
Abstract
Objective:
Technology-based programs can be cost-effective in the management of chronic obstructive pulmonary disease (COPD). However, cost-effectiveness estimates always contain some uncertainty, and decisions based upon them carry some risk. We conducted a value of information (VOI) analysis to estimate the value of additional research of a web-based self-management intervention for COPD to reduce the costs associated with uncertainty.
Methods:
We used a 10,000-iteration cost-effectiveness model from the health care payer perspective to calculate the expected value of perfect information (EVPI) at the patient- and population-level. An opportunity loss was incurred when the web-based intervention did not produce a greater net monetary benefit than usual care in an iteration. We calculated the probability of opportunity loss and magnitude of opportunity costs as a function of baseline health utility. We aggregated opportunity costs over the projected incident population of inpatient COPD patients over 10 years and estimated it as a function of the willingness-to-pay (WTP) threshold. Costs are in 2022 U.S. Dollars.
Results:
Opportunity losses were found in 22.7% of the iterations. The EVPIpatient was $78 per patient (95% confidence interval: $75–$82). The probability that the intervention was the optimal strategy varied across baseline health utilities. The EVPIpopulation was $506,666,882 over 10 years for a WTP of $50,000.
Conclusions:
Research estimated to cost up to $500 million would be warranted to reduce uncertainty. Future research could focus on identifying the impact of baseline health utilities to maximize the cost savings of the intervention. Other considerations for future research priorities include implementation efforts for technology-based interventions.
Introduction
TECHNOLOGY AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Chronic obstructive pulmonary disease (COPD) has an estimated worldwide prevalence of 13% 1 and cited as the third leading global cause of death. 2 COPD is both preventable and treatable, 3 but poses an enormous economic burden on society. 4 The Centers for Disease Control and Prevention estimated the annual cost for the management of COPD in the United States (U.S.) in 2020 to be $49 billion. 5 Limiting disease progression and preventing COPD exacerbations may reduce the cost of management of COPD. Therefore, research and development of innovative and cost-effective technologies to promote disease self-management and improve outcomes in COPD are of paramount importance. 6
Technology-based interventions and programs, particularly during the COVID-19 era, are emerging as alternatives or complements to usual management performed during outpatient clinic visits. 6 Remote support for COPD self-management interventions, including physical activity, has been shown to be both low-cost and effective. 7 –10 Over several randomized controlled trials, we evaluated the effectiveness of a pedometer-based, web-mediated self-management intervention focused on promoting physical activity in patients with COPD. 11 –15 This multicomponent intervention, based on the theory of self-regulation, supports behavior change through: (1) iterative feedback; (2) personalized daily step count goals; (3) motivational messages; (4) educational tips; and (5) an online forum for social support. This intervention significantly improves daily step counts compared to a pedometer alone 12,15 and usual care. 14 Our analyses show a reduced risk of acute exacerbations 13 and improvements to health-related quality of life (HRQoL). 12,15
Promising results from this technology-based self-management intervention are aligned with other reviews and meta-analyses that suggest technology can be leveraged to support self-management behaviors (e.g., physical activity) and other relevant clinical outcomes (e.g., HRQoL) in patients with COPD. 16 –22
VALUE OF INFORMATION ANALYSIS
As new technologies are developed, policy and decision makers must determine the payoffs associated with adopting each one. These payoffs are typically estimated through cost-effectiveness analyses, 23 which inherently incorporate some level of uncertainty. 24 As such, there is always risk that decisions on technology adoption based on existing information will be incorrect. 25,26 Adopting a suboptimal strategy may lead to negative consequences for patient care and the health care system. 27 For example, previous research may support the effectiveness of an intervention, but does not guarantee that it is effective for the entirety of the patient sample. If money is spent on an intervention that is not cost-effective for that patient, it is an opportunity loss. Additional information could better inform decisions by reducing uncertainty; however, obtaining additional information comes with a cost. Therefore, assessing the need and value of additional research is recommended. 26
Value of information (VOI) analyses quantify the expected value of research in reducing uncertainty around its cost-effectiveness to inform whether collecting additional evidence is worthwhile. A VOI analysis is informed by how cost-effective the technology appears given prior information, the uncertainty surrounding cost-effectiveness, and consequences of decision error based on current, imperfect information. VOI analyses identify the strategy (e.g., intervention) with the maximum expected net benefit in cost and health effects, and can inform the cost-effectiveness of additional research. VOI analyses are recommended by the International Society for Pharmacoeconomics and Outcomes Research 27,28 and are growing in popularity, particularly in health care. 29 Use of VOI analysis to assess the return on investment of further research incorporates the potential future impact of interventions on a population level. 30
CURRENT STUDY
Numerous studies have evaluated the effectiveness of technology-based self-management interventions for COPD 17,19 –22 and their cost-effectiveness, 6,8,9,31 but none, to our knowledge, has evaluated the VOI. The current analysis aimed to estimate the value of additional research for a web-based self-management intervention for COPD to reduce uncertainty in the cost-effectiveness. Given the burden of this disease and the uncertainty in the cost-effectiveness, 21,22 we expect the aggregated opportunity costs to be substantial.
