of and behavior toward information technology. 10 The model suggests that perceived usefulness (PU) of telemedicine and its perceived ease of use (PEU) can predict the technology's future utilization. PEU is defined as the extent to which an individual believes that using the system will be free of effort, while PU is defined as the extent to which an individual believes that using the system will enhance the outcomes.
The TAM model cannot explain all the variability in use of new technologies and other factors are needed. Some previous consumer and telemedicine studies supported integrating trust with the TAM model, arguing that trust relates to PEU and PU. 10 –13
Trust has long been regarded as an important aspect of therapeutic caregiving. 14 Studies have identified a clear correlation between patients' trust in their physician and their preference for treatment, which may result in productive interactions and patient-centered care. 15 The definition of patient's trust adopted in this study is patient's belief in the credibility and reliability of the physician's words, behavior, and treatment, expecting that physicians will act in the patient's best interest, in support of their health. 16 Literature suggests 17 that patient's trust in the physician is associated with confidence in the offered treatment.
In this study, we added to the existing extended model of TAM and trust, the shared decision making (SDM) concept. When faced with the task of making health care decisions, shared decision making has been shown to increase the patient's satisfaction, to improve the quality of care, and reduce costs, 18 as well as improve affective-cognitive outcomes. 19 Moreover, patients who are more engaged in their health care decision making are more likely to experience confidence in treatment decisions, satisfaction with treatment, and trust in their physician. 20 SDM is defined as an approach in which clinicians share with their patients the best available evidence, to support their patients in considering options and to achieve an informed preference. 21 Indeed, in a previous qualitative study we conducted, 22 patients in focus groups indicated that trust and shared decision making were factors in choosing the type of visit (telemedicine or in-clinic consultation).
This study was conducted with the Meuhedet Healthcare Services (MHS), a health maintenance organization in Israel, which provides universal, mandatory, tax-funded health care coverage from birth onward for Israeli residents. Approximately 1.3 million members of all ages receive care from MHS. Patients have the option to receive, at no cost, health care consultation services from their primary care physician, either in-clinic or remotely—digitally through a video consultation and with a new enhanced option using a medical home device (Tytocare™).
Physicians use the mobile device to facilitate noninvasive medical examinations of patients, as part of the video consultation. The device is designed to capture and transmit visualization of ear, throat, and skin images, and heart and lung auscultations, including heart rate detection and temperature taken by an infrared transdermal thermometer. 23 Studies indicate that it is also feasible for parents to perform at home physician-guided medical examinations, 23 and it has a superior mean comparative diagnostic score with a high reliability otoscope diagnosis. 24 The physician controls the device remotely and instructs the patient how to perform each examination.
In a previous study that explored the attitudes and challenges of physicians in a telemedicine service in Israel, the main factor stated by the physicians was their difficulty making a diagnosis from a distance, due to the inability to perform a physical examination in the telemedicine setting. 25 Increasingly, utilization of remote medical devices such as Tytocare will overcome this adoption barrier.
The aim of this study was to better characterize video consultation and remote home medical device users, and to assess future intention to use such services, in a sample of the Israeli adult population. This study seeks to do so using the model of TAM and trust and an additional variable: shared decision making, in explaining the intention to use video consultation (Fig. 1). We used the suggested model in three sampled groups: experienced video consultation users, medical device users (Tytocare), and nonexperienced users. We hypothesized there will be differences between the groups due to their different experience.
