
Abstract
Introduction:
Patient satisfaction has been shown to changes based on the distance a patient to see their physician. We sought to examine the effects of telehealth on patient satisfaction.
Methods:
We examined patient satisfaction survey scores from outpatient clinics at University of California, San Francisco. Patient home and clinic addresses were used to calculate distance in kilometers (km). Outcomes were “top scores (9–10)” and “low scores (<9).”
Results:
Of 103,124 evaluations that met inclusion criteria, those where patient traveled >100 km for in-person visits had more top scores (84%) than those traveled <10 km (80.2%). Relative to in-person visits, telehealth was associated with an increased odds (odds ratio [OR]: 1.48) of receiving a top score at all distances. Those traveling >100 km had the highest odds of top score for telehealth (OR: 1.86).
Conclusions:
Patients receiving care through telehealth, particularly those far from the outpatient clinic, are more likely to provide high patient satisfaction scores for the visit provider.
Introduction
Better patient–physician relationships have been linked to improved health outcomes. 1 Health systems measure this relationship through core satisfaction metrics that are predicted to play an increasing role in physician incentives. 2 Patient satisfaction has been shown to inversely correlate with distance traveled to see their physician—the farther a patient travels for his or her care, the less likely they are to be satisfied. 3 Telehealth, meanwhile, has shown a mixed impact on patient satisfaction. 4 -6 We sought to demonstrate a relationship between the distance traveled by the patient and satisfaction with their ambulatory visit. We hypothesized that telehealth visits will have higher satisfaction scores than in-person visits, particularly for patients who live far from the clinic.
Methods
We examined patient satisfaction survey scores from all outpatient clinics at University of California, San Francisco (UCSF), from January 1, 2017, to January 1, 2019. We chose a pre-COVID-19 period to reduce confounding related to the pandemic. We analyzed patient and provider demographics including age, gender, race/ethnicity, medical specialty, and payor. Visit type was dichotomized to “In-person” and “Telehealth.” Patient home and clinic addresses were used to calculate distance in kilometers (km).
If a patient rated a physician multiple times, the first score was chosen and the others excluded. Those with missing data and providers with <30 reviews were excluded. The primary outcome was provider score (1–10) based on the question “How would you rate the provider overall on a scale of 1–10, with 0 being the worst and 10 being the best.” Provider scores were dichotomized to “top scores (9–10)” and “low scores (<9).”
Descriptive statistics were used to characterize the study cohort. Continuous variables were reported as means and standard deviation. We performed a univariate analysis of patient and provider factors associated with “top rating.” A two-sided p-value <0.05 was considered statistically significant.
Results
A total of 103,124 evaluations met inclusion criteria. The majority of patients identified as white (65.1%) and female (56.9%) with a median (interquartile age range of 59 years [41, 69]) (Table 1). Most visits were in-person (97.7%) with a median travel distance of 31.8 km. Patients who traveled >100 km for in-person visits had higher rates of top provider score (84%) than patients who traveled <10 km to clinic (80.2%). Increased satisfaction with increasing travel distance was observed (Table 1). Relative to in-person visits, telehealth visits were associated with an increased odds (odds ratio [OR]: 1.48; confidence interval [CI]: 1.3–1.68; p < 0.001) of receiving a top score at all distances.
Odds of Receiving Top Rating
Includes patients who selected “Other”, “Prefer not to say”. Those with missing data were excluded.
Factors that predict receiving top provider score (9 or 10 out of 10) in telehealth and in-person visits.
CI, confidence interval; IQR, interquartile range; OR, odds ratio.
Those traveling >100 km had the highest odds of top score for telehealth compared with in-person visits (OR: 1.86; CI: 1.78–1.95; p < 0.001). Analysis by California county showed similar high scores for counties far from San Francisco (Fig. 1).