Methods
ANALYTIC STEPS
We begin by summarizing the analytic steps for this VOI analysis, which include the following: (1) identify the underlying cost-effectiveness model, accompanying parameters, and corresponding probabilistic parameters; (2) calculate the expected value of perfect information (EVPI) at the patient level; (3) calculate the EVPI at the population level; and (4) evaluate the EVPI as a function of the willingness-to-pay (WTP) threshold.
All analyses were completed with Microsoft Excel and SAS 9.4 (Cary, NC). the model and article were created in accordance with the Consolidated Health Economic Evaluation Reporting Standards. 32 The VA Bedford Healthcare System Institutional Review Board reviewed and determined that this analysis of retrospective deidentified and existing published data was not human subjects research and therefore did not require a HIPAA waiver of authorization.
COST-EFFECTIVENESS MODEL
We developed a cost-effectiveness model from the health care payer perspective using data from a recent randomized controlled trial, 11,15 published literature, 33,34 and the National Inpatient Sample. 35,36 The National Inpatient Sample was chosen as hospitalizations are the major cost-driving factor in COPD; In addition, applying the VOI to an inpatient sample, as opposed to outpatient care, offers a more conservative estimate of the incident population. An earlier study presented a cost-effectiveness model based on a single-loop Monte Carlo Simulation (MCS) 27 with 10,000 iterations and compared three strategies: (1) website+pedometer (i.e., web-based self-management intervention); (2) pedometer alone; and (3) usual care. 8 The website+pedometer and pedometer-alone were preferred strategies that maximized cost-effectiveness. 8 For the current VOI analysis, we compared the website+pedometer to usual care. The relevant model parameters, probabilistic distributions, and assumptions from the cost-effectiveness model are presented in Table 1. Usual care was based on previously published literature. 33,34
Overview of the Cost-Effectiveness Analysis Model Parameters from the Previous Publication 8
SD, standard deviation; SGRQ-TS, St. George's Respiratory Questionnaire-Total Score.
PATIENT-LEVEL EVPI
From the cost-effectiveness model, we calculated the net monetary benefit (NMB) for each iteration by group (website+pedometer or usual care). The NMB is a metric that incorporates the cost of the strategy (C) and effectiveness (ΔE; change in health utilities at 12 months from baseline) relative to society's WTP for new technologies (WTP; λ). A WTP of $50,000 USD was used, as it is a widely used benchmark for assessing the cost-effectiveness of an intervention.
We calculated net benefit observed for each strategy for all 10,000 simulations using a single-loop Monte Carlo scheme for computing the EVPI 27 —this represents net benefits under perfect information, where we would always choose the group with the greatest net benefit. In each iteration, we identified which strategy yielded the greatest net benefit, and calculated the opportunity loss that would be averted if there was perfect information predicting patient benefit from the intervention. The EVPI at the patient-level (EVPIpatient ) is calculated as the difference between the maximum expected NMB given perfect information and the maximum expected NMB given current information. The expected NMB with perfect information is the mean NMB when the simulation with the higher NMB is chosen.