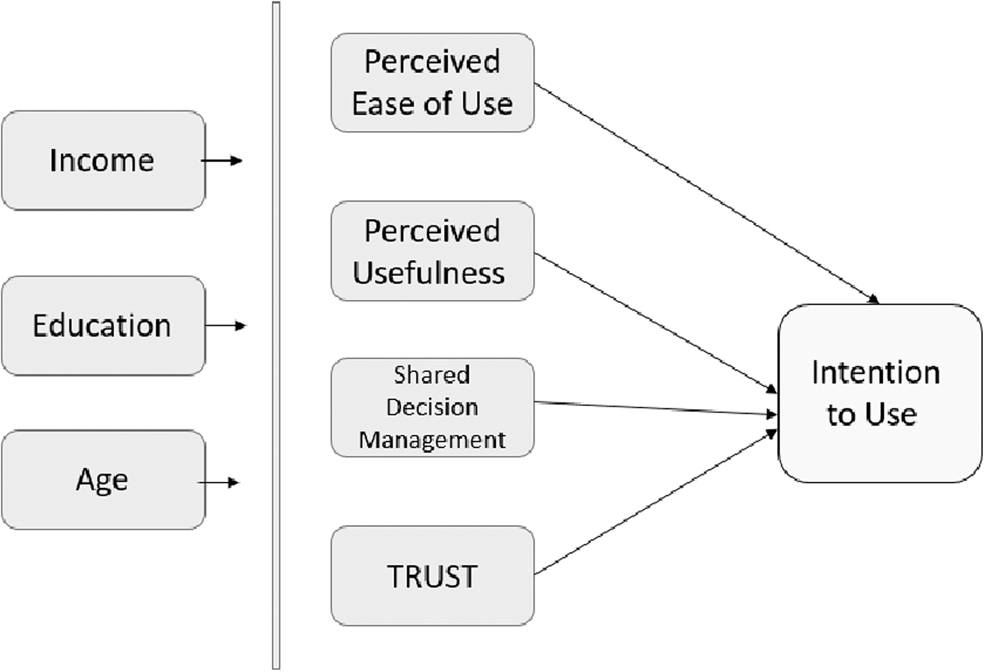
Study model.
Methods
The study included a survey that explored possible factors affecting the intention and actual use (ACT) of video visits, with or without a medical device. The ethical committees of MHS and the University of Haifa approved the study.
The target population included adults older than 18 years, who were insured by a health maintenance organization, who had a medical visit between April 2021 and December 2021.
To investigate patients' perceptions of their intention to use video consultations, a self-reported, anonymous questionnaire was developed. The survey included the TAM, trust, and SDM variables. Respondents rated items related to the following measures: ACT, intentions to use (Intention), PEU, PU, shared decision making (SDM), and trust (TRUST). Table 1 presents the variable names and examples of items. Each item had 3–6 questions. The TAM items PU, PEU, and Intention were adopted from previous research, 5,26 and were used to measure TRUST 26 and SDM. 27
Variables Assessed and Item Description
ACT, Actual Use; PEU, Perceived Ease Use; PU, Perceived Usefulness; SDM, Shared Decision Making.
Although validated by prior research, the variables were examined to ensure content validity and reliability within the context of this study and in Hebrew, because validity sometimes differs across different populations. 28 Respondents answered the questionnaire by rating each item on a 5-point Likert scale ranging from “totally disagree” to “totally agree.” Scores were developed by computing the mean of all the items that constituted each theoretical dimension. In addition, respondents provided demographic information (age, gender, family status, socioeconomic status, education, and health).
An initial pre-test of the tool was conducted with five volunteers to gain an understanding of the time necessary to complete the survey and clarity issues regarding the questions. This was followed by a preliminary cross-sectional survey of 137 users. The data collection commenced, after which the questionnaire was once again examined to ensure its content validity and reliability. The internal consistency of the instrument was assessed by calculating Cronbach's alpha values for each theoretical variable, as shown in Table 1. The construct validity of the model was evaluated using interterm correlation analysis.
Following the pre-test, language modifications and design minor modifications were made to the questionnaire and answer choices, and then a full-scale data collection was performed. To collect the data, the MHS provided three samples for surveying: nonusers: 14,059 patients, randomly sampled, who did not use any digital health, video consultation users: 13,799 patients, randomly sampled, who used at least once a video consultation, and Tytocare device owners: 4,535 patients who own a Tytocare device.
All patients received an email message inviting them to participate in a survey about digital health. A second message was sent after 7 days reminding patients to complete the questionnaire. Among the 1,198 patients who answered the questionnaire, 421 were nonusers of video consultations (using only traditional in-clinic visits), with an effective response rate of 33%; 506 used video consultations, with a response rate of 27%; and 271 were users of video consultation with Tytocare medical device, with a 17% response rate.