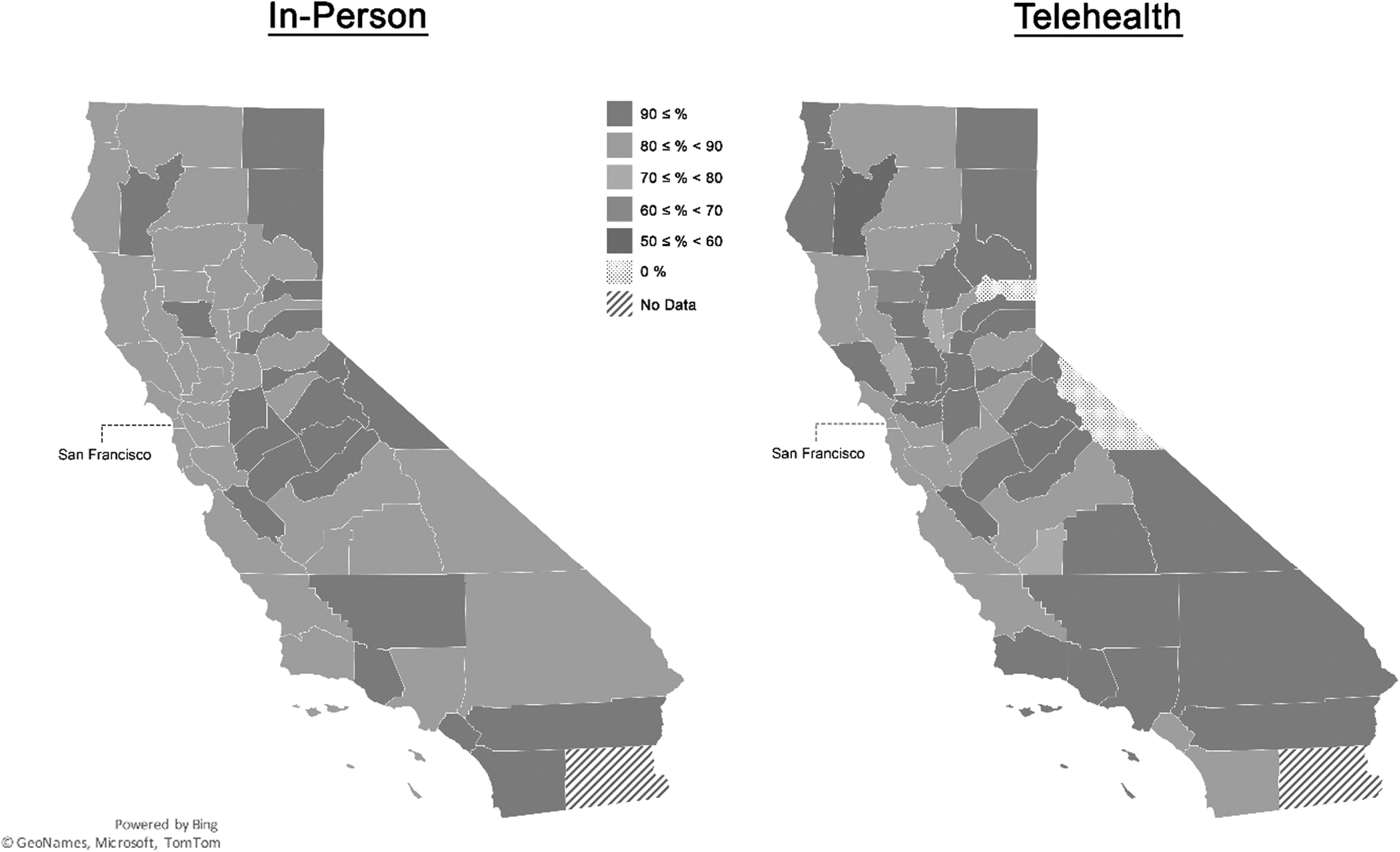
Rate (maximum 100%) of top provider score (9 or 10 out of 10) among in-person and telehealth visits by California County.
Discussion
Among patients seeking outpatient care, those seen in telehealth were more likely to provide a high satisfaction score. Interestingly, patients who live farther from the outpatient clinic were overall more satisfied for both in-person and telehealth visits. High satisfaction among the cohort traveling from a greater distance may be due to increased medical complexity, availability of a specialty clinic, or difficulty in finding a local provider. The beneficial effect of telehealth is amplified among the population traveling from a greater distance—the odds of receiving a top satisfaction score for telehealth compared with in-person increased with distance. The most satisfied patients are those who live >100 km from clinic and are seen in telehealth with 90% providing a top provider score.
LIMITATIONS
Study data were collected before the COVID-19 pandemic when telehealth was less common. The increase in telehealth since that time may affect current trends in satisfaction.
Conclusion
Patients receiving care through telehealth, particularly those patients who live far from the outpatient clinic, are more likely to provide high patient satisfaction scores for the visit provider. This represents a modifiable factor to improve patient satisfaction, particularly among those patients who may have barriers to care.
Footnotes
Acknowledgments
We gratefully acknowledge the assistance of Nizar Hakam, Behnam Nabavizadeh, Natalie Rios, and Michael Sadighian. All were from the UCSF Department of Urology and were otherwise uncompensated for their review of provider profiles.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.