The expected NMB with current information is calculated as the mean NMB for the website+pedometer across all simulated iterations, even in simulated iterations where the web-based intervention yielded an opportunity loss. Table 2 displays a select sample of the MCS iterations to further illustrate this analysis.
Sample Monte Carlo Simulation Output and Calculations
λ, Willingness-to-Pay Threshold; MCS, Monte Carlo Simulation; NMB, net monetary benefit.
With the MCS iterations, we examined the association between baseline health utility score and opportunity losses (i.e., when the website+pedometer was not the optimal strategy) and opportunity gains (i.e., when the website+pedometer was the optimal strategy). The utility values represent a preference-based HRQoL measure. 37
POPULATION-LEVEL EVPI
The EVPI at the population level (EVPIpopulation
) is the EVPIpatient
totaled over the incident population (I) summed for the anticipated life-time usefulness of the intervention (T), modified by a discount rate (r) compounded over time (t).
First, we calculated the incident population (I), that is, the estimated number of patients who are eligible per year across the expected lifetime of the intervention. The incident population was calculated using the Healthcare Cost and Utilization Project (HCUP) Clinical Classification Software (CCS) code for COPD (127). 38 We used the HCUP Nationwide Inpatient Sample 35 data from calendar years 1993 to 2011 and the National Inpatient Sample 36 data from 2011 to 2014 to determine the annual total of U.S. patients admitted to the hospital with COPD as the primary diagnosis. We estimated an annual growth rate from 1993 to 2014 using linear regression of log-transformed annual COPD inpatient numbers. This growth rate was then extrapolated to a population beginning in 2021 with the last cohort ending in 2030, resulting in 10 cohorts of patients (Table 3).
Value of Information Parameters
θ, uncertain parameters; j, strategy decision (0 = usual care, 1 = website+pedometer); .
We assumed the lifetime usefulness of technology (T) at 10 years, a reasonable estimate from a policymaker perspective. 30 We used a discount rate (r) of 2% from 2021 to 2030, which reflects the mean rate of return on a relatively safe investment. 39 Discounting was applied under the assumption that the current value of a service will likely depreciate over time and that future populations would prefer future technology, compared to current technology. We then estimated the EVPIpopulation as a function of the WTP threshold. All costs were inflated to 2022 dollars using the Consumer Price Index (inflation rate = 1.18). 40
Results
PATIENT-LEVEL OPPORTUNITY LOSSES
Using a WTP threshold of $50,000, the mean NMB with perfect information (where the optimal strategy, i.e., the strategy that yielded the higher NMB, was always chosen) was $39,447 (95% confidence interval [CI]: $39,137–$39,756). Within iterations where the website+pedometer was the optimal strategy, the mean NMB was $2,086 (95% CI: $2,054–$2,118). The website+pedometer was not the optimal strategy in 22.7% of iterations. Among iterations where the website+pedometer was not the optimal strategy, the mean opportunity loss was $346 (95% CI: $339–$353). The EVPIpatient (i.e., the mean maximum net benefit for each iteration if all opportunity losses were avoided) was $78 (95% CI: $75–$82).
We examined the relationship between baseline health utilities and the probability of selecting the optimal strategy (i.e., avoiding an opportunity loss). As evident in Figure 1, the opportunity losses and gains vary as a function of baseline health utility. When health utilities are low (≤0.3), usual care is more likely to be the optimal strategy. The probability that the intervention is the optimal strategy increases as health utilities increase from about 0.5 to 0.7, then the probability begins to decrease again. When health utilities are high (≥0.9), there is less of a difference between probability of optimal strategy selection.