STATISTICAL ANALYSIS
An analysis was performed using the statistical tests described below, and structural equation models (SEMs) were built using the Lavaan R package. 29 First, the model was assessed, performing standardization and clustering of items to measures, using a pre-defined allocation of items. Then reliability of the scales was performed. A correlation matrix, using hierarchical clustering on the individual items to validate the pre-defined allocation, was explored. Eventually, respondents' sociodemographic factors were analyzed, frequencies were reported, and χ 2 tests were performed for all differences between the types of medical visits. Analyses were conducted using two-sided tests for significance and with p < 0.005. Analyses were performed using IBM SPSS V27. Then a model was built for three samples: telemedicine video consultations users, nontelemedicine users, and telemedicine video consultation users with the medical device (Tytocare).
We fit 3 SEMs for each of the 3 groups: nonusers, experienced users, and Tytocare users, to predict the extent of telemedicine future use. Each model included the individual items, measures as latent variables, covariance between the measures, and additional background variables: age, gender, income, and education level. Post hoc modifications included the removal of the satisfaction measure and the addition of background demographic variables (education, age, gender, and income). We conducted an additional step in which we pruned the models by removing insignificant variables and creating much simpler models for descriptive purposes.
Results
Among the 1,198 patients who answered the questionnaire, nearly 58% of respondents were women, and the average age was 48.8 years; Table 2 depicts the distribution of socioeconomic characteristics of survey respondents. Among the respondents, above-average income was noted among the medical device users (Tytocare).
Socioeconomic Characteristics of Survey Patients by Visit Type
The main results of models of the survey are summarized in Table 3. A SEM analysis was used to analyze the models of the three types of users to identify relationships between the constructs. All three models presented a good fit to the data following goodness of fit (GFI), normed fit index (NFI), comparative fit index (CFI), and root mean square error approximation (RMSEA) parameters (CFI >0.9, RMSEA <0.08, and standardized root mean square residual [SRMR] <0.049), as shown in Table 4. In all three cases, the models showed a significant Chi-square statistic. However, in large sample sizes, it was acceptable, and the model fit to data was good. 30 Figures 2, 3, and 4 illustrate the model, and the coefficients are used to observe relationships.
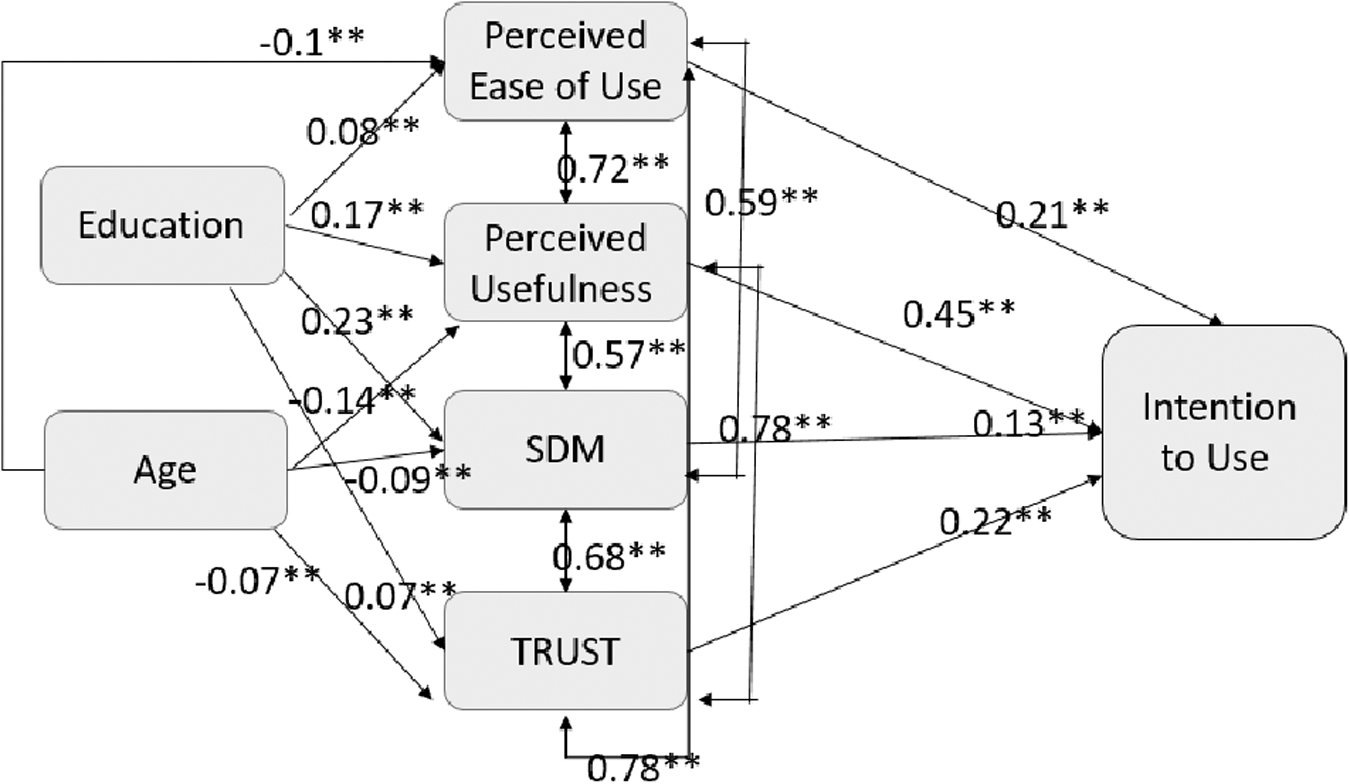
Prediction of video consultation use—Experienced Users. SDM, Shared Decision Making. **p < 0.01.
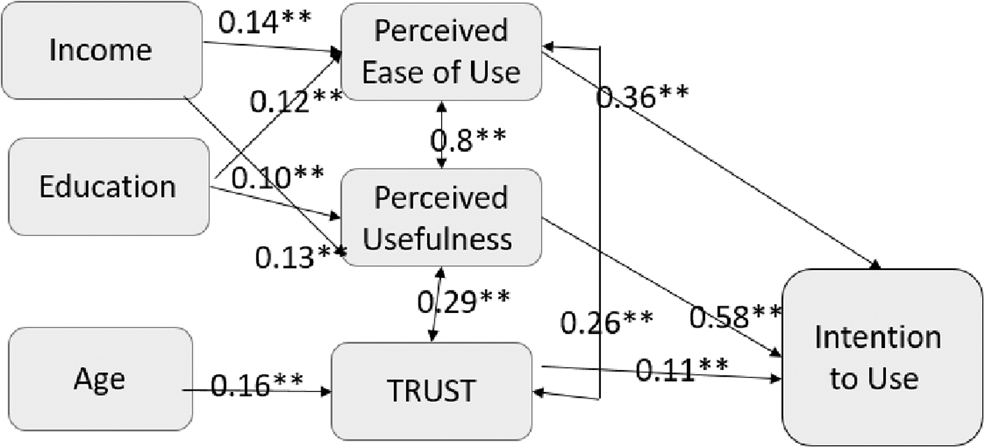
Prediction of Video consultation use—Nonusers. **p < 0.01.
Summary of the Pruned Structural Equation Model Models' Results
Values are regression estimates and asterisks indicate the significance (*** p < 0.001, ** p < 0.01, * p < 0.05).
NA, non applicable.
Summary of the Structural Equation Model Models' Fit Indices
CFI, comparative fit index; RMSEA, root mean square error approximation; SRMR, standardized root mean square residual.
In the model presenting the variables associated with the use of video consultation without the Tytocare device (Fig. 2), both trust and SDM had a strong positive association on intention to use, together with the traditional TAM variables: usefulness and ease of use. Education had a positive association on independent variables, whereas age had a negative association on them.
In the nonusers of video consultations model (Fig. 3), trust was significant and expanded the traditional TAM. Socioeconomic variables had a positive association on the independent variables.