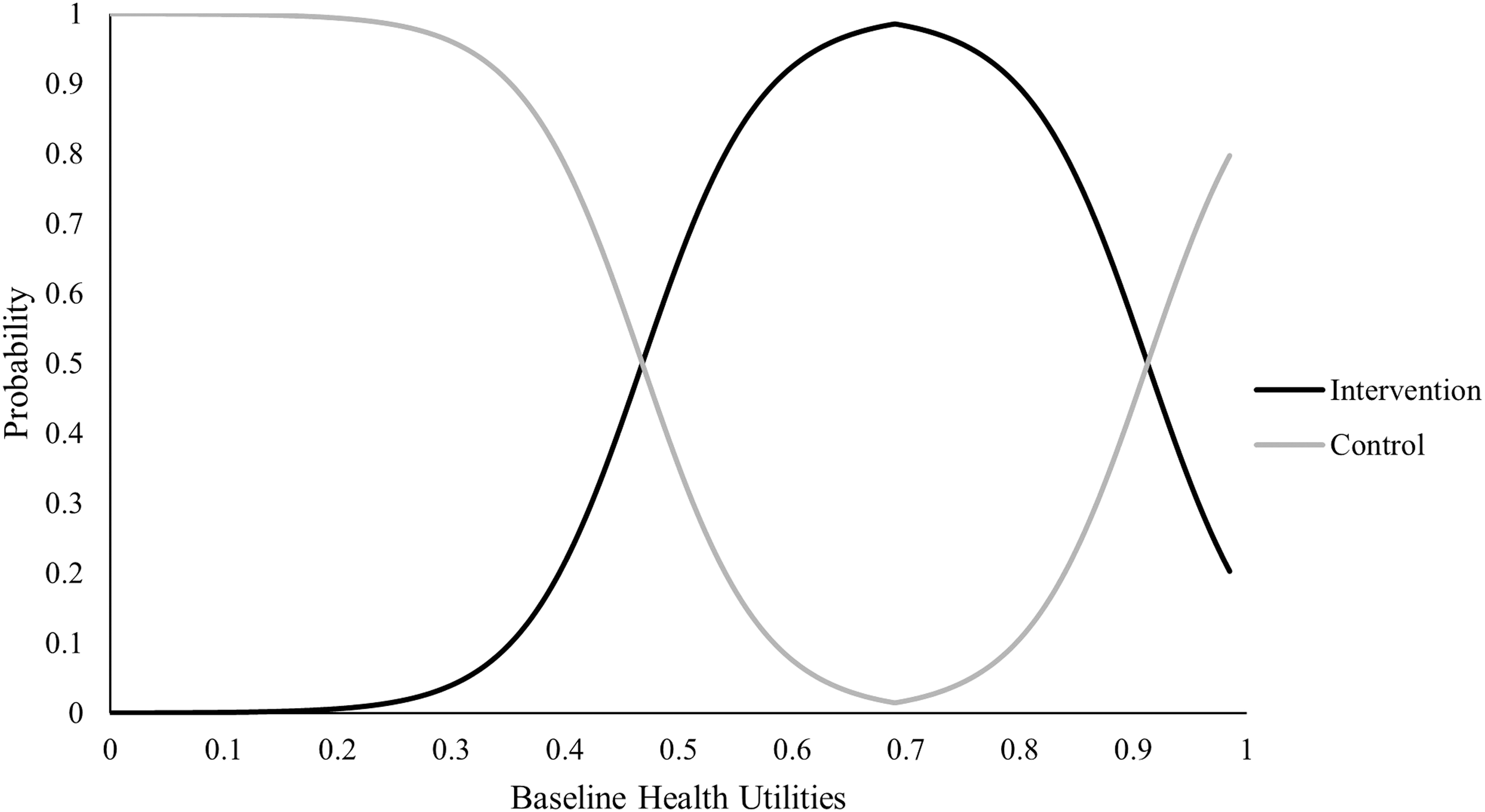
Probability of optimal strategy selection across baseline health utilities (range 0.0–1.0, where 1.0 represents perfect health).
POPULATION-LEVEL OPPORTUNITY LOSSES
In the United States, the proportion of patients with COPD increased by 1.6% per year from 1993 to 2014, 35,36 (β = 0.016, p < 0.001). We used this mean annual growth rate to extrapolate to a population beginning in 2021 and ending in 2030. Across this 10-year period, we applied a 2% discount rate, corresponding to an incident population of 658,818 in 2021 and 633,642 in 2030 (Table 4). Summed across the 10 years, this equated to 6,461,575 individuals with COPD during the 10-year period. The population-level EVPI for patients diagnosed with COPD (for WTP = $50,000) is calculated as $506,666,882. Figure 2 presents the overall EVPI as a function of the WTP. The population-level EVPI peaked at $1,081,927,915 for WTP of $12,000. The EVPI was $697,809,852 for WTP of $10,000, and $397,729,891 for WTP of $100,000.

EVPI as a function of willingness-to-pay threshold (λ). EVPI, expected value of perfect information.
Annual Predicted Incident Population of Patients Admitted to an Inpatient Stay with Chronic Obstructive Pulmonary Disease for Estimation of Population-Level Expected Value of Perfect Information
Predicted population using mean annual growth rate from 1993 to 2014 from HCUP NIS for COPD and bronchiectasis, extrapolated to 2021.
Predicted population as a function of the expected lifetime of the technology (10 years with a 2% discount rate).
COPD, chronic obstructive pulmonary disease; HCUP, Healthcare Cost and Utilization Project.
SENSITIVITY ANALYSIS
To further understand the influence of baseline health utilities on the patient- and population-level opportunity losses, we calculated the VOI using only iterations of the MCS where baseline health utilities fell within one standard deviation of the mean (0.53–0.85). This range represented patients for whom the intervention would likely yield a higher net benefit compared to usual care based on current information. Using a WTP threshold of $50,000, the mean NMB with perfect information was $38,164 (95% CI: $37,973–$38,355). The EVPIpatient was $2.06 (95% CI: $1.77–$2.35). The population-level EVPI (for WTP = $50,000) is calculated as $13,295,377. The population-level EVPI peaked at $964,030,366 for WTP of $13,000. The EVPI was $637,845,514 for WTP of $10,000, and $363,552,085 for WTP of $100,000.
Discussion
This analysis aimed to evaluate the uncertainty regarding the cost-effectiveness of a web-based self-management intervention for COPD and assess the EVPI associated with perfect selection of patients to benefit from the intervention. Some uncertainty is inherent in decision-making to adopt a new technology. If the decision based on current information is incorrect, there will be opportunity loss. Given the growing interest in technology-based interventions for COPD management, 6 applying a VOI approach provides novel economic information to aid in the decision to support future research from a population-level perspective. This conclusion is specific to this web-based self-management intervention, but these methods and identification of the VOI can be extrapolated and applied to other technology-based interventions.
Previous work supports that the web-based intervention is effective in promoting physical activity and other health outcomes, 11 –15 cost-effective, 8 and cost-saving. 9 Results of the patient-level EVPI analysis show that about 23% of the simulated iterations represented an opportunity loss under the strategy of the web-based intervention. This supports that the intervention is not always the most cost-effective strategy compared to usual care. This percentage is similar to earlier work within the realm of pulmonary rehabilitation, the standard of care for COPD. 10 An earlier study found that the probability of center-based pulmonary rehabilitation being cost-effective compared home-based pulmonary rehabilitation was 19% at a WTP of $50,000/Quality-Adjusted Life Year (QALY). 41 While effective for many patients, there is a chance that it may not be cost-effective for all patients. The current analysis addresses the value of additional research to reduce the uncertainty of the intervention's cost-effectiveness.
The probability that the intervention is the optimal strategy varied by baseline health utilities. The web-based intervention may be the optimal strategy for patients with baseline health utilities ranging from 0.5 to 0.9. The estimated health utility in COPD is ∼0.67, ranging from 0.82 (stage I—mild COPD) to 0.62 (stage IV—severe COPD). 42 This suggests that the intervention may be optimal within the average clinical range of health utilities for patients with COPD. Sensitivity analysis further supported the benefit of selecting the intervention for patients within this range, as the EVPI declined substantially at both the patient- and population-levels. Opportunity losses could be reduced, and in doing so, optimize the cost-effectiveness of the web-based intervention, by further evaluating and modifying the intervention for patients with lower health utilities.