In the Tytocare user model (Fig. 4), SDM played a significant role in patients' intention to use the device; however, trust and the socioeconomic variables were insignificant.
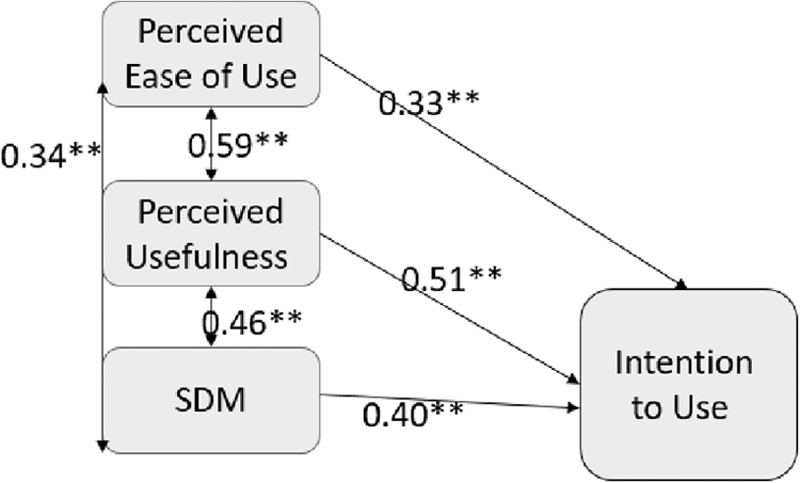
Prediction of Medical Device use. **p < 0.01.
Discussion
This study proposed to better understand patients' future intentions to use telemedicine video consultations with or without a medical device in primary care post-covid-19. Our findings show that PEU and PU are two important antecedents that directly influence behavioral intention to use telemedicine. This study assessed additional variables—trust and SDM. Overall, the study survey generated several models.
The first model suggests that for experienced users of video consultations, PEU, PU, trust, and SDM have significant impacts on behavioral intention to use video consultations. In addition, both trust and SDM have significant positive effects on PEU, and PU, separately. Perceived ease of use was one of the key factors determining PU. The second model for nonexperienced video consultation users generated different results. Perceived ease of use, PU, and trust had a significant impact on behavioral intention to use video consultations, whereas SDM was not significant. In addition, trust had significant positive effects on PEU and PU, separately.
Our research found that trust has an apparent direct positive effect on PU and behavioral intention to use video consultation. As patients become more confident that the technology can meet their expectations, their perceptions of complexity and uncertainty regarding this change and usage are reduced. Our findings, as in previous studies, indicate that trust is an important variable in the quality of care and satisfaction with health care systems. 31 –33 Therefore, physicians have a role in strengthening their patient's trust, to ensure that they will use video visits in the future.
SDM also plays an important role, determining how patients choose to utilize health care services. Patient's willingness to utilize remote care, through video consultation, is affected by their physician's attitude. Thus, patient's trust in the physician and treatment may also be affected by the physician's enabling shared decision-making during a clinical encounter, which in turn positively predicts patient adherence to treatment. 34 Willingness to be more involved in decision making predominately characterizes the younger, higher educated, and higher income population, 35 –37 matching also characteristics of digital health users. 38 Our study supports this, as education and age had significant effects on PEU, PU, trust, and SDM, for experienced video consultation users. Not surprisingly, users of video consultation were undertaken by higher socioeconomic status patients.
Another model this study proposes is a model explaining intention to use the Tytocare medical device. This acts as an example case for understanding patients' intentions to use remote medical devices, accompanying video consultations with their primary-care physician. We found PEU, PU, and shared decision making were significantly associated with future intention to use video consultation with medical device, whereas trust was not. We postulate socioeconomic variables and trust were insignificant, due to the homogeneous users' profile and the small size of sample of Tytocare users.
A remote medical device, such as Tytocare, allows primary-care video consultations to become more data rich, as patients can use tools to remotely provide physicians with ear and throat images, breathing sounds, heart rate, blood oxygen levels, and other parameters. 39,40 Therefore, the understanding of patient intentions to use these devices is crucial. Remote physician-guided patient use of a sometimes-intrusive medical device (e.g., for ear or throat examinations), can be challenging and complicated, both for the physician and patient. In addition, new technologies were claimed to risk nonverbal communication and intuitive knowledge being lost during the therapeutic process. 41 Good communication, which is a basis of SDM, was found to improve the patient's future intention to use such a device.