Conversely, future research could evaluate the intervention in patients with higher health utilities (i.e., healthier), where the intervention may be less useful. For example, research that seeks to explore if increasing the intensity of the intervention by adding an additional exercise training component is cost-effective may be a fruitful line of future research. These findings are in line with an earlier VOI analysis concerning bronchodilators in COPD, which also found that it would be most beneficial to collect additional information on the role of utilities. 43 Patients with lower health utilities, a correlate of worse disease severity, 44 are in greater need of self-management interventions. 45 However, disease severity is also associated with lower activation for self-management. 46 Therefore, future research should continue to understand how health utilities impact patient activation and engagement with technology-based self-management interventions.
The population EVPI provides an estimated limit on returns to further research. Despite an unlimited number of research questions and topics, funding for medical research is limited. VOI analyses can aid in the decision-making process regarding which research topics would benefit the most from additional research and create the greatest return on investment—that is, which research topics have the highest VOI. If the cost of future research exceeds the EVPI, then the proposed research is not cost-effective. However, the potential additional value provided by each distinct research study requires future consideration in its relative contribution to the overall VOI. The National Institute for Health and Clinical Excellence (NICE) developed a VOI-based framework to inform decisions. 47
As outlined in the NICE framework, when the technology is cost-effective, deciding to adopt the intervention with further research would be appropriate if additional research is possible and would fall below the EVPI. 47 In the current analysis, the EVPI for the choice between the web-based self-management intervention and usual care was over 500 million USD at the population level over 10 years at a WTP of $50,000/QALY. This suggests that further research to remove uncertainty and enable more robust economic decisions to be made would be worth up to 500 million USD. Research that can be conducted at an estimated cost lower than this value would be warranted to reduce uncertainty regarding the cost-effectiveness of the intervention.
LIMITATIONS AND FUTURE DIRECTIONS
VOI analyses can only provide information about the values of eliminating uncertainty around the probabilistic parameters included in the model. Some sources of uncertainty not included in the original cost-effectiveness model may not have been considered. Patient characteristics, such as comorbidities, distance to care, and comfort with technology, are not included in this analysis, and may influence which strategy (intervention or usual care) is a better option for the patient. 48,49 Our model is also limited in our use of secondary data sources. As specified in our previous description of our cost-effectiveness model, 8 we converted the St. George's Respiratory Questionnaire-Total Score (SGRQ-TS) to health utilities via a validated crosswalk using utilities from the EuroQoL-5 (EQ-5D). While the EQ-5D is widely used to assess heath utilities across a wide range of health conditions, 50 it does not necessarily reflect other outcomes specific to COPD.
Our population was estimated using the CCS codes, which aggregates the International Classification of Diseases, 10th Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) codes into clinically meaningful categories. The CCS code for COPD includes bronchiectasis, although the discharge-weighted number of bronchiectasis discharges (where bronchiectasis was the primary diagnostic code) made up <2% of the discharges. As this code is not specific to only COPD, it may therefore not be a true reflection of hospitalizations only in COPD.
In addition, our model does not consider the VOI concerning implementation efforts. Implementation is a critical step in translating evidence-based interventions from research to clinical practice. VOI analyses and other economic evaluations can be used to support decision-making regarding whether future research should be conducted or if an intervention should be implemented, but the best ways, or strategies, to support this implementation remains a priority for future work. Along with implementation of the intervention, there remain substantial barriers to implementing VOI work into the decision-making process. A recent stakeholder-informed evaluation suggested that future VOI work should focus on supporting decision-makers and researcher knowledge of VOI analyses and supporting stakeholder buy-in of VOI analyses (e.g., citing other success stories). 51
Conclusion
In summary, we applied a VOI approach to estimate the value of additional research to reduce the uncertainty in the cost-effectiveness of a web-based self-management intervention for COPD. The VOI analysis indicates that there is uncertainty regarding the choice between the web-based intervention and usual care. The EVPI suggests that further research should focus on the cost-effectiveness of the intervention relative to baseline patient health utilities. Moreover, the extent of the uncertainty and VOI depends on the maximum WTP. Future work would benefit from further parameter identification and addressing barriers to implementation of the intervention.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The primary trial of this secondary analysis was supported by the Department of Veterans Affairs, Health Services Research and Development Service (Grant IIR 09-366). This secondary analysis was supported by the National Heart, Lung, and Blood Institute (K12HL138049).