Patients are increasingly involved in their treatment, and a patient-centered approach is advocated by key health organizations and institutions throughout the world. 42,43 In coming years, patients will take on an important participatory role, becoming a full partner in making decisions regarding his or her treatment. 44,45 Indeed, in systematic reviews, it has been shown that patients, who are more actively engaged in their health care decisions, experience better health outcomes and health care experiences. 46
Remote care consultations using video, whether with or without a medical device, require patients and physicians to communicate clearly and unhurriedly, as calm and attentive video consultations were found as a key motivator in adoption of the technology. 47 The design of the operating function of the system should be easy and useful and health services should consider how to guide patients and physicians to increase trust and SDM. Video consultations with a medical device place an additional responsibility on the physician to guide the patient to perform actions the physician initially performed himself at the clinic. For example, physicians may need to guide the patient to direct the camera or the remote medical device, such as how to place an otoscope in a child's ear, without harming the eardrum.
Physician–patient communication and patient satisfaction and engagement in treatment are dependent upon trust and good interpersonal relationships 48 and may help to overcome such barriers in adoption of telemedicine technology. Training of health care professionals, emphasizing communication skills, can be one of the tools toward implementation.
This study has several limitations. First, certain population groups were not represented in our sample. As the survey was conducted in Hebrew through a web panel, non-Hebrew speakers, such as monolingual speakers of Arabic and Russian, and elderly patients who did not have a computer could not answer the survey. Moreover, since telemedicine has the potential to be an effective tool for overcoming inequality gaps and underserved patient populations with poorer access to health, future studies with more non-Hebrew speakers need to explore the usage characteristics of these populations. Future studies should endeavor to explore other factors, such as demographics and health literacy, on the intention to use and recommend adoption of services. Another possible limitation is that the Tytocare device must be purchased privately by the patient at a cost of 60 USD, whereas video consultations have no additional cost; thus, certain patient groups, such as those of lower socioeconomic status, might be less able to use it for remote care. 49
Finally, a significant effort was made to ensure higher participation rates, by providing three subsequent reminders to the respondents. Ultimately, the result of low response rate in this study may have introduced a nonresponse bias, as individuals who possess a higher inclination toward technology may have different responses and a greater willingness to use digital tools. However, it should be noted that the response rates among the three groups (digital: 4.56%, nondigital: 5.05%, and Tytocare: 4.01%) are similar and not statistically significant (p = 0.0974, χ 2 = 4.658).
The similar low rates of response suggest respondents generally were not interested in answering the survey and are not biased in the way they answered the study variables. Therefore, these results may not be biased due to these low rates. To further validate the results, future research could utilize an internet panel with a higher response rate and participants from other health insurance providers.
Conclusion
Use of telehealth increased, as more patients accessed health care through video consultations during the COVID-19 pandemic. This research added 2 constructs, trust and SDM, to the TAM. In the context of video consultations in Primary Healthcare, our findings show that this model improves the level of explaining the variability in use of telemedicine.
Footnotes
Acknowledgments
We thank MHS for their contributions to this work and to the Sarid Institute for conducting the survey.
Authors' Contributions
I.M. contributed to the study conception and design, acquisition, analysis, and interpretation of data, and drafting and revising of the article. I.C. contributed to analyzing and interpreting the data, and drafting and critically revising the article. O.B.A. contributed to analyzing and interpreting the data, and drafting and critically revising the article. A.H. contributed to the interpretation of data, and critically revising the article. All authors provided critical feedback and edits to each version of the article. All authors read and approved the final article, and agreed to be accountable for all aspects of the work.
Data Sharing
The data used in this study are not publicly available or accessible.
Disclosure Statement
No competing financial interests exist.
Funding Information
The survey was supported by the Meuhedet Research and Medicine departments, No. 430024